北京大学学报(医学版) ›› 2020, Vol. 52 ›› Issue (3): 582-585. doi: 10.19723/j.issn.1671-167X.2020.03.028
内含终丝的骶管囊肿21例临床研究
林国中,王振宇( ),谢京城,刘彬,马长城,陈晓东
),谢京城,刘彬,马长城,陈晓东
- 北京大学第三医院神经外科,北京 100191
Clinical study of 21 cases of sacral cysts containing fila terminale
Guo-zhong LIN,Zhen-yu WANG(),Jing-cheng XIE,Bin LIU,Chang-cheng MA,Xiao-dong CHEN
- Department of Neurosurgery, Peking University Third Hospital, Beijing 100191, China
摘要:
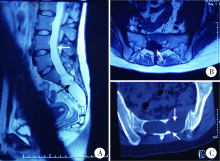
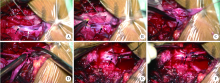
目的 总结内含终丝的骶管囊肿的特点,探讨其手术治疗方法。方法 回顾分析2010年7月至2017年3月收治的21例内含终丝的骶管囊肿患者的临床特点、影像学特征和手术方法。临床症状以腰骶部及会阴区疼痛、双下肢无力和二便功能障碍为主。磁共振成像表现为骶管内长T1、长T2囊性信号,囊内可见终丝信号,增强扫描无强化,均合并脊髓低位。手术包括囊壁切除、终丝切断、脊髓拴系松解和终池重建等主要步骤。结果 囊壁全切除14例,次全切除7例。21例均将终丝分离切除,彻底松解拴系,并全部完成终池重建。术后除7例有轻度肛周麻木感外,无其他新发神经功能障碍。病理检查证实囊壁和终丝符合脊膜囊肿和终丝结构。术后患者腰骶部及会阴区疼痛消失、双下肢无力及大小便功能障碍逐渐恢复。视觉模拟疼痛评分从术前(5.24±1.41)分降到术后的(2.01±1.33)分;运动障碍者手术后肌力提高1~2级;括约肌障碍者日本骨科协会(Japanese Orthopaedic Association,JOA)评分从(2.09±0.99)分上升到(2.78±0.52)分。随访3个月至7年,平均2.25年,所有患者脊髓功能达到McCormick分级Ⅰ级,仅1例囊肿复发。结论 内含终丝的骶管囊肿罕见,以腰骶部及会阴区疼痛和脊髓拴系症状为主要表现。磁共振成像有助于该病的诊断,表现为囊肿内脑脊液信号和终丝结构,伴有脊髓圆锥低位。手术应在显微镜下切除囊壁,切断终丝并松解脊髓拴系和重建终池。
中图分类号:
- R651.2


| [1] | 陈晓东, 王振宇, 谢京城, 等. 症状性骶管内囊肿的诊断与治疗[J]. 中国脊柱脊髓杂志, 2006,16(2):138-141. |
| [2] | Sun J, Wang Z, Li Z, et al. Reconstruction of nerve root sheaths for sacralextradural spinal meningeal cysts with spinal nerve root fibers[J]. Sci China Life Sci, 2013,56(11):1007-1013. |
| [3] |
Nabors MW, Pait TG, Byrd EB, et al. Updated assessment and current classification of spinal meningeal cysts[J]. J Neurosurg, 1988,68(3):366-377.
pmid: 3343608 |
| [4] | 谢京城, 王振宇, 陈晓东. 骶管终丝脊膜囊肿合并脊髓拴系综合征的诊断和治疗[J]. 中国临床神经外科杂志, 2015,20(11):651-653. |
| [5] | Hukuda S, Mochizuki T, Ogata M, et al. Operations for cervical spondylotic myelopathy. A comparison of the results of anterior and posterior procedures[J]. J Bone Joint Surg Br, 1985,67(4):609-615. |
| [6] | Selcuki M, Mete M, Barutcuoglu M, et al. Tethered cord syndrome in adults: Experience of 56 patients[J]. Turk Neurosurg, 2015,25(6):922-929. |
| [7] | 汪寒松. MRI在诊断骶管囊肿中的应用[J]. 中国当代医药, 2014,21(2):127-128. |
| [8] | Lee GY, Paradiso G, Tator CH, et al. Surgical management of tethered cord syndrome in adults: indications, techniques, and long-term outcomes in 60 patients[J]. J Neurosurg Spine, 2006,4(2):123-131. |
| [9] | Sun JJ, Wang ZY, Liu B, et al. Neck transfixion for sacralextradural spinal meningeal cysts without spinal nerve root fibers[J]. Eur Spine J, 2016,25(6):1945-1952. |
| [10] | 林国中, 王振宇, 刘斌. 神经电生理监测技术在椎管内病变术中的应用[J]. 北京大学学报(医学版), 2012,44(5):776-779. |
| [1] | 林国中, 马长城, 王振宇, 谢京城, 刘彬, 陈晓东. 颈1~2硬膜外神经鞘瘤的显微微创治疗[J]. 北京大学学报(医学版), 2021, 53(3): 586-589. |
| [2] | 陈立华,杨艺,魏群,李运军,李文德,高进宝,于斌,赵浩,徐如祥. 颞下-乙状窦后联合锁孔入路显微手术治疗岩斜区脑膜瘤[J]. 北京大学学报(医学版), 2016, 48(4): 738-742. |
| [3] | 段鸿洲, 李良, 张扬, 张家湧, 鲍圣德. 床突旁动脉瘤的外科治疗[J]. 北京大学学报(医学版), 2015, 47(4): 679-684. |
| [4] | 彭靖, 龙海, 袁亦铭, 崔万寿, 张志超, 潘文博. 显微镜下和腹腔镜下精索静脉结扎术的疗效比较[J]. 北京大学学报(医学版), 2014, 46(4): 541-543. |
| [5] | 彭靖,袁亦铭,宋卫东,崔万寿,张志超,李俊杰,高冰,辛钟成. 输精管结扎术后患者行显微镜下输精管复通术的疗效[J]. 北京大学学报(医学版), 2013, 45(4): 597-. |
| [6] | 赵连明, 姜辉, 洪锴, 黄锦, 唐文豪, 毛加明, 乔杰, 刘平, 廉颖, 马潞林. 非嵌合型克氏综合征患者显微取精成功3例报告[J]. 北京大学学报(医学版), 2012, 44(4): 547-550. |
| [7] | 樊东升, 张俊, 邓敏, 康德瑄, 郑菊阳, 徐迎胜, 鲁明, 傅瑜, 沈扬, 张英爽, 张华纲. 肌萎缩侧索硬化/运动神经元病的基础与临床研究[J]. 北京大学学报(医学版), 2009, 41(3): 279-281. |
| [8] | 杨朝晖, 彭歆, 谢秋菲. 面神经离断损伤神经电图诊断评价[J]. 北京大学学报(医学版), 2008, 40(6): 639-641. |
| [9] | 周崇阳, 杨朝晖, 冯海兰. 咬合重建对咀嚼肌肌电图协同模式的近、远期影响[J]. 北京大学学报(医学版), 2008, 40(3): 323-326. |
| [10] | 刘小璇, 樊东升, 张俊, 郑菊阳, 马铁民. 比较不同方式移植的人间充质干细胞在大鼠失神经支配的骨骼肌的分布及对坐骨神经损伤的影响[J]. 北京大学学报(医学版), 2008, 40(2): 185-191. |
| [11] | 毛驰, 俞光岩, 彭歆, 张雷, 郭传瑸, 黄敏娴, 张益, 马大权. 头颈部游离复合组织瓣移植的临床研究[J]. 北京大学学报(医学版), 2008, 40(1): 64-67. |
| [12] | 刘波, 梁冶矢, 石祥恩, 张庆俊. 视神经胶质瘤7例的诊断与治疗[J]. 北京大学学报(医学版), 2005, 37(6): 645-647. |
| [13] | 王振宇, 谢京城, 马长成, 刘彬, 陈晓东, 李振东, 孙建军. 枕下扩大外侧入路手术切除枕大孔区脑膜瘤[J]. 北京大学学报(医学版), 2004, 36(6): 634-636. |
| [14] | 鲍圣德, 王象昌, 张建国, 尤玉才, 霍惟扬, 张彦芳, 葛为勇. 后颅底肿瘤的显微外科手术治疗[J]. 北京大学学报(医学版), 2001, 33(1): 32-34. |
| [15] | 尤玉才, 张晓华, 张彦芳, 王象昌. 脑动静脉畸形治疗方法的选择——附61例分析[J]. 北京大学学报(医学版), 2001, 33(1): 29-31. |
|
