北京大学学报(医学版) ›› 2022, Vol. 54 ›› Issue (5): 991-999. doi: 10.19723/j.issn.1671-167X.2022.05.028
三维超声血管斑块定量分析技术评估颈动脉粥样硬化斑块
邢海英1,2,陈玉辉3,许珂1,2,黄点点1,2,彭清1,2,刘冉1,2,孙葳1,2,黄一宁1,2,*( )
)
- 1. 北京大学第一医院神经内科, 北京 100034
2. 神经系统小血管病探索北京市重点实验室, 北京 100034
3. 北京医院神经内科, 北京 100730
Evaluation of carotid atherosclerotic plaques by vascular plaque quantification (VPQ) technology of three-dimensional ultrasonography
Hai-ying XING1,2,Yu-hui CHEN3,Ke XU1,2,Dian-dian HUANG1,2,Qing PENG1,2,Ran LIU1,2,Wei SUN1,2,Yi-ning HUANG1,2,*()
- 1. Department of Neurology, Peking University First Hospital, Beijing 100034, China
2. Department of Neurology, Beijing Key Laboratory of Neurovascular Disease Discovery, Beijing, China
3. Department of Neurology, Beijing Hospital, Beijing 100730, China
摘要:
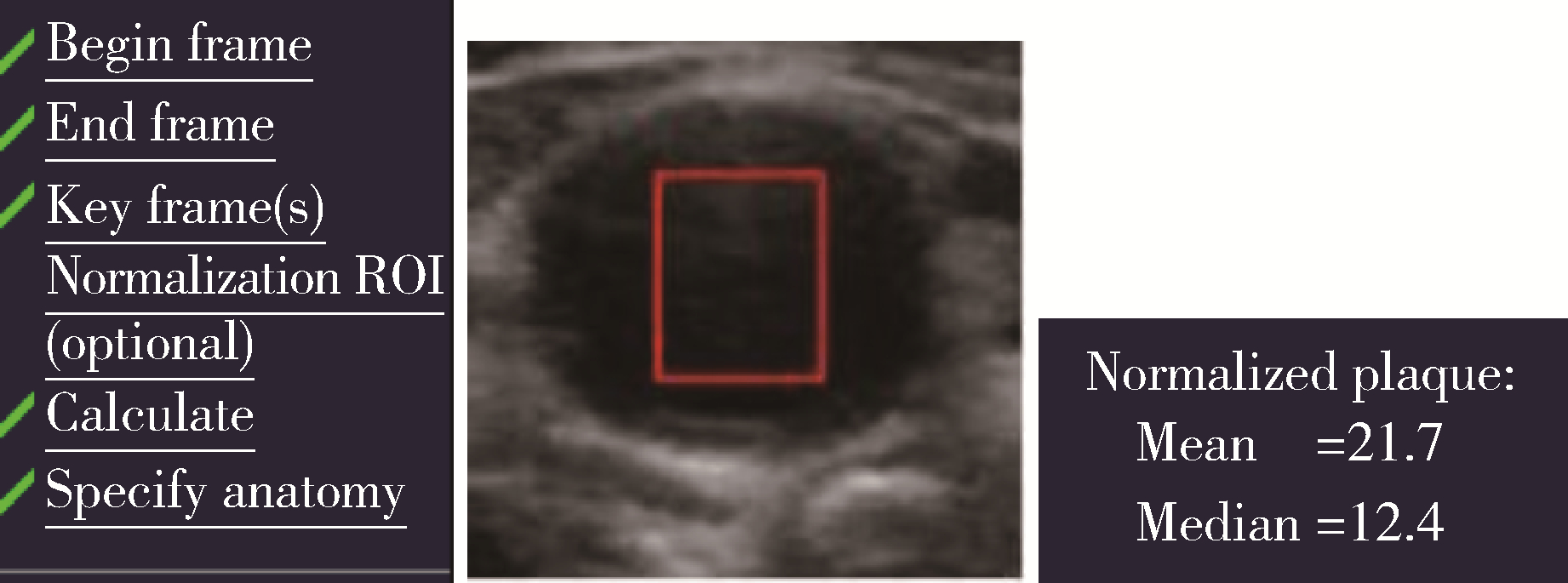
目的: 分析应用三维超声血管斑块定量分析技术(vascular plaque quantification, VPQ)评估颈动脉粥样硬化斑块的可行性并观察他汀类药物对颈动脉粥样硬化斑块的影响。方法: 选择2016年1月至2018年9月于北京大学第一医院神经内科治疗的颈动脉粥样硬化患者, 采用三维超声检查患者的双侧颈动脉, 对存在颈动脉粥样硬化斑块的患者采用VPQ测量颈动脉斑块的灰阶中位数(gray scale median, GSM)及其他血管参数。根据斑块的GSM, 分为低GSM组(GSM < 40)和高GSM组(GSM≥40), 比较两组患者的临床特征和斑块特征, 分析斑块的稳定性。根据患者是否服用他汀类药物, 将患者分为他汀组和非他汀组, 比较两组患者在3个月和2年时颈动脉斑块GSM及其他血管参数的变化。结果: 共入组120例患者, 其中男性79例, 女性41例, 平均年龄(65.39±9.11)岁。低GSM组31例, 高GSM组89例。低GSM组管腔的狭窄程度更重(面积狭窄率41.32%±21.37% vs. 29.79%±17.16%, P < 0.05)。低GSM组的标准化管壁指数(normalized wall index, NWI)显著大于高GSM组(0.61±0.14 vs.0.52±0.12, P < 0.01), 观察了77例患者颈动脉粥样硬化斑块的变化, 其中男51例, 女26例, 年龄(64.96±9.58)岁, 根据是否服用他汀类药物分为他汀组(n=56)和非他汀组(n=21)。与基线相比, 3个月随访时两组患者的颈动脉斑块体积、面积、管腔狭窄度、GSM变化差异均无统计学意义(P >0.05); 2年随访时, 他汀组的GSM增加[中位数10.00(2.00, 28.00)], 而非他汀组的GSM减低[中位数-7.00 (-11.00, 5.50)], 组间差异有统计学意义(P < 0.01)。他汀组的颈动脉斑块体积无明显增加, 而非他汀组的斑块体积略增加, 但两组的变化值差异无统计学意义[他汀组斑块体积增加[中位数0.00 (-30.00, 40.00) mm3, 非他汀组为30.00 (10.00, 70.00) mm3, P>0.05]。结论: 三维超声(three dimensional ultrasound, 3DUS)的VPQ可测量颈动脉斑块的GSM, 低GSM(GSM < 40)组患者的血管狭窄程度更重, 标准化管壁指数更高。VPQ观察到颈动脉粥样硬化斑块的患者服用中强度他汀类药物治疗2年后斑块的灰阶中位数增加, 提示3DUS的VPQ技术可用来观察他汀类药物治疗颈动脉动脉粥样硬化斑块的效果。
中图分类号:
- R543.4

| 1 |
Lal BK , Hobson RW , Pappas PJ , et al. Pixel distribution analysis of B-mode ultrasound scan images predicts histologic features of atherosclerotic carotid plaques[J]. J Vasc Surg, 2002, 35 (6): 1210- 1217.
doi: 10.1067/mva.2002.122888 |
| 2 |
Herr JE , Hetu MF , Li TY , et al. Presence of calcium-like tissue composition in carotid plaque is indicative of significant coronary artery disease in high-risk patients[J]. J Am Soc Echocardiogr, 2019, 32 (5): 633- 642.
doi: 10.1016/j.echo.2019.01.001 |
| 3 |
Mujaj B , Bos D , Selwaness M , et al. Statin use is associated with carotid plaque composition: The Rotterdam study[J]. Int J Cardiol, 2018, 260, 213- 218.
doi: 10.1016/j.ijcard.2018.02.111 |
| 4 |
Vergallo R , Crea F . Atherosclerotic plaque healing[J]. N Engl J Med, 2020, 383 (9): 846- 857.
doi: 10.1056/NEJMra2000317 |
| 5 |
Touboul PJ , Hennerici MG , Meairs S , et al. Mannheim carotid intima-media thickness and plaque consensus (2004-2006-2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011[J]. Cerebrovasc Dis, 2012, 34 (4): 290- 296.
doi: 10.1159/000343145 |
| 6 |
中国成人血脂异常防治指南修订联合委员会. 中国成人血脂异常防治指南(2016年修订版)[J]. 中华心血管病杂志, 2016, 44 (10): 833- 853.
doi: 10.3760/cma.j.issn.0253-3758.2016.10.005 |
| 7 | Geroulakos G , Ramaswami G , Nicolaides A , et al. Characterization of symptomatic and asymptomatic carotid plaques using high-resolution real-time ultrasonography[J]. Br J Surg, 1993, 80 (10): 1274- 1277. |
| 8 |
Johri AM , Herr JE , Li TY , et al. Novel ultrasound methods to investigate carotid artery plaque vulnerability[J]. J Am Soc Echocardiogr, 2017, 30 (2): 139- 148.
doi: 10.1016/j.echo.2016.11.003 |
| 9 |
el-Barghouty N , Geroulakos G , Nicolaides A , et al. Computer-assisted carotid plaque characterisation[J]. Eur J Vasc Endovasc Surg, 1995, 9 (4): 389- 393.
doi: 10.1016/S1078-5884(05)80005-X |
| 10 |
Spanos K , Tzorbatzoglou I , Lazari P , et al. Carotid artery plaque echomorphology and its association with histopathologic characteristics[J]. J Vasc Surg, 2018, 68 (6): 1772- 1780.
doi: 10.1016/j.jvs.2018.01.068 |
| 11 |
Mathiesen EB , Bonaa KH , Joakimsen O . Echolucent plaques are associated with high risk of ischemic cerebrovascular events in carotid stenosis: The tromso study[J]. Circulation, 2001, 103 (17): 2171- 2175.
doi: 10.1161/01.CIR.103.17.2171 |
| 12 |
Hashimoto H , Tagaya M , Niki H , et al. Computer-assisted analysis of heterogeneity on B-mode imaging predicts instability of asymptomatic carotid plaque[J]. Cerebrovasc Dis, 2009, 28 (4): 357- 364.
doi: 10.1159/000229554 |
| 13 |
Huibers A , de Borst GJ , Bulbulia R , et al. Plaque echolucency and the risk of ischaemic stroke in patients with asymptomatic carotid stenosis within the first asymptomatic carotid surgery trial (ACST-1)[J]. Eur J Vasc Endovasc Surg, 2016, 51 (5): 616- 621.
doi: 10.1016/j.ejvs.2015.11.013 |
| 14 |
Zhang M , Zhao Q , Gao Y , et al. Prediction for rupture risk of carotid artery plaques: A comparative study of 3D-GSM and CAS system[J]. Eur J Radiol, 2016, 85 (9): 1659- 1665.
doi: 10.1016/j.ejrad.2016.05.013 |
| 15 |
王秀玲, 张敏郁, 丁桂春, 等. 三维超声灰阶中位数定量评价颈动脉斑块的易损性[J]. 中华医学超声杂志: 电子版, 2017, 14 (1): 23- 28.
doi: 10.3877/cma.j.issn.1672-6448.2017.01.008 |
| 16 |
Urbak L , Sandholt BV , Graebe M , et al. Patients with unstable atherosclerosis have more echolucent carotid plaques compared with stable atherosclerotic patients: A 3-D ultrasound study[J]. Ultrasound Med Biol, 2020, 46 (9): 2164- 2172.
doi: 10.1016/j.ultrasmedbio.2020.04.002 |
| 17 |
Nicolaides AN , Kakkos SK , Kyriacou E , et al. Asymptomatic internal carotid artery stenosis and cerebrovascular risk stratification[J]. J Vasc Surg, 2010, 52 (6): 1486- 1496.
doi: 10.1016/j.jvs.2010.07.021 |
| 18 |
Ruiz-Ares G , Fuentes B , Martinez-Sanchez P , et al. A prediction model for unstable carotid atheromatous plaque in acute ischemic stroke patients: Proposal and internal validation[J]. Ultrasound Med Biol, 2014, 40 (9): 1958- 1965.
doi: 10.1016/j.ultrasmedbio.2014.04.015 |
| 19 |
Biasi GM , Froio A , Diethrich EB , et al. Carotid plaque echolucency increases the risk of stroke in carotid stenting: The imaging in carotid angioplasty and risk of stroke (ICAROS) study[J]. Circulation, 2004, 110 (6): 756- 762.
doi: 10.1161/01.CIR.0000138103.91187.E3 |
| 20 |
Ariyoshi K , Okuya S , Kunitsugu I , et al. Ultrasound analysis of gray-scale median value of carotid plaques is a useful reference index for cerebro-cardiovascular events in patients with type 2 diabetes[J]. J Diabetes Investig, 2015, 6 (1): 91- 97.
doi: 10.1111/jdi.12242 |
| 21 |
国家卫生健康委员会脑卒中防治专家委员会血管超声专业委员会, 中国超声医学工程学会浅表器官及外周血管超声专业委员会, 中国超声医学工程学会颅脑及颈部血管超声专业委员会, 中国超声医学工程学会颅脑及颈部血管超声专业委员会. 头颈部血管超声若干问题的专家共识(颈动脉部分)[J]. 中国脑血管病杂志, 2020, 17 (6): 346- 352.
doi: 10.3969/j.issn.1672-5921.2020.06.013 |
| 22 |
Kadoglou NP , Gerasimidis T , Moumtzouoglou A , et al. Intensive lipid-lowering therapy ameliorates novel calcification markers and GSM score in patients with carotid stenosis[J]. Eur J Vasc Endovasc Surg, 2008, 35 (6): 661- 668.
doi: 10.1016/j.ejvs.2007.12.011 |
| 23 |
Yamaguchi M , Sasaki M , Ohba H , et al. Quantitative assessment of changes in carotid plaques during cilostazol administration using three-dimensional ultrasonography and non-gated magnetic resonance plaque imaging[J]. Neuroradiology, 2012, 54 (9): 939- 945.
doi: 10.1007/s00234-012-1011-2 |
| [1] | 巩超, 刘秋萍, 王佳敏, 刘晓非, 张明露, 杨瀚, 沈鹏, 林鸿波, 唐迅, 高培. 社区人群他汀干预策略预防心血管病效果的马尔可夫模型评价[J]. 北京大学学报(医学版), 2022, 54(3): 443-449. |
| [2] | 刘欢,王宏宇,刘金波,赵红薇,周迎燕,李丽红. 颈动脉斑块患者大动脉功能与冠心病和下肢动脉疾病的关系[J]. 北京大学学报(医学版), 2017, 49(6): 1027-1033. |
| [3] | 张静,任景怡,陈红,韩冠平. 他汀类药物可降低不稳定性心绞痛患者血浆中炎症相关microRNAs的表达水平[J]. 北京大学学报(医学版), 2015, 47(5): 761-768. |
| [4] | 欧蒙恩, 张晓, 刘云松, 葛严军, 周永胜. 联合应用基质细胞衍生因子1、辛伐他汀及骨胶原支架进行体内异位成骨[J]. 北京大学学报(医学版), 2015, 47(1): 47-51. |
| [5] | 王艳飞, 贾新未, 赵文萍, 王凤娟, 刘亚宁, 张芳, 张丽敏, 王鸿超. 辛伐他汀后适应对缺血再灌注损伤大鼠TNF-α及NF-κB的影响[J]. 北京大学学报(医学版), 2014, 46(6): 990-992. |
| [6] | 徐璐, 王超, 沈文文, 祁荣. 辛伐他汀纳米脂质体对骨髓间充质干细胞成骨分化的影响[J]. 北京大学学报(医学版), 2014, 46(6): 883-888. |
| [7] | 关静琳, 姜雯 , 王怀宇, 曾辉, 张素敏, 王广, 毛节明. 辛伐他汀对高胆固醇血症患者血管内皮的多重影响[J]. 北京大学学报(医学版), 2014, 46(5): 703-706. |
| [8] | 夏经钢, 曲杨, 胡少东, 许骥, 尹春琳, 徐东. 强化调脂对行非心脏手术的冠状动脉粥样硬化性心脏病患者的心肌保护作用及机制初探[J]. 北京大学学报(医学版), 2014, 46(4): 601-605. |
| [9] | 翟国君, 姚伟娟, 贾子昌, 韩金涛, 赵军, 李选, 董国祥. 静脉人工血管桥内膜增生的形态学特征及洛伐他汀的干预作用[J]. 北京大学学报(医学版), 2012, 44(5): 783-787. |
| [10] | 杨琳, 王莹, 吕天敬, 周利群, 金杰. 临床有效剂量的洛伐他汀对前列腺癌PC3细胞的影响[J]. 北京大学学报(医学版), 2010, 42(4): 391-395. |
| [11] | 宋纯理, 党耕町, 贾弘抖, 郭昭庆, 马庆军. 辛伐他汀促进骨髓基质细胞的成骨分化[J]. 北京大学学报(医学版), 2003, 35(5): 533-536. |
| [12] | 张新超, 张彤, 徐成斌, 金晓峰. 辛伐他汀和西立伐他汀对体外培养血管平滑肌细胞增殖及迁移的影响[J]. 北京大学学报(医学版), 2001, 33(4): 344-346. |
| [13] | 任汉云, 张念先, 徐红, 陆道培. 辛伐他汀选择性抑制慢性髓性白血病细胞增殖并诱导凋亡[J]. 北京大学学报(医学版), 2001, 33(2): 136-139. |
|
||
