
种植体周黏膜炎是可逆性疾病,附着于种植体及其修复体表面的菌斑生物膜是该疾病的始动因素[5],Salvi等[6]通过让受试者停止口腔卫生措施3周,诱导出了实验性种植体周黏膜炎,而在控制菌斑后,龈沟液中的生物标志物含量呈现可逆趋势[7]。这表明,有效地菌斑控制是逆转疾病的关键,这也促使临床医生不断探索更高效、更微创的清创方法。在此背景下,喷砂技术因其清创效率高、作用范围广、患者体验佳等优势[8-9],已被用于种植体周维护。然而,目前关于喷砂技术与传统超声(ultrasonic debridement, US)治疗直接比较的研究仍相对缺乏。因此,本研究旨在比较赤藓糖醇喷砂(erythritol air-polishing, EAP)和US两种方法治疗种植体周黏膜炎的短期临床疗效差异,并评估患者报告的结局。
1 资料与方法
本研究遵守《赫尔辛基宣言》中人体医学研究的伦理准测,经北京大学口腔医学院生医学伦理委员会审批(PKUSSIRC-201946080),并在中国临床试验注册平台进行注册(ChiCTR2000031392),受试者在研究开始前均签署知情同意书。
1.1 研究设计
本研究为单盲、随机对照试验,采用计算机生成的随机数字序列,由1名不参与受试者招募与临床评估的研究人员通过在线随机化网站(www.random.org)生成。分配方案隐藏于不透光的密封信封中,直至受试者签署知情同意书并完成基线测量后依次开启。对结局评估者实施设盲,即所有临床指标的检查与记录均由1名不知晓分组情况且不参与治疗过程的医师完成。所有受试者均由同1名资深牙周专科医师进行治疗。
1.2 研究对象
受试者选自2021年6月至2022年5月就诊于北京大学口腔医院牙周科的患者。纳入标准:年龄18~70岁;口内有至少1颗种植体且负重时间超过1年;目标种植体至少1个位点探诊深度≥4 mm,有探诊出血和/或溢脓,同时影像学检查显示种植体周围骨水平稳定,位于种植体颈部平台或以上;不吸烟或戒烟超过1年。排除标准:影像学检查或探诊检查发现粘接剂残留;已知对氯己定、赤藓糖醇或本研究使用的其他牙科材料过敏;患有未经控制的全身系统性疾病(如未控制的糖尿病);近3个月接受过牙周和种植体维护治疗;3个月内应用免疫抑制剂或抗生素;妊娠期或哺乳期。
1.3 临床指标
主要结局指标:种植体周探诊深度(peri-implant probing depths, PPD),使用牙周探针以0.25 N轻力探诊,记录6个位点(近中颊、颊侧中央、远中颊、近中舌、舌侧中央、远中舌)种植体黏膜边缘到袋底的距离,精确至1 mm。
次要结局指标:改良菌斑指数(modified plaque index, mPLI):记录6个位点,0=无菌斑;1=探针尖划过种植体表面可见菌斑;2=肉眼可见菌斑;3=大量软垢。探诊出血(bleeding on probing, BOP):记录6个位点,探诊检查后记录有无出血,以百分比形式表示阳性位点比例,探诊出血严重程度分级参考改良出血指数(modified sulcus bleeding index, mSBI)[10],即0=不出血,1=点状出血,2=线状出血,3=重度出血。种植体周软组织探诊溢脓(suppuration on probing,SoP):探诊后观察颊舌侧有无溢脓,记录为有或无,计算探诊溢脓种植体数目占总种植体数目的百分比。疼痛视觉模拟评分(visual analogue scale,VAS):治疗结束后,患者为感受的术中疼痛程度打分,0分代表无疼痛,10分代表非常疼痛。此外,作为探索性分析,还计算了PPD≥4 mm位点的比例。
治疗成功标准的判定参考2023年欧洲牙周病学联合会《S3级临床实践指南》[11],即疾病完全缓解=种植体周BOP阴性且无溢脓,疾病部分缓解=种植体周围存在≤1个点状BOP阳性位点,且无溢脓。
1.4 样本量计算
样本量计算参照以往相关研究[12],治疗后两组PPD差值取0.3 mm,标准差取0.3,采用两组独立样本t检验进行比较,设定显著性水平双侧α值取0.05,统计功效(1-β)值取0.8,理论最小样本量为每组16例(总样本量32例);考虑到可能存在10%的失访率,最终每组纳入18例(总样本量36例)。
1.5 干预措施
在受试者完成纳入后,首先由1名不参与治疗操作的研究人员采集其基线期临床指标。随后,对所有受试者进行口腔卫生宣教,并根据其天然牙的牙周状况进行相应的洁治和/或龈下刮治。
EAP组:种植体采用龈下喷砂处理,使用直径14 μm的含氯己定成分的赤藓糖醇砂粉(EMS公司, 瑞士)。具体操作方法如下:将喷砂头插入至距离种植体周袋底约1 mm处,保持操作角度在60°~90°之间,沿冠根方向采用提拉式移动,每个治疗位点持续处理5 s。每次移动喷砂头时均与前一处理区域部分重叠,以确保围绕种植体周缘进行完整、连续的清创。
US组:种植体接受US刮治,采用US工作仪(EMS公司, 瑞士)搭配聚醚醚酮(poly ether-ether-ketone, PEEK)纤维涂层的工作尖进行刮治。
EAP组和US组均使用0.12%(质量分数)氯己定溶液进行种植体周袋冲洗。所有治疗均由同1位资深牙周专科医师完成,且操作在未拆除种植体上部结构、不麻醉的条件下完成。治疗结束后立即请患者对术中疼痛程度进行VAS评分。术后1个月和3个月分别进行随访,期间再次强化口腔卫生宣教,并使用橡皮杯蘸取抛光膏对修复体进行抛光处理。
1.6 统计学分析
采用SPSS 24.0统计软件进行数据分析。连续变量的正态性通过Shapiro-Wilk检验进行评估。符合正态分布的计量资料(PPD、mPLI、BOP、PPD≥4 mm)以均数±标准差表示,组间比较采用独立样本t检验;非正态分布数据(VAS)以M(P25, P75)表示,采用Mann-Whitney U检验进行比较。分类资料采用卡方或Fisher’ s检验。对于临床参数随时间变化的组内比较,符合正态分布者采用重复测量方差分析,不满足条件者采用Friedman检验。对于重复测量数据的组内事后两两比较,采用Bonferroni法对P值进行校正,以控制多重比较带来的Ⅰ类错误风险。所有统计检验均以P<0.05为差异有统计学意义。
1.7 检查者一致性
研究开展前,检查者于同日、间隔1 h对10颗非本研究招募患者的种植体进行探诊检查,若两次探诊深度相差1 mm以内,则认为检查结果一致,检查者自身一致性组内相关系数为0.92(95%CI: 0.88~0.94)。
2 结果
2.1 患者一般情况
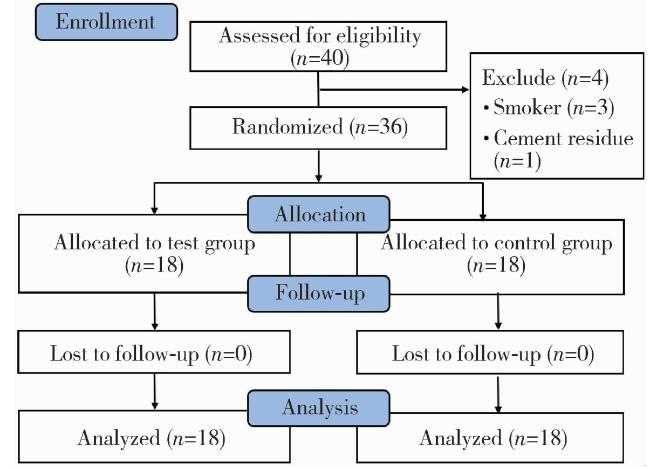
表1 患者一般情况Table 1 Baseline patient characteristics |
| Variable | EAP (n= 18) | US (n= 18) | P value |
| Age/years, ${\bar x}$±s | 51.0±10.5 | 50.1±9.9 | 0.785 |
| Male/female, n | 10 / 8 | 6 / 12 | 0.176 |
| History of periodontitis/% | 66.7 | 83.3 | 0.738 |
| Implant position, n (%) | 0.345 | ||
| Anterior maxilla | 2 (11.1) | 2 (11.1) | |
| Posterior maxilla | 8 (44.4) | 6 (33.3) | |
| Anterior mandible | 4 (22.2) | 1 (5.6) | |
| Posterior mandible | 4 (22.2) | 9 (50.0) | |
| Prosthesis retention, n (%) | 0.705 | ||
| Screw-retained | 12 (66.7) | 13 (72.2) | |
| Cement-retained | 6 (33.3) | 5 (27.8) | |
| Baseline clinical parameters | |||
| Mean PPD/mm, ${\bar x}$±s | 4.0±0.5 | 3.8±0.4 | 0.187 |
| Mean mPLI, ${\bar x}$±s | 1.4±0.7 | 1.5±0.9 | 0.712 |
| Mean BOP/%, ${\bar x}$±s | 85.2±13.9 | 88.0±17.9 | 0.601 |
| SoP/% | 27.8 | 22.2 | 0.700 |
EAP, erythritol air-polishing; US, ultrasonic debridement; PPD, peri-implant probing depth; mPLI, modified plaque index; BOP, bleeding on probing; SoP, suppuration on probing. |
2.2 两组患者临床指标的变化
如表 2所示,EAP组和US组在基线期的各项临床指标差异无统计学意义(P>0.05)。主要结局指标平均PPD均随时间显著改善:EAP组在治疗后1个月(P=0.011)及3个月(P<0.001)均较基线显著下降,US组在治疗后1个月(P=0.038)及3个月(P=0.018)指标亦较基线显著改善,但组间比较差异无统计学意义(P>0.05)。
表2 两组患者临床指标在3个月随访期内的变化Table 2 Changes in clinical parameters over the 3-month experimental period in the two groups |
| Parameters | Baseline | 1 month | P valuea | 3 months | P valueb |
| Mean PPD/mm, ${\bar x}$±s | |||||
| EAP | 4.0±0.5 | 3.7±0.6 | 0.011 | 3.4±0.5 | <0.001 |
| US | 3.8±0.4 | 3.6±0.5 | 0.038 | 3.5±0.4 | 0.018 |
| P valuec | 0.284 | 0.654 | 0.250 | ||
| Mean mPLI, ${\bar x}$±s | |||||
| EAP | 1.4±0.7 | 0.6±0.7 | <0.001 | 0.2±0.2 | <0.001 |
| US | 1.5±0.9 | 0.5±0.6 | <0.001 | 0.3±0.2 | <0.001 |
| P valuec | 0.791 | 0.546 | 0.058 | ||
| PPD≥4 mm sites/%, ${\bar x}$±s | |||||
| EAP | 73.1±24.8 | 53.7±22.8 | <0.001 | 42.6±26.1 | <0.001 |
| US | 62.0±21.4 | 55.6±24.5 | 0.009 | 57.4±25.1 | 0.039 |
| P valuec | 0.081 | 0.785 | 0.029 | ||
| BOP/%, ${\bar x}$±s | |||||
| EAP | 85.2±13.9 | 64.8±31.8 | 0.016 | 53.7±29.5 | <0.001 |
| US | 88.0±17.9 | 70.4±31.1 | 0.012 | 59.2±28.7 | <0.001 |
| P valuec | 0.606 | 0.601 | 0.573 | ||
| SoP/% | |||||
| EAP | 27.8 | 0 | NA | 0 | NA |
| US | 22.2 | 0 | NA | 0 | NA |
| P valuec | 0.700 | NA | NA |
PPD, peri-implant probing depth; EAP, erythritol air-polishing; US, ultrasonic debridement; mPLI, modified plaque index; BOP, bleeding on probing; SoP, suppuration on probing. a, 1 month compared to baseline; b, 3 months compared to baseline; c, comparison between two groups. NA, not applicable (due to zero variance). |
次要结局指标mPLI和BOP在EAP组和US组中,于术后1个月及3个月时均较基线显著改善,但两组间的改善程度在任何时间点差异均无统计学意义(P>0.05),详细的组内比较统计学结果见表 2。此外,治疗前两组分别有27.8%和22.2%的位点存在SoP,在治疗后1个月和3个月两组均未检出SoP。两组疼痛VAS评分均较低,EAP组为1.00(1.00,2.00),US组为2.00(1.00,2.25),组间差异无统计学意义(P > 0.05)。
在针对PPD≥4 mm位点比例的探索性分析中,基线时EAP组为(73.1±24.8)%,US组为(62.0± 21.4)%;治疗后3个月,EAP组显著降低至(42.6±26.1)%,US组降低至(57.4±25.1)%,组间差异具有统计学意义(P=0.029,表 2)。
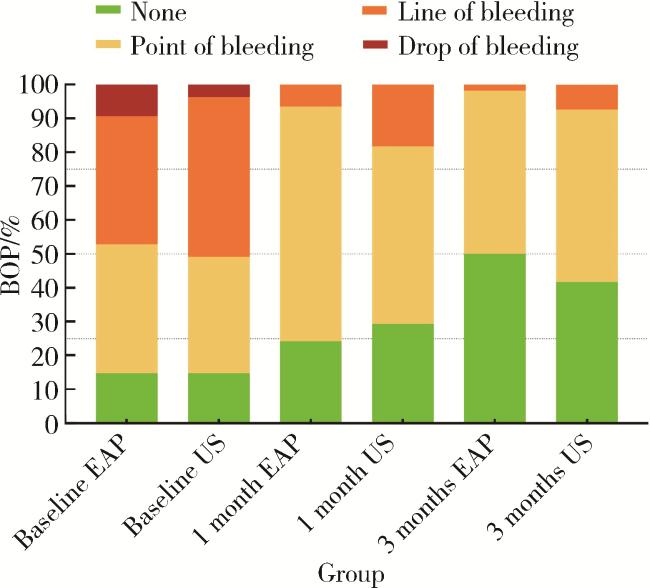
治疗成功率方面,治疗后3个月,种植体水平上EAP组与US组分别有5颗(27.8%)和3颗(16.7%)种植体周围存在≤1个点状BOP阳性位点,且无溢脓,达到可接受的临床治疗终点,其中BOP阴性且无溢脓的种植体数量分别为3颗(16.7%)和2颗(11.1%);位点水平上,EAP组与US组达到BOP阴性的比例分别为50.0%和41.7% (图 2),组间差异无统计学意义(P > 0.05)。研究期间未报告任何不良事件。
{kind=link}
{kind=link}
{kind=link}
{kind=link}
3 讨论
本研究比较了EAP与US对种植体周黏膜炎的短期临床疗效,两组间主要结局指标平均PPD在观察期内展现了相似的改善程度,这可能归因于两种方法均能有效破坏并移除种植体周袋内的生物膜,从而在控制浅、中度袋的炎症方面达到相近的水平。
然而,对减少深袋(PPD ≥ 4 mm)位点比例方面的探索性分析中,在本研究有限的随访期内,EAP组较US组展现出优势,这一优势可能源于喷砂治疗独特的清创机制与喷砂粉的物理特性。在喷砂临床操作中,高速气流携载粉末形成细腻粒子流,更易进入种植体周深袋底部及种植体不规则表面,实现对US器械难以触及区域的有效清洁。除机械清创作用外,本研究使用的赤藓糖醇砂粉中含氯己定成分,体外研究表明,该砂粉具有抑制细菌黏附与生物膜形成的生物学特性[13],从而在清除已有菌斑的同时可抑制其早期再形成,从而在深袋环境中产生了更持久的抗炎效果。值得注意的是,该指标为本研究的次要终点,其临床意义有待在未来以深袋比例作为主要终点的研究中得到专门验证。
在炎症改善方面,本研究两组患者的BOP降幅[EAP组(31.5±24.9)%,US组(28.7±17.0)%]与既往研究结果基本一致,例如,Verket等[14]报道甘氨酸喷砂与US治疗后12个月BOP分别下降了31.8%与35.1%,Riben-Grundstrom等[15]也观察到相似改善趋势。此外,靖无迪等[16]的随机对照试验进一步表明,甘氨酸喷砂对于BOP的改善优于US联合氯己定冲洗。尽管多项研究将BOP阴性作为种植体周黏膜炎完全缓解的理想标准[17-18],但实际临床中达到该目标的难度较大。Nicola等[17]的研究显示,US联合或不联合甘氨酸喷砂治疗种植体周黏膜炎,12个月后BOP阴性患者的比例分别为16%与27%。本研究达到BOP阴性的种植体比例同样较低(EAP组16.7%,US组11.1%),进一步印证了单次非手术治疗虽可有效减轻炎症程度,但难以实现疾病的彻底消除[14]。2023年,欧洲牙周病联合会颁布的《S3级临床实践指南》中修订了种植体周疾病的治疗目标,将“疾病部分缓解”确立为一项更现实的临床治疗终点,即再评估时种植体周存在≤1个BOP阳性位点,且无溢脓[11]。尽管本研究已采纳指南中更为宽松的“部分缓解”标准进行评估,但两组总体达标率仍不理想(EAP组27.8%,US组16.7%)。这一结果强烈提示,对于相当一部分种植体周黏膜炎病例,其炎症状态可能比预想的更为顽固,单次的非手术治疗或许不足以彻底改变其微生态环境或生物膜结构。因此,为实现有效的炎症控制,多数病例需要更强化的治疗方案,例如增加治疗频次、联合疗法或使用局部或全身辅助药物,抑或是采用基于个体风险因素的个性化综合治疗策略。
患者主观感受方面,两组患者报告的术中疼痛程度均较轻,EAP组与US组VAS评分中位数分别为1.00(1.00, 2.00)和2.00(1.00, 2.25),组间差异无统计学意义。该结果提示,两种治疗方式均具备良好的临床耐受性。值得关注的是,这一结果与部分针对天然牙周治疗的研究结论存在差异,例如,Ulvik等[19]的研究显示,在天然牙周治疗中,EAP的主观舒适度显著优于US。这种差异可能源于种植体与天然牙在解剖结构上的本质区别,种植体缺乏牙周膜这一重要的本体感受器结构,其周围黏膜组织中感觉神经末梢的分布密度相对较低,可能导致对机械刺激的整体感知能力下降。
本研究存在以下局限性:(1)3个月的随访期较短,仅能反映治疗的初期抗炎效果,未能捕捉疾病的长期动态演变,因此, 无法回答哪种疗法在预防疾病复发、维持长期稳定性方面更具优势; (2)尽管所有患者均接受了标准的牙周基础治疗与统一的口腔卫生指导,但个体间在长期维护的依从性与效果上可能存在差异,这种全口牙周环境的动态波动,是影响种植体周健康的一个不可忽视的复杂因素; (3)未进行卫生经济学评价。鉴于此,未来研究需要在更大规模、更长周期的试验中验证EAP的疗效与机制,并引入成本-效益分析,重点关注疾病的复发率和维持临床指标稳定所需的维护间隔等。
综上所述,在本研究有限的随访期内,EAP与US均能有效改善种植体周黏膜炎的临床症状,总体疗效相当。尽管主要结局指标无差异,但结合EAP在减少深袋比例方面显示的潜力及微创特性,可为临床医生在处理种植体周深袋时提供一个有价值的治疗选项。