



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
数字化光纤透照法判断龋洞深度
[于江利, 唐仁韬, 冯琳△  , 董艳梅]
, 董艳梅]
, 董艳梅]
|
|


目的 使用DIAGNOcam系统体外研究新型数字化光纤透照法(digital imaging fiber optic transillumination,DIFOTI)判断龋洞深度的准确性。方法 实验采用自身配对设计,选取74颗有1个邻面龋、边缘嵴均未破坏的离体磨牙(66颗)和前磨牙(8颗),在龋洞所对应的牙合面边缘嵴中央做标记点,将离体牙固定在标准牙列模型内,龋洞与另一离体牙的无龋坏牙面相邻接,用黏蜡封闭至釉牙骨质界(cemento-enamel junction,CEJ)上2 mm及邻间隙(模仿牙龈缘及龈乳头),然后将标准牙列模型放入仿头模内,使用DIAGNOcam系统对离体牙进行探照检查,通过系统的探头从牙合面拍摄获取投射照片。使用DIAGNOcam系统软件测量工具,在投射照片上,从标记点起至龋损最深处长度记为 a,延长 a至对侧边缘嵴处的长度记为 b, b为光纤透照摄取图像中牙的宽度,然后在离体牙牙合面上得到自标记点至对侧边缘嵴与光纤透照图中 b平行的线为患牙的实际宽度,其长度记为 c。投射照片上光纤透照所测得的龋坏深度为 d,通过公式 d/a=c/b(数字化光纤测得的龋坏深度/图像中龋损深度=实际牙宽度/图像中牙宽度),推导得出 d=a×c/b,计算出 d值。取出离体牙,去净腐质,测量实际洞深,记为 D,每个样本 d与 D的差值记录为 Δd。结果用SPSS 20.0软件进行一致性检验,并用MedCalc 14.8.1.0软件对 Δd进行Bland-Altman分析。结果 d与 D的相关系数(intraclass correlation coefficient, ICC)为0.951( ICC>75%), P=0.263,两组数据差异无统计学意义,具有良好的一致性,且两组数据之间存在 y=0.23 +0.91 x 函数关系( x为数字化光纤透照法测得龋洞深度, y为实际龋洞深度)。Bland-Altman分析 Δd显示, Δd的均值 Δdmean为0.05 mm,标准差 ΔdSD=0.308,95%置信区间为(-0.55~0.65),这种相差幅度在临床上可以接受,因此可以认为两种测量方式的一致性较好。结论 使用DIAGNOcam系统体外检测牙齿龋坏深度与龋洞去腐后的实际深度基本一致,提示临床上可以使用DIAGNOcam系统来辅助评估龋洞深度。
Objective: To analyze the accuracy of the digital imaging fiber optic transillumination (DIFOTI) on diagnosis of caries lesions depth using DIAGNOcam system.Methods: This experiment adopted self-matching design. Seventy-four extracted teeth (molar: sixty-six, premolar: eight) with one caries lesions in proximity which were not damaged in surface marginal ridge were selected. Dental calculus and dental stains were removed from the extracted teeth for standby application. A sign was marked in the middle of the occlusal surface edge at the side of decay. Then the teeth were fixed in the standard model of dentition and cavities were adjacent with the sound tooth surface. Sticky wax was applied to seal the level of 2 mm beyond cemento-enamel junction (CEJ) in the direction of occlusion and interproximal space to imitate gingival margin and gingival papilla. The standard models of dentition was seated in imitation head mold. The lesions depth degree was looked into and checked with DIAGNOcam system. Besides, the pictures on the occlusal surfaces were recorded and saved. The sign above could be seen on the picture. The measuring tool in DIAGNOcam system was used to measure the depth of the caries from the sign (as starting point) to the deepest point of caries in the pictures and its length was recorded for a. The line a was lengthened to the contralateral edge of occlusal surface in the photo and the length was recorded for b. A line from the marked point on the occlusal surface edge of the extracted teeth was draw parallel to the line b on the corresponding photo and its length was recorded for c. The depth of the cavities on the projected images was recorded for d, and calculated d/a=c/b (digital optical fiber measured decay depth/caries damage depth of the image = actual tooth width/tooth width of the image), and d=c/b×a inferred. At last, the teeth were taken out from the standard model dentition. The decay of the tooth was removed completely. The actual depth of the cavity was recorded for D. The difference between d and D was recorded for Δd. The software of SPSS 20.0 was used to test the consistency of the results, and the MedCalc 14.8.1.0 software was used for Bland-Altman analysis.Results: The intraclass correlation coefficient ( ICC) between d and D was 0.951 ( ICC>75%), P=0.263. There was a function relationship y=0.23 +0.91 x between d( x) and D( y). Bland-Altman analysis method showed that the mean of Δd ( Δdmean) was 0.05 mm, the standard deviation of Δd ( ΔdSD)=0.308, and the 95% confidence interval was (-0.55 to 0.65). The amplitude of difference was clinically acceptable. So the consistency of the two measurement modes was high.Conclusion: There was no significant difference between the depth of caries lesions checked with DIAGNOcam system and the depth of the actual cavity, and the consistency was very good. The vitro study suggests that the DIAGNOcam system may be used to assess the depth of caries cavity as a useful tool in diagnosis and treatment.
龋病是一种常见病、多发病, 世界卫生组织将其列为危害人类的三大疾病之一[1], 龋损患牙的检查、诊断、治疗对其预后有重要的意义。由于部位隐蔽, 邻面龋的准确检出是临床的难题之一, 同时, 邻面龋由于其特殊的部位, 龋损发展容易累及牙髓。发现龋损后, 龋洞深度的判断可以辅助诊断及评价预后, 对于深龋损, 采用适宜的方法预先采取防护措施可以提高活髓保存的概率, 提高疗效。目前较为普遍的方法是拍摄X线咬合翼片或根尖平片, 根据龋损的深度不同, 咬合翼片发现邻面龋的概率为39%~91%, 但拍摄X线片检查, 患者需接受电离辐射。
光纤透照对于邻面龋损的检出与咬合翼片的一致率可高达95%[2, 3, 4, 5], 与X线片相比, 光纤透照具有无电离辐射、可重复测量的优点。由于使用便利性和有效性等方面的原因, 以往的光纤透照技术并没有在临床广泛应用。随着技术的发展, 数字化摄取照片与光纤透照法相结合的新型数字化光纤透照技术(digital imaging fiber optic transillumination, DIFOTI, 商品名为DIAGNOcam)能够在去腐之前, 用无创、无辐射的方法, 反复、多次检查并摄取检测图像, 通过所获取的数据信息评估洞深。Ye等[6]的研究表明, DIFOTI诊断系统对龋损诊断非常有价值。
本研究采用DIFOTI方法对于龋损深度进行评估, 以期为临床上龋病的诊断、治疗提供参考。
3个月内拔除的离体磨牙或前磨牙。纳入标准:有1个邻面龋, 龋损牙合方位于釉牙骨质界上, 边缘嵴未破坏。排除标准:龋损累及牙合面, 龋损牙合方位于釉牙骨质界下, 隐裂。将样本去除牙石及色素, 浸泡备用。
本研究使用的器材有标准牙列模型(日进齿科材料有限公司, 图1)、黏蜡[贺利氏(中国)投资有限公司]、DIAGNOcam(KaVo, 德国)、仿头模(A-DEC, 41 L, 美国, 图2)、游标卡尺(广州百威狮工具有限公司)、20# K锉(Dentsply, 德国)。
 | 图1 标准牙列模型Figure 1 Standard model of dentition |
 | 图2 仿头模Figure 2 Imitation head mold |
将离体牙固定在标准牙列模型内, 龋洞与另一无龋坏离体牙的牙面相邻接, 黏蜡封闭牙龈缘及邻间隙, 模仿龈乳头形态至釉牙骨质界上2 mm, 然后将标准牙列模型放入仿头模内检测。
DIAGNOcam数字化光纤透照仪的组成有光纤透照探头、数字化摄像头、图像处理系统(cam系统)。光纤透照探头由两个近红外光放射头端组成, 可夹持于待测牙的颊舌面。数字化摄像头位于牙合面部位, 摄取照片。
DIAGNOcam系统检测过程:将DIAGNOcam光纤透照探头对置于仿头模内的离体牙模拟临床透照过程进行探照检查, 通过系统的探头从牙合面拍摄获取投射结果照片。
离体牙事先在龋损侧边缘嵴中央做一牙面标记点, 使用DIAGNOcam系统软件测量工具, 在投射照片上, 以图像中的牙面标记点为起点, 至照片所示龋损最深处作为图像中龋损深度, 其长度记录为a, 从标记点至a线终点的延长线至对侧边缘嵴处作标记线, 为光纤透照摄取的图像中牙宽度, 其长度记录为b, 然后在离体牙牙合面上得到自标记点至对侧边缘嵴与光纤透照图中标记线平行的线为患牙的实际宽度, 其长度记录为c。投射照片上所指示的深度所代表的光纤透照所测得的龋坏深度为d, 通过公式d/a=c/b(光纤测得龋坏深度/图像中龋损深度=实际牙宽度/图像中牙宽度), 推导得出d=a× c/b, 计算出d值(图3)。
使用慢速手机和钨钢球钻, 依照临床去腐过程及去腐标准将离体牙龋洞内腐质去除干净(若有露髓孔, 其直径< 1 mm), 测量用20# K锉沿c的方向, 进入去净腐质的窝洞内, 锉尖抵于窝洞最深点, 用制动片指示标记点所在平行于牙长轴的平面, 为实际洞深的长度记录。用游标卡尺测量K锉记录的长度, 得到龋洞的实际深度D(有露髓孔的龋洞, 以露髓孔边缘为龋洞最深处)。
比较数字化光纤透照检测所测得的龋坏深度d与去腐后龋洞的实际深度D。
用SPSS 20.0统计软件进行一致性检验, 并用MedCalc 14.8.1.0软件对Δ d进行Bland-Altman分析, 数据以均数± 标准差(最小值, 最大值)表示, P< 0.05为差异有统计学意义。
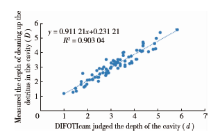
实验数据用SPSS 2.0软件进行一致性检验结果显示, DIFOTI所得龋坏深度d与去腐后龋洞的实际深度D的相关系数(intraclass correlation coefficient, ICC)为0.951(ICC> 75%), F=1.27, P=0.263, 关系方程为y=0.23+0.91x(x为DIFOTI测得的龋洞深度, y为实际龋洞深度, 表1、图4)。用MedCalc 14.8.1.0软件对结果进行Bland-Altman分析显示, DIFOTI所得龋坏深度d与去腐后龋洞实际深度D的差值Δ d的均值Δ dmean为0.05 mm, 标准差Δ dSD=0.308, 95%置信区间为-0.55~0.65, 这种相差幅度在临床上可以接受, 因此可以认为两种测量方式的一致性较好(图5)。
| 表1 数字化光纤透照法测得的龋洞深度(d)与去腐后龋洞的实际深度(D) Table 1 DIFOTIcam judged the depth of the cavity (d) and measured the depth of cleaning up the detritus in the cavity (D) |
DIFOTI的原理是利用龋齿病变区的光学性质不同于周围的正常牙体组织, 腐坏的组织会增加光的散射并吸收光子, 从而使龋齿病变区出现阴影[6, 7, 8]。
DIFOTI检测过程中, 环境光线是影响实验结果的重要因素, 为使实验过程尽量模拟临床, 本实验中将离体牙固定于塑料牙列中, 邻牙也为离体牙, 放置于仿头模内, 用软蜡模仿牙龈的光学性质, 仿头模模仿口内的光强度, 从而保证了在检测过程中患牙的环境光线尽量接近临床。
龋洞深度的评估对临床治疗及风险评估有重要的指导意义。Marthaler[9]早在1965年就在龋的临床试验报告中阐述了测量龋深度的意义, 此后多项研究也对釉质龋坏的诊断及深度进行了分析[10, 11, 12]。Ismail[13]提出应用视诊及探诊或两者结合的方法来评估龋洞深度。近年来随着数字技术的发展, DIFOTI技术再次受到关注[14], DIAGNOcam系统是其中的代表。
DIAGNOcam系统定量测量龋洞深度的原理是将数字成像与光纤透照法相结合, 使光纤透照收到的定性信息可被摄像头摄取记录, 采集的图像可以存储并可重复测量, 与先前获得的图像进行对比, 降低了医生的主观性、学习背景、诊疗经验不同等造成的对结果的不同判读。DIFOTI这一技术最大的特点是无创、无辐射, 更加有利于孕妇、儿童[8]。
 | 图3 DIAGNOcam检测、测量及龋洞去腐的实验过程Figure 3 Experimental process of the DIAGNOcam detection, measurement, and cleaning up the detritus |
 | 图4 数字化光纤透照法测得的龋洞深度(d)与实测龋洞深度(D)的散点图及对应函数曲线Figure 4 A scatter diagram and the corresponding function curve of the DIFOTIcam judged the depth of the cavity (d) and measured the depth of cleaning up the detritus in the cavity (D) |
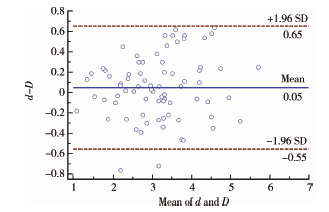 | 图5 数字化光纤透照法测得龋洞深度(d)与实测龋洞深度(D)结果的Bland-Altman分析Figure 5 Bland-Altman plot of the DIFOTIcam judged the depth of the cavity (d) and measured the depth of cleaning up the detritus in the cavity (D) |
光纤透照所采用的光源对于龋损辨别的敏感性非常重要, DIAGNOcam系统所采用的光源为波长780 nm的近红外光。
以往研究表明, 近红外光对于龋损的诊断有较高的灵敏性。Wua等[4]的研究显示, 采用不同光谱探照牙齿反射成像图像的对比度研究中, 近红外光谱的分辨率最高。Staninec等[5]的研究结果显示, 近红外光谱成像对于筛查邻近的龋损病变很敏感, 是避免电离辐射的理想替代工具。Young等[15]的研究表明, 数字成像与光纤透照法相结合在诊断龋坏的初期表现比传统的X线投照技术更加敏感, Ye等[6]的进一步研究也表明DIFOTI系统在诊断累及牙本质中层以内的龋洞时, 敏感性高于X线片, 当龋损超过牙本质中1/2时, 其诊断的敏感性与X线片差异无统计学意义。作为安全性更好、技术敏感性更低、而检测敏感性更高的检测技术, 光纤透照技术受到了越来越多的关注[16, 17]。
综上所述, 准确判断龋损深度对于临床诊断、治疗、预后评估有重要的意义。本研究表明, DIFOTI技术可以用于测量龋损的深度, 其与龋洞完全去净腐质后的实际洞深有很好的一致性, 临床中实际应用DIFOTI技术对于龋病诊治的作用有待进一步研究。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|