



{kind=link}
{kind=link}
{kind=link}
{kind=link}
术中CT引导下寰枢椎复位、固定
[王圣林 , 杨钟玮, 闫明, 刘忠军]
, 杨钟玮, 闫明, 刘忠军]
, 杨钟玮, 闫明, 刘忠军]
|
|


目的 探讨术中CT引导下寰枢椎复位、固定手术的临床疗效。方法 选择2015年1月至8月北京大学第三医院骨科行术中CT引导下寰枢椎复位、固定术的16例患者进行回顾性分析,其中男7例,女9例,年龄26~68岁,平均49.9岁。16例中12例为陈旧性寰枢关节不稳定或脱位,4例为C2齿突新鲜骨折、脱位。16例中14例进行了寰枢椎植骨融合术,2例仅寰枢椎固定、未进行植骨。术中CT使用时机:(1)在术中置钉前CT扫描评估寰枢椎复位情况;(2)术中寰枢椎椎弓根穿刺过程中,CT扫描引导穿刺方向(其中2例患者联合使用3D打印个体化导板和术中CT引导寰枢椎置钉);(3)置钉完成后应用多平面CT重建图像评估螺钉位置及寰枢关节复位情况。计算术中CT扫描的次数,将同期实施徒手寰枢椎内固定的19例作为对照组,比较两种术式的置钉准确性。结果 本组11例术中CT扫描1次、4例2次、1例3次,平均1.4次。16例中CT扫描发现2例寰椎螺钉位置不佳,在术中进行了修正,未出现神经、血管损伤及伤口感染病例。所有病例获得随访,随访时间3~10个月,平均6.7个月。16例术后寰枢关节均获得解剖复位。术后3个月复查CT见寰枢融合良好(14例),齿突骨折骨性愈合(2例)。11例术前合并脊髓病患者脊髓功能改善,平均JOA评分由12.1分提高至14.4分。至最后一次随访均未发现断钉、断棒、内固定松动等并发症发生。置钉准确性比较,发现16例CT组所有寰枢椎螺钉位置均满意,而徒手置钉组19例中有2例4枚的螺钉位置不佳(10.5%)。结论 应用术中CT引导下寰枢椎复位、固定术提高了寰枢椎置钉的准确性,判断寰枢关节复位程度更加精确,术中即刻了解螺钉位置,一定程度上避免返修,显示该术式临床效果良好。
Objective: To evaluate the clinical result of atlantoaxial reduction and fixation guided by the intraoperative CT.Methods: Sixteen cases were retrospectively studied, including seven males and nine females, with the mean age of 49.9 years. Twelve cases were diagnosed as chronic atlantoaxial instability or dislocation, while four cases as acute odontoid fracture and dislocation. Among the sixteen cases, fourteen underwent atlantoaxial fusion, while two underwent temporary atlantoaxial fixation without fusion. The intraoperative CT was used in the setting of: 1. Evaluating the atlantoaxial reduction before the screw insertion; 2. Guiding the C1 and C2 pedicle drilling (two cases using additional three-dimensional printing drilling template);3. Evaluating the position of the screws and reduction after the atlantoaxial fixation. In addition, three-dimensional drilling template combined with intraoperative CT was used in two cases. CT scanning frequency was calculated. To evaluate the accuracy rate of screw fixation under the intraoperative CT, 19 cases without the intraoperative CT were studied as the control group.Results: Averaged CT scanning frequency was 1.4 times (Once in eleven cases, twice in four and three times in one). Among the sixteen cases, mal-positioned C1 screws were found and revised in two cases. No spinal cord injury or vertebral artery injury occurred. The follow-up ranged from three to ten months, with the mean of 6.7 months. Fourteen cases achieved solid osseous fusion, and two with temporary fixation had odontoid fracture union. Anatomic reduction was achieved in all the cases. Eleven cases with preoperative myelopathy had postoperative improvement and their mean JOA scores improved from 12.1 to 14.4. To the last follow-up, no hardware complications were found including screw broken, rod broken or fixation loosening. All the screws of intraoperative CT group had good positions. For 19 cases of the control group, there were two cases of mal-positioned screws (10.5%).Conclusion: Advantages of atlantoaxial reduction and fixation guided by the intraoperative CT included: improving the accuracy of the atlantoaxial screws, exactly evaluating the reduction of the atlantoaxial joint, immediately discovering the mal-positioned screws and avoiding the revision surgery. A good clinical result was found in the preliminary study.
寰枢关节不稳定或脱位会对延脊髓造成压迫, 严重者会致瘫甚至致死[1, 2]。此类疾患首选手术治疗, 对寰枢关节不稳定或脱位实施复位、固定术[2, 3, 4], 文献报告的绝大多数此类手术为徒手操作, 术中使用普通C臂透视检验螺钉位置, 但其二维图像对螺钉位置的判断欠精确、效果不可靠。近来, 有研究应用术中CT指导脊柱内固定手术[5], 可以及时发现螺钉位置不良, 避免因置钉失误或减压不充分导致的二次手术。术中CT引导下置钉更加精确, 在脊柱畸形内固定术方面具有优势[6, 7], 但寰枢椎手术应用术中CT的报道目前尚少见。本研究报告一组术中CT引导下寰枢椎复位、固定手术病例资料, 供借鉴。
选择2015年1月至8月, 于北京大学第三医院骨科行手术治疗的寰枢关节不稳定或骨折脱位患者16例, 实施术中CT引导下后路寰枢椎复位、固定术作为病例组, 对其病历资料进行回顾性分析, 其中男7例, 女9例, 年龄26~68岁, 平均49.9岁。术前诊断陈旧性寰枢关节不稳定或脱位12例, 齿突新鲜骨折、脱位4例。合并颈脊髓病11例(JOA评分9~16分, 平均12.1分), 合并寰椎枕骨化畸形4例, 合并颈2~3先天分节不全(Klippel-Feil综合征, KFS)2例, 合并强直性脊柱炎1例, 合并类风湿关节炎1例。
选择徒手置钉手术患者19例作为对照组, 其中男性10例, 女性9例; 年龄 9~63岁, 平均46.8岁(表1)。对照组入组标准:(1)寰枢椎不稳定或骨折脱位; (2) 与CT引导组相同时间段、同一术者徒手实施的寰枢椎内固定术。排除标准:(1)寰枢椎区骨质破坏者; (2)失访或资料不全者。
病例组16例患者均使用全身麻醉, 在颅骨牵引下或Mayfield头架固定下施行手术(CT扫描时机1:全身麻醉后Mayfield头架固定或颅骨牵引, CT扫描评估寰枢椎复位情况, 即齿突下移程度、寰齿前间隙, 图1)。
手术方式包括寰椎侧块螺钉、枢椎椎弓根螺钉固定术和枢椎椎弓根螺钉固定、枕颈固定术。
1.2.1 寰椎侧块螺钉、枢椎椎弓根螺钉固定术 在寰椎后弓下方探查侧块的内缘, 在后弓的表面相当于侧块中心的位置磨开一孔, 用手锥或手钻向寰椎侧块内钻取钉道(CT扫描时机2:术中寰枢椎椎弓根穿刺过程中, CT扫描引导穿刺方向, 图2)。侧位透视及探查骨壁完整证实钉道位置良好后, 植入直径3.5 mm、长度28~30 mm的螺钉。将C2神经根及血管上挑, 显露出枢椎椎弓根, 在枢椎椎板与侧块交接部磨孔。直视枢椎椎弓根、用手锥向内钻取钉道, 探查无活动出血, 骨壁是否完整后植入直径3.5 mm、长度26~28 mm的螺钉。寰枢螺钉之间用钉板或钉棒固定。本组中2例患者同时使用了3D打印个体化导板结合术中CT引导寰枢椎置钉, 其手术步骤详见后文的典型病例。
1.2.2 枢椎椎弓根螺钉固定、枕颈固定术 同上述方法植入枢椎椎弓根螺钉, 连接枕骨钛板, 用枕骨螺钉固定至枕骨鳞部(CT扫描时机3:置钉完成后应用多平面CT重建图像, 评估螺钉位置及寰枢关节复位情况, 发现螺钉位置不佳时重新置钉, 图3)。
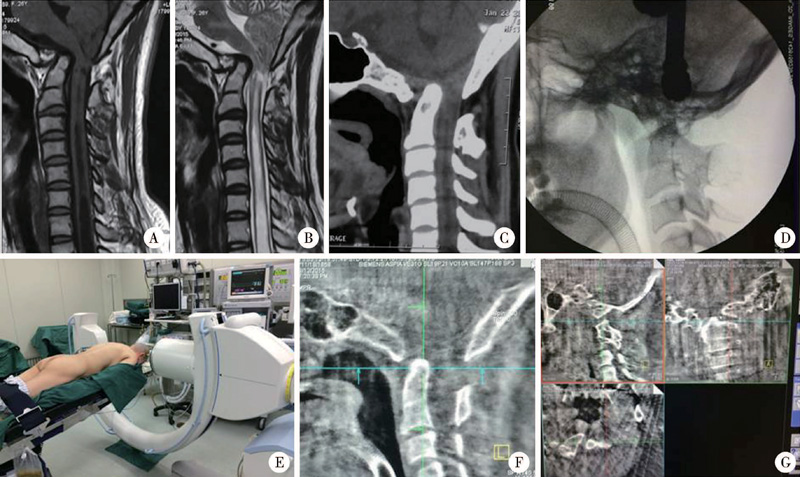 | 图1 应用术中CT评估寰枢椎复位情况Figure 1 The intraoperative CT was used to evaluating the atlantoaxial reduction A and B, preoperative MRI showed the atlantoaxial dislocation, basilar invagination and syringomyelia; C, preoperative CT showed occipitalization and dens dislocation; D, after traction under general anesthesia, the location of the dens and C1 can hardly revealed using the C-arm; E and F, the intrao-perative CT helped the surgeon to judge the complete reduction of C1 and C2; G, in this CT image, we can find the lateral mass joints were fully reduced. A 26 years old female, diagnosed as Atlantoaxial dislocation, occipitalization and basilar invagination. |
 | 图2 术中CT引导寰枢椎置钉方向Figure 2 The intraoperative CT guided the C1 and C2 pedicle drilling direction A and B, radiography showed atlantoaxial dislocation and os odontoideum; C, under the guiding of the intraoperative CT, the unsatisfied drilling direction was modified; D, the fine screw position was achieved using the CT guiding; E, F and G, the repeated CT confirmed all screws were ideally inserted. A 48 years old female, diagnosed as atlantoaxial dislocation and os odontoideum. We modified the driling direction using the intraoperative CT. |
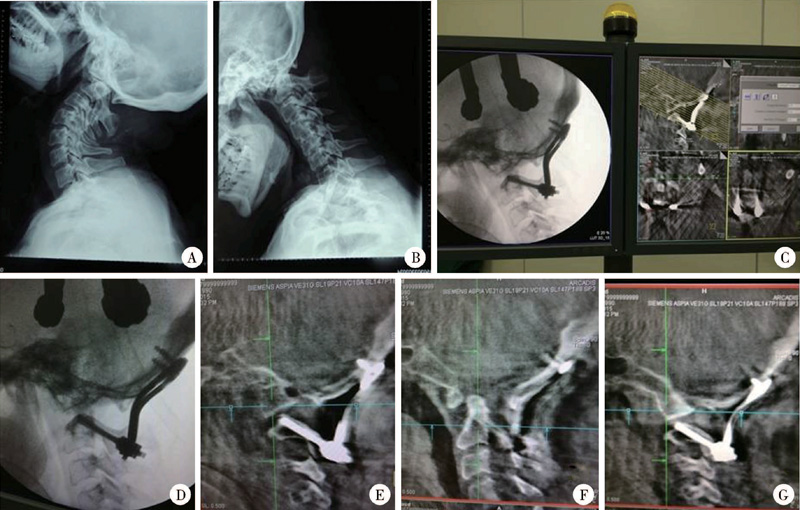 | 图3 置钉完成后应用多平面CT重建图像评估螺钉位置及寰枢关节复位情况Figure 3 Evaluating the position of the screws and reduction after the atlantoaxial fixation A and B, radiography showed the 55 years old lady suffered atlantoaxial dislocation and occipitalization; C and D, C2 pedicle screws and occipitocervical fixation were performed; E, F and G, after the procedure, the intraoperative CT was performed, evaluating the fine position of the C2 screw, the anatomically reduced odontoid and the lateral mass joints. A patient with atlantoaxial dislocation and occipitalization. During the operation, the decompression can be analyzed. |
内固定手术完成后, 取髂后松质骨处理为颗粒状, 置于寰枢椎板间或者颅骨至颈椎椎板之间。16例中14例进行了寰枢椎植骨融合术, 2例齿突骨折的青年患者仅寰枢椎固定, 未进行植骨。术后24~48 h拔除引流管, 鼓励患者下地活动。术后1周拍颈椎X线平片, 术后3个月复查颈椎CT, 了解内固定及植骨融合情况, 术后6个月及12个月复查评估脊髓功能。
术后3个月复查时, 行重建CT检查, 评估螺钉位置:螺钉完全位于C2椎弓根或C1侧块内、未穿破骨壁、未进入椎动脉孔及椎管者, 即认为寰枢椎螺钉位置良好, 否则判为螺钉位置不佳。
采用SPSS16.0软件进行统计学分析, 计量资料以± s表示, 分类数据采用χ 2 检验, 比较并分析病例组(CT引导组)与对照组(徒手组)的性别、年龄、置钉准确率是否存在差异。
16例术中行CT扫描的患者中, 11例实施了寰枢椎固定; 5例实施了枕颈固定(C2至枕骨), 全部病例术中均未出现脊髓及血管损伤。11例术中CT扫描1次, 4例扫描2次, 1例扫描3次, 平均1.4次。16例中CT扫描发现2例的寰椎螺钉位置不佳, 在术中进行了修正。
16例术中CT扫描患者的随访时间3~10个月, 平均6.7个月, 至最后一次随访未发现断钉、断棒、假关节形成等并发症。14例实施植骨融合的患者均获得骨性融合(术后3个月CT评估)。2例新鲜齿突骨折患者术后3个月CT显示骨折愈合, 拆除了内固定, 释放寰枢关节的活动, 所有寰枢关节获得解剖复位。术前有脊髓病者11例, 术后近期脊髓功能有不同程度的改善(术后JOA评分12~16分, 平均14.4分)。
病例组和对照组的年龄及性别组成差异无统计学意义。术后影像学发现CT引导组16例寰枢椎螺钉位置均满意(54枚螺钉, 100%); 而对照组实施徒手置钉的19例患者中(72枚螺钉), 术后CT显示2例患者4枚寰枢椎螺钉位置不佳(1枚C1螺钉偏上进入寰枕关节, 1枚C1螺钉偏外穿出寰椎侧块, 2枚枢椎螺钉偏外、偏上, 部分螺纹突破骨质), 但随访发现此2例骨融合均未受影响。病例组的置钉准确性(100%)高于对照组(89.5%), 但是差异无统计学意义(表1)。
| 表1 临床资料及置钉准确性比较 Table 1 Clinical data and comparison of the screw accuracy |
男性, 61岁, 主因“ 齿突骨折空心钉固定术后颈痛、四肢麻木无力6个月” 入院。患者6个月前因齿突骨折在外院行齿状突空心螺钉固定术, 术后1个月出现颈痛及四肢麻木, 近来麻木逐渐加重并四肢无力(JOA评分12分)。查体双上肢肌力4级, 握拳伸展动作减慢; 下肢肌力4级+, 步态不稳。双膝反射活跃, 双侧Babinski征阳性。影像学显示:齿突螺钉松动移位, 寰椎前移, 颈脊髓受压。手术先行前路螺钉取出, 翻身行后路寰枢椎固定融合术。后路术中使用3D打印个体化导板(术前2 d由术者根据患者CT图像设计个体化置钉的导航通道, 并打印导板), 剥离寰枢椎椎板后, 将导板分别覆盖于寰椎、枢椎的椎板, 沿预制的导引孔向寰椎侧块、枢椎椎弓根穿刺, 并置入合适长度的螺钉(图4A~C)。置钉完成后行术中CT显示螺钉位置满意(图4D、E、H), 寰枢关节解剖复位, 脊髓压迫解除(4F、G)。术后4个月随访时诉四肢无力明显改善, 上肢麻木感部分缓解(JOA评分15分)。
 | 图4 联合使用3D打印个体化导板和术中CT引导寰枢椎置钉Figure 4 Three-dimensional drilling template combined with intraoperative CT were used for C1 and C2 screws insertion A and B, during the posterior procedure, the drilling templates were respectively fixed on the C1 and C2 lamina surface, and the drill was inserted into the predetermined whole; C, C1 screw trajectory was prepared; D and E, the intraoperative CT was performed to evaluate the position of the C1 and C2 screws; F, after the screw-plate fixation, anatomic reduction of C1-C2 joint was achieved; G and H, the dens fracture was also ideally reduced. The male patient with den Fx underwent den’ s screw fixation six monthsago, and suffered the screw loosening. The drill template and intraoperative CT were combined in the operation. |
寰椎侧块螺钉结合枢椎椎弓根螺钉固定术能够坚强固定寰枢关节[8], 在寰枢关节不稳定合并寰椎枕骨化畸形者, 可行枢椎椎弓根至枕骨的固定融合[4]。Wang等[8]对319例寰枢椎螺钉内固定者的术后CT评估显示, 寰枢椎螺钉位置不良率分别为4.5%和7.2%, 可见普通C臂引导下的徒手置钉存在相当的失误率, 在颅椎区畸形者徒手置钉的风险更高。本研究的对照组19例患者中, 术后影像学检查也发现2例患者的4枚螺钉位置不佳, 徒手置钉的失误率与以往学者的经验相当[8]。重建CT为判断螺钉位置的金标准, 但术后重建CT检查即便发现寰枢椎螺钉位置不良, 却无法避免二次手术。
与普通C臂相比, 在寰枢椎手术中应用术中CT的优点包括:(1)由于颅椎区畸形骨组织遮挡, 普通C臂透视下齿突尖部和寰椎关系显示不清, 一般无法准确判断寰枢关节的复位情况; 术中CT清晰显示齿突尖和颅底骨结构, 有助判断寰枢关节是否获得解剖复位。值得一提的是, 术中CT重建图像可以显示寰枢侧块关节张开的程度。若侧块关节张开充分(图1G), 提示行后路复位内固定承受的应力较小, 而侧块关节无法张开时提示寰枢关节脱位严重, 往往需要实施经口寰枢关节松解术[3]。(2)由于牙齿、气管插管及头架的遮挡, 术中应用普通C臂无法显示寰枢椎正位; 而术中CT可以精确指示寰枢椎螺钉内倾及头倾的方向, 穿刺更加安全。(3)植入螺钉后术中CT可即刻判断其位置, 避免干扰椎管、椎动脉或寰枕关节; 本研究病例组即有2例重置了寰椎螺钉, 避免了二次手术; 而对照组的19例有2例4枚螺钉的位置不佳(10.5%), 置钉失误率高于病例组, 但由于本研究的病例数较少, 两组差异无统计学意义。另外, 术中CT可即刻了解寰枢复位、减压情况, 无需等到术后CT检查。
术中CT引导寰枢椎内固定术虽可以增加置钉的准确性, 但是却增加了辐射量。对于不同经验水平的术者和手术难度不同的病例, 何时选择使用术中CT、使用次数等都可能不同。根据本研究病例组16例的经验, 认为可以根据术者经验程度及不同病例的特点择机进行术中CT:颅椎区严重畸形的患者, 若术中穿刺钉道时不顺利可以即刻进行CT扫描, 指导穿刺; 置钉完成后感觉螺钉不牢固或者对寰枢椎复位程度不确定, 可进行扫描确定; 寰枢椎手术的学习曲线较长, 对于经验不足的术者可以适当增加术中CT的扫描次数。
随着近年来数字化骨科技术的发展, 已经有学者将3D打印导板应用至寰枢椎内固定手术中[9, 10], 该技术基于患者的CT图像设计个体化置钉的导航通道, 并使用光敏化树脂打印出导航导板, 在术中引导穿刺置钉, 通过尸体标本和临床验证, 基于该技术制作的导航模板能显著提高寰枢椎螺钉置入的准确性。本研究病例组有2例患者使用了3D打印的导板辅助置钉, 并结合术中CT即刻了解螺钉位置(图4), 证实螺钉位置良好。目前, 3D打印导板技术结合术中CT指导寰枢椎置钉, 尚未见相关报道。
本研究病例数较少, 随访时间尚短, 但研究结果显示术中CT可以满足寰枢椎复位、固定术个性化治疗的手术需要。术中CT引导下穿刺置钉, 可减少术中相关并发症发生, 还可以在术中验证寰枢关节复位情况、局部减压程度和植入螺钉的位置, 一定程度上避免二次手术的风险。3D打印导板结合术中CT指导寰枢椎置钉的结果显示良好。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|