
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT扫描对桡骨远端B3骨折的诊断价值
[李绍良, 王满宜, 鲁谊△  ]
]
]
|
|


目的:评价三维CT扫描是否提高对AO分型B3型桡骨远端骨折的检出率。方法:选择2013年1月至2014年1月,北京积水潭医院创伤骨科急诊收治的30例桡骨远端骨折患者进行回顾性分析,所有患者均接受了切开复位内固定术,采集所有病例的原始X线片和三维CT扫描图像,由2名医师先根据X线片作出骨折的AO分型诊断,再根据三维CT扫描检查结果作出骨折AO分型诊断,将X线与三维CT扫描作出的诊断结果进行比较,评价X线和CT对B3骨折的检出率,并计算Cohen’s Kappa值判断X线片和CT对B3型骨折的诊断是否一致。结果:30例骨折病例经手术确认均为B3型桡骨远端骨折, 10例术中确认为B3.3型骨折。三维CT检查结果的诊断与手术判断一致,而单纯依靠X线片只能诊断24例(24/30,80%)的B3型骨折,发现6例(6/10,60%)B3.3型骨折。CT扫描对B3型骨折的检出率优于X线(100% vs. 80%, P<0.05 ),对B3.3型骨折的检出率也优于X线(100% vs. 60%, P<0.05 )。CT扫描和X线检查对B3和B3.3型骨折诊断的一致性较差(kappa值=0), 最重要的是在此研究过程中发现并描述了两种特殊类型的B3型骨折,即桡侧B3型骨折和尺侧B3型骨折。结论:CT可以显著提高B3和B3.3桡骨远端骨折的诊断率, 并有助于我们发现两种特殊类型的B3型骨折。
Objective:To determine whether 3-dimentional CT scans is able to effectively improve the detection rate of AO B3 distal radius fractures in clinics.Methods:From Jan 2013 to Jan 2014, 30 patients with distal radius fractures were retrospectively enrolled in this study, all the patients directly visited the skeletal trauma emergency department in Beijing Jishuitan Hospital post injury and all of them accepted open reduction and internal fixation of distal radius fractures at last. All the radiographic data including X ray films and 3-dimentional CT scans of these patients were collected. Two independent observers were required to make primary AO classifications for each fracture by X rays at first, then to make final AO classifications by 3-dimentional CT scans. Finally, the detection rates of CT scans and plain films for AO B3 distal radius fractures and B3.3 distal radius fractures were compared, the agreements of the two methods for diagnosing AO B3 and B3.3 fractures were calculated by Cohen’s Kappa calculations.Results:All the 30 fractures were confirmed to be AO B3 distal radius fractures intraoperatively, and 10 of them were B3.3 fractures. The results were completely consistent with the results of 3-dimensional CT scans. However, only 80%(24/30) AO B3 distal radius fractures and 60%(6/10) B3.3 distal radius fractures could be diagnosed only by X rays. The detection rate of CT scans was proved to be significantly higher than X rays for diagnosing B3 distal radius fractures(100% vs. 80%, P<0.05), the detection rate of CT scans was also proved to be significantly higher than that of plain films for detecting B3.3 distal radius fractures(100% vs. 60%, P<0.05). The agreement of 3-dimentional CT scans and X ray was poor for detecting both the AO B3 distal radius fracture and B3.3 distal radius fracture (kappa=0). Most importantly, in the study process, two special kinds of B3 distal radius fracture were initially found and described by us. One was named as radial B3 fracture, and the other was named as ulna B3 fracture.Conclusion:3-dimentional CT scans can effectively improve the detection rate of B3 and B 3.3 distal radius fractures, and also help find two special kinds of B3 fractures.
在桡骨远端骨折中, AO分型的B3型骨折特指桡骨远端掌侧关节面的剪切力骨折, 通常合并腕骨向掌侧脱位或半脱位[1, 2], 是一种特殊的桡骨远端骨折。这种骨折累及到桡腕关节面, 并且不稳定, 治疗上需要手术精确的解剖复位, 坚强内固定, 所以临床上需要高度重视这种骨折的正确诊断, 避免误诊、漏诊而采用错误的治疗方法。
虽然普通X线片是初始的诊断工具, 但对于复杂的骨折, X线片不能够提供足够的影像学信息。近年来文献报道了有关CT在桡骨远端骨折诊疗中的作用, 如应用CT诊断桡骨远端骨折累及下尺桡关节面受损的情况[3], 用CT描述桡骨远端关节内骨折的具体骨折形态[4], CT研究桡骨远端掌侧剪切力骨折累及背侧皮质骨折的问题[5], 而对于关节内骨折, 目前公认CT可以提供更详尽的骨折形态学资料, 并有助于治疗方式的选择[6, 7, 8]。
对于AO分型的B3型骨折, 目前尚未见CT与X线诊断比较的报道, 本研究通过分析30例B3型桡骨远端骨折患者的X线和三维CT扫描资料, 目的在于:(1)总结该特殊类型骨折的CT评估对临床诊疗的影响; (2)比较CT和X线对这种特殊骨折的诊断的检出率是否一致; (3)分析通过 CT图像是否能够发现特殊类型的B3骨折。
选择2013年1月至2014年1月于北京积水潭医院急诊科就诊, 并且通过手术最终诊断为AO分型B3型桡骨远端骨折的患者共30例进行回顾性分析, 平均年龄(41± 13)岁, 其中男性11例(36.7%)、女性19例(63.3%), 左侧19例(63.3%)、右侧11例(36.7%)。本研究开始前已通过北京积水潭医院医学伦理委员会审查批准。
经北京积水潭医院PACS(picture archiving and communication systems)系统收集完整的影像学资料后, 由2名经过AO分型培训合格后的观察者(1名放射科医师, 1名骨科住院医师)先依次阅览患者的X线片, 做出初步诊断和分型, 是否B3型骨折(图1), 并进一步判断是否为B3.3骨折。再依次阅览患者的CT图像, 做出最后诊断和分型。B3.3骨折的定义为桡骨远端掌侧的剪切力骨折块分为舟骨关节面骨块和月骨关节面骨块两块(图2)[9, 10]。
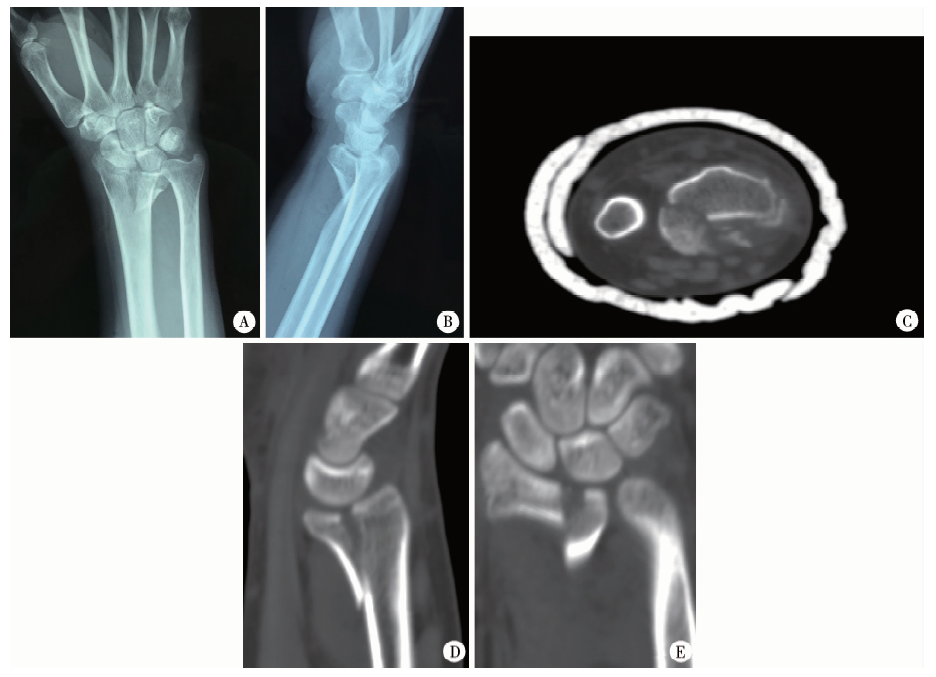
 | 图1 年龄49岁, 女性, AO B3型骨折, X线可见桡骨远端掌侧剪切骨折合并腕骨向掌侧的半脱位(A、B), CT可见向掌侧移位的桡骨远端掌侧骨折块(C), 桡腕关节向掌侧脱位(D)Figure 1 A 49-year old female patient sustained AO B3 distal radius fracture, volar shearing fragment associated with volar subluxation of carpals was found in X ray (A, B), volarly displaced fragment was shown in CT (C), volarly dislocation of radiocarpal joint (D) |
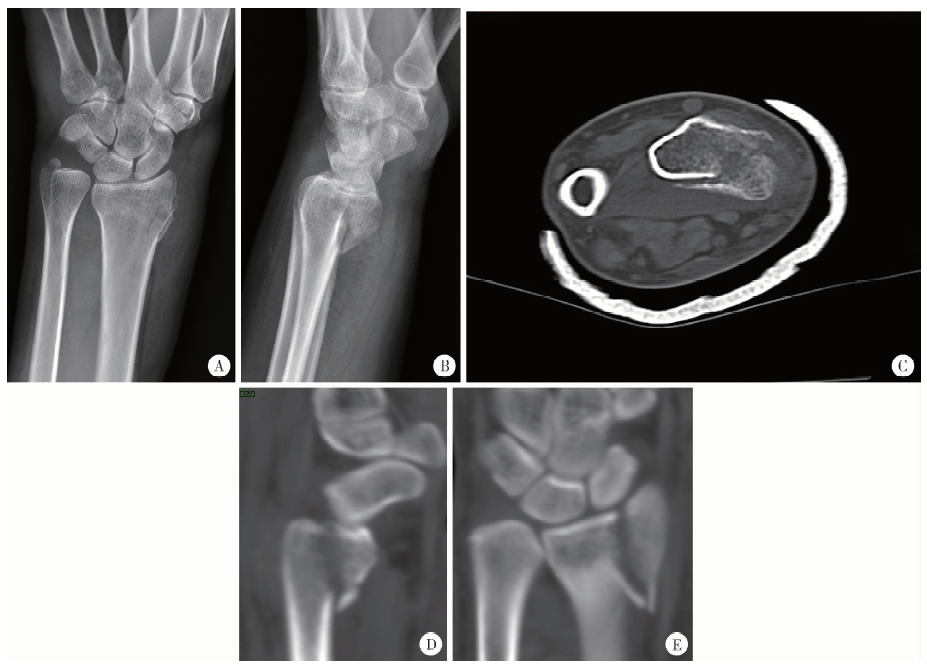
 | 图2 年龄56岁, 女性, B3.3型粉碎骨折, 可见桡骨远端掌侧关节面的剪切力骨折, 掌侧骨折块分为桡侧和尺侧两块Figure 2 A 56-year old female patient sustained a AO B3.3 comminuted fracture, volar shearing fracture of the joint surface was found and the volar fragment was divided into two fragment in radial side and ulna side |
所有诊断结果均由2名观察者协商一致后决定, 最后比较每位患者的X线初步诊断分型与CT最后诊断分型是否一致。所有患者的诊断均以手术中确定的最终诊断分型为准, 手术均采用桡侧腕屈肌入路, 充分显露骨折端, 精确复位后以掌侧钢板固定, 术中辅以C型臂透视。
所有患者急诊就诊后均常规行腕关节的标准正侧位X线检查及三维CT扫描, 对腕关节骨折北京积水潭医院常规采用东芝Aquilion(TSX 101A)16排螺旋CT扫描机, 扫描层厚0.5 mm, 螺距0.5 mm, 重建间隔 2 mm, 电流150 mA, 电压120 kV。
使用SPSS 19.0(SPSS公司, 美国)软件进行数据录入及统计学分析。X线片和CT扫描诊断检出率比较采用卡方检验, 检验水准α 值取双侧0.05。X线和CT扫描的诊断一致性通过计算Cohen’ s Kappa值判断。
根据2名独立观察者阅览影像学资料所做出的诊断, 发现仅靠标准的正侧位X线检查, 初步诊断仅确诊了24例桡骨远端B3型骨折, 确诊了6例B3.3骨折; 但通过三维CT扫描, 所有30例患者的最终诊断分型均为桡骨远端B3型骨折, 10例 B3.3骨折, 包括X线上诊断为B3.3骨折的6例。最后手术中通过观察骨折的实际形态确定CT扫描的结果是准确的。
本组病例中, 单独X线片诊断B3型桡骨远端骨折的检出率只有80%(24/30, 图2), 单独X线片上B3.3型骨折的发现率为60%(6/10)。三维CT扫描对B3型骨折的检出率优于X线(100% vs. 80%, P< 0.05 ), 对B3.3型骨折的检出率也优于普通X线(100% vs. 60%, P< 0.05 )。X线与CT检查的一致性检验kappa值为0, 说明X线和CT检查对同一骨折的诊断一致性较差。
X线检查没有确诊的6例患者中有1例漏诊, 1例误诊为桡骨远端AO分型A2型骨折, 4例误诊为AO分型B1型骨折, 但经CT扫描和手术治疗最终诊断分型均为B3型骨折, 而且通过CT检查发现6例均为特殊的B3型桡骨远端骨折, 即桡舟关节面或桡月关节面的掌侧剪切力骨折, 与骨折关节面相对应的舟骨或月骨向掌侧半脱位。3例为尺侧B3骨折(图3), 即桡骨远端的桡月掌侧关节面剪切力骨折合并桡月关节半脱位, 而桡舟关节对合关系保持正常; 另外3例为桡侧B3骨折(图4), 即桡骨远端的桡舟掌侧关节面剪切力骨折合并桡舟关节半脱位, 而桡月关节面基本完整或轻微骨折, 桡月关节保持正常对合关系。这两种特殊类型的B3型骨折目前尚未见报道。
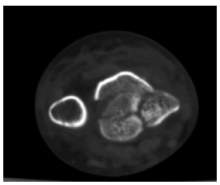
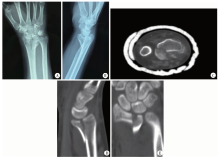
 | 图3 年龄38岁, 男性, 依靠X线最初诊断为桡骨远端骨折AO B1型(A、B), 经CT检查后发现为AO B3型骨折, 且骨折只累及桡月关节面(C), 矢状位扫描可见尺掌侧骨折块及向掌侧脱位的桡月关节(D), 冠状面上显示的尺侧骨块(E)Figure 3 A 38-year old male patient was initially diagnosed AO B1 distal radius fracture on X ray(A, B), later was found to be AO B3 fracture on CT scans, and the fracture only involved the radiolunate joint surface (C), displaced ulna volar fragment and volarly dislocated radiolunate joint in saggital view (D), ulna fragment was shown in coronal view (E) |
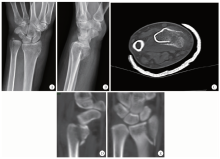
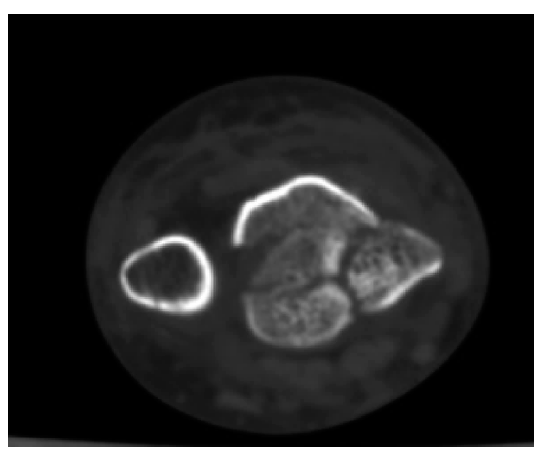
 | 图4 年龄35, 男性, 单纯依赖X线诊断为AO A2型骨折(A、B), 经CT检查后确诊为AO B3型骨折, 且骨折只累及桡舟关节面(C), 矢状位扫描上可见移位的桡掌侧骨折块及桡舟关节向掌侧脱位(D), 冠状位扫描上可见桡侧骨折块(E)Figure 4 A 35-year old male patient was initially diagnosed AO A2 fracture (A, B), later was found to be AO B3 fracture, and the fracture only involved radioscaphoid joint surface (C), displaced radial volar fragment and volarly dislocated radioscaphoid joint in saggital view (D), radial fragment was shown in coronal view (E) |
桡骨远端骨折AO分型B3型骨折典型的侧位X线表现为:桡骨远端背侧皮质基本完整, 掌侧缘皮质连续性中断, 可见冠状面的骨折线, 腕骨跟随掌侧的关节面骨块向掌侧及近端半脱位, 桡腕关节面可见台阶(图1)。AO分型根据X线上骨折块的大小将B3骨折分为B3.1小骨块骨折, B3.2大骨块骨折, B3.3粉碎骨折[9, 10]。
目前关于B3型骨折CT图像表现的研究很少见, Souer等[5]用三维CT测量了25例桡骨远端掌侧剪切力骨折, 发现其中10例为C型骨折, 7例为真正的B型骨折, 剩余8例介于B型和C型之间。刘红光等[11]用CT扫描了22例掌侧Barton骨折即B3型骨折, 认为CT扫描能更清晰地显示Barton骨折及脱位。而本研究通过分析30个病例的CT表现, 发现CT对于桡骨远端剪切力骨折的诊疗有十分重要的意义。
首先, 单纯行X线检查有漏诊和误诊的可能性, 本组病例中单纯依靠X线检查只能正确诊断80%的B3骨折, 而结合三维CT扫描可以将诊断的准确率提高到100%; 其次, CT还有助于准确判断骨折的粉碎程度, 在本组病例中, 单纯依靠X线仅发现60%的B3.3型骨折; 另外, CT还有助于判断剪切力骨块的大小、位置、关节是否脱位等, 更有利于临床医师做出准确的判断, 给患者提供个性化的治疗[12, 13, 14, 15], CT对于关节内的桡骨远端骨折, 较X线可以更精确地评价关节面骨折的分离、塌陷和粉碎情况, 所以CT通过提供详细准确的影像学信息, 直接影响到治疗方式的选择, 可以帮助医生作出手术治疗的决定, 并选择合适的手术入路[16, 17]。
本研究还通过CT发现了少见的特殊骨折类型, 即桡侧或尺侧B3骨折, 从CT上观察, 其骨折线更接近于矢状面, 且只累及桡舟或桡月关节面, 造成部分关节面的分离塌陷, 累及的半侧桡腕关节出现半脱位, 而未累及的另一半桡腕关节, 对线基本维持正常。
AO分型B3.3型桡骨远端骨折近年来受到很多学者的关注, Beck等[9]总结了52例B3型骨折, 结果发现常规应用掌侧钢板固定B3.3型骨折有失败的风险, 因此建议对小的掌侧月骨窝骨块加用克氏针, 微型螺钉、线缆等固定方式以降低手术失败的风险。Tan等[18]报道了两例手术固定失败的B3.3型骨折, 其中1例经过3次手术才治疗成功, 因此建议临床高度重视B3.3骨折, 尤其要注意固定掌尺侧的关节面骨块。本研究中B3.3型骨折占全部B3骨折的33.3%(10/30), 所以临床中切忌忽略或低估B3.3型骨折, 而影像学正确的发现并诊断该特殊类型的骨折是保证治疗成功的第一步, 也是关键的一步。虽然以往常规应用X线作临床诊断, 但本研究说明仅仅依靠X线检查是不够准确、不够严谨的, 而应用三维CT扫描能显著提高诊断的准确率, 也更有利于这种特殊类型骨折的治疗。
本研究尚存在以下不足:(1)回顾性研究难免存在回忆偏倚; (2)由于严格的纳入排除标准, 样本量较小, 代表性不足, 希望将来进行大样本的随机对照的前瞻性研究来进一步证实结论。
综上所述, 对于所有可疑的AO分型B3型骨折, 除了必需的X线检查, 有条件时, 一定要进行三维CT扫描, 这样有助于提高临床医师的诊断水平, 更深入地认识这种特殊类型的骨折, 并根据骨折的形态提供个性化的治疗。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|