





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
不同下颌前伸度口腔矫治器治疗阻塞性睡眠呼吸暂停低通气综合征的系统评价
[马燕燕, 章晶晶, 高雪梅△  ]
]
]
|
|


目的:评价不同下颌前伸度的口腔矫治器治疗阻塞性睡眠呼吸暂停低通气综合征(obstructive sleep apnea and hyponea syndrome,OSAHS)的临床疗效。方法:计算机检索PubMed、Embase、Cochrane图书馆、CNKI、维普和万方等数据库,纳入不同下颌前伸度的口腔矫治器治疗OSAHS的随机对照试验(randomized clinical trials,RCT)和前后对照试验(before-after trials,BAT),对其进行质量评价并提取资料,用RevMan 5.3软件进行meta分析。结果:纳入2个RCT、2个采用了随机方法的BAT和3个非随机BAT,共244例患者。根据方法学质量评价及各试验设计情况,对其中4篇高质量研究进行meta分析,结果显示,下颌前伸量达到下颌最大前伸度(maximal mandibular advancement,MMA)50%与75%两组的治疗有效率[呼吸暂停低通气指数(apnea hypopnea index,AHI)或氧减指数(oxygen desaturation index,ODI)降低>50%]比较, I2=0%,合并效应量 RR值为0.93, 95% CI为0.80~1.09;两组的治愈率(AHI或ODI<10次/h)比较, I2=45%,合并效应量 RR值为0.85, 95% CI为0.68~1.06,证据尚不足以证明两组的治疗有效率和治愈率有差异。亚组分析提示病情严重程度可能是影响治愈率的重要因素。结论:对于OSAHS患者,在一定范围内下颌前伸度增加有利于提高治疗有效率和治愈率,但尚缺乏足够证据证明75%MMA优于50%MMA;轻症患者治愈率高于重症。
Objective:To evaluate the polysomnology results along with mandibular titrated advancement using oral appliance to treat obstructive sleep apnea and hyponea syndrome(OSAHS).Methods:Several electronic databases (PubMed, Embase, Cochrane Library, CNKI, VIP, and Wanfang) were systematically searched up to September 2015.There was no restriction of language or source of information. All randomized clinical trials (RCT) and before-after trials (BAT) comparing at least two different mandibular advancements were included. Two independent reviewers selected the studies, extracted data and evaluated risk of bias by quality assessment. Data were pooled using a fixed-effects model, and the summary effect measure was calculated by risk ratio ( RR) and 95% CI. Meta-analysis was performed using RevMan 5.3 software.Results:Two RCTs and five BATs were included in the review. Among the five BATs, two of them were randomized, while the other three were not. Outcomes including apnea hypopnea index (AHI), oxygen desaturation index (ODI), success rate (reduction of AHI or ODI >50%), normalization rate (AHI or ODI<10/h) were assessed in this review. Based on the trial design and quality assessment, four studies were included for meta-analysis. No significant difference in the success rate was found between the group with 50% of the maximal mandibular advancement (MMA) and the group with 75% of MMA [ I2=0%, RR=0.93, with 95% CI (0.80, 1.09)]. No significant dif-ference in the normalization rate was found between the 50% of MMA and 75% of MMA groups [ I2=45%, RR=0.85, with 95% CI (0.68, 1.06)]. Subgroup analysis displayed that the severity of OSAHS before treatment was a potential factor affecting the normalization rate.Conclusion:Based on current available evidence, the success rate and normalization rate for treating OSAHS in the patients with 75% MMA were not found to be significantly higher than those with 50% MMA. Due to small simple size in this meta-analysis, the results of the present study should be interpreted with caution. Further prospective studies are needed to strengthen the evidence.
阻塞性睡眠呼吸暂停低通气综合征(obstructive sleep apnea and hyponea syndrome, OSAHS)是一种常见的睡眠呼吸障碍, 以睡眠时反复发生上气道部分或完全阻塞为特征, 常伴随着微觉醒。OSAHS的治疗方法包括行为治疗(控制体重、戒酒、睡眠姿势调整)、持续正压通气(continuous positive airway pressure, CPAP)、口腔矫治器、各种上气道软(硬)组织手术、药物治疗等。CPAP是治疗OSAHS的首选方法, 但很多患者不能或不愿使用呼吸机。美国睡眠医学研究会(American Academy of Sleep Medicine, AASM)推荐口腔矫治器用于治疗轻中度的OSAHS和不能耐受CPAP的重度OSAHS患者[1]。
治疗OSAHS的口腔矫治器中, 下颌前移类矫治器使用范围最广, 近来很多随机对照试验(rando-mized clinical trials, RCT)证明下颌前移类矫治器能有效减轻睡眠呼吸暂停、改善日间嗜睡、提高生活质量[2, 3, 4]。下颌前移矫治器通过改变下颌位置, 直接或间接改变上气道周围解剖结构关系, 减轻或消除上气道的阻塞, 同时降低了上气道塌陷性[5]。
但影响下颌前移矫治器疗效的因素有很多[6, 7], 不同研究得到的治疗有效率差别较大[8, 9, 10, 11], 其中一个重要原因是不同研究中矫治器的下颌定位不同。目前临床医生进行下颌定位主要凭经验和习惯, 缺乏精确的标准定位, O’ Sullivan等[12]将下颌定位在患者下颌最大前伸度(maximal mandibular advancement, MMA)70%附近的位置, Ferguson等[13]将下颌定位在MMA减去3 mm的位置。近年还出现了使用远程控制下颌前伸度的滴定式研究来预测疗效和确定最适前伸位置[14], 但此方法尚未大范围推广使用。Ferguson等[15]提出下颌前伸度越大, OSAHS症状减轻越明显, 但是此论断也尚未被证实。本系统评价的目的在于比较下颌不同前伸度对OSAHS治疗效果的影响。
纳入研究的选择标准如下:(1)研究类型:RCT(无论是否采用盲法及隐蔽分组)或前后对照试验(before-after trials, BAT); (2)研究对象:经多导睡眠监测诊断为OSAHS的成人患者, 排除中枢性或混合性睡眠呼吸暂停低通气者; (3)干预措施:研究设计口腔矫治器至少包括两种不同的下颌前伸度; (4)观察指标:睡眠监测指标, 如呼吸暂停低通气指数(apnea-hyponea index, AHI)、呼吸紊乱指数(respiratory disturbance index, RDI)、最低血氧饱和度(minimum oxygen saturation, MinSaO2)、氧减指数(oxygen desaturation index, ODI), 计算治疗有效率(success rate, AHI或ODI降低> 50%)、治愈率(normalization rate, AHI或ODI< 10次/h)。
文献检索分为电子数据库检索和参考文献检索。电子数据库检索策略采用主题词和自由词相结合的原则, 以sleep apnea、sleep apnea syndrome、OSA、OSAS、OSAHS、snore、upper airway resistance syndrome、sleep-disordered breathing、mandibular advancement、mandibular protrusion、mandibular repositioning、睡眠呼吸暂停、鼾症、下颌前伸、口腔矫治器等为检索词, 数据库包括PubMed、Embase、Cochrane图书馆、CNKI、维普、万方, 检索年限为各数据库建库至2015年9月9日, 无语言限制。表1为PubMed检索策略。经电子数据库检索纳入的文献, 对其进行参考文献检索, 筛选出符合标准的文献。
| 表1 PubMed 检索策略 Table 1 Search strategy for PubMed |
两名评价员分别按照检索策略和选择标准对文献进行检索和筛选。通过NoteExpress对文献进行去重, 然后阅读所有文献的题目和摘要, 排除明显不符合选择标准的文献(如动物实验、非口腔矫治器、正常人群研究、回顾性研究、综述等); 获取并阅读所有潜在相关文献的全文, 筛选出符合纳入标准的文献, 如遇分歧通过讨论或者第三方协商解决。
两名评价员分别独立对最终纳入的文献按照事先制定的数据提取表进行数据提取, 包括作者、年代、研究设计、样本量、年龄、体重指数(body mass index, BMI)、下颌前伸度、治疗效果(睡眠监测指标的变化)、治疗有效率和治愈率, 数据缺失时尽量联系文章原作者。纳入的研究按照Cochrane系统评价手册5.1.0的RCT质量评价标准[16], 对其随机方法、隐蔽分组、盲法、结果数据的完整性、选择性报告研究结果、其他偏倚来源等方面进行质量评价, 如意见不同则通过讨论或与第三方协商解决。
若纳入的文献数量足够且质量较高, 则考虑进行meta分析。采用Cochrane协作网提供的RevMan 5.3软件进行统计分析, 计数资料采用相对危险度(risk ratio, RR)及其95%可信区间(confidence interval, CI)为疗效分析统计量, 计量资料采用加权均数差(weighted mean difference, WMD)及其95%CI为疗效统计量。各纳入研究间的异质性采用χ 2检验, 若P> 0.1且I2< 50%则采用固定效应模型; 若P< 0.1且I2> 50%则尽可能寻找统计学异质性产生的原因, 根据临床和方法学异质性因素进行亚组分析或敏感性分析; 若研究间无临床和方法学异质性, 则采用随机效应模型。
初检文献共1 864 篇, 其中PubMed 301篇、Embase 601篇、Cochrane 218篇、CNKI 165篇、维普220篇、万方359篇, 排除重复文献后剩余1 380篇。阅读文献题目和摘要后排除明显不符合纳入标准的文献1 349篇, 对可能符合纳入标准的31篇文献阅读全文后, 排除24篇(排除理由:无法获取睡眠监测指标、只研究一种下颌前伸度等), 最终纳入7篇文献[17, 18, 19, 20, 21, 22, 23](图1)。
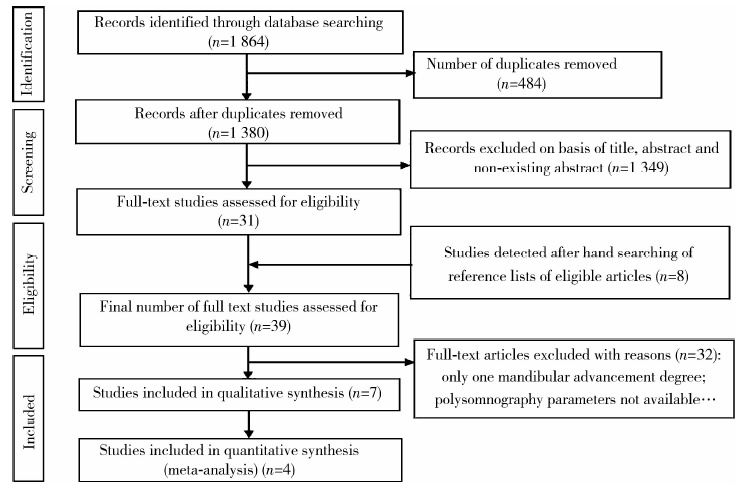 | 图1 文献筛选流程图Figure 1 Flow chart of selection process |
本研究纳入的7篇文献的研究基本特征见表2, 其不同下颌前伸度的有效率及治愈率见表3。
| 表2 系统评价下颌定位疗效的纳入研究基本特征 Table 2 Characteristics of the included studies for systematic review of mandibular re-positioning |
| 表3 不同下颌前伸度的患者治疗前后AHI或ODI及治疗有效率和治愈率 Table 3 AHI or ODI before and after treatment, success and normalization rate for different mandibular advancement degrees |
纳入的7篇研究中有2篇RCT[22, 23], 2篇为随机BAT[20, 21], 3篇为非随机BAT[17, 18, 19]。对其随机方法、隐蔽分组、盲法、结果数据的完整性、选择性报告研究结果、其他偏倚来源等7项条目, 按照Cochrane系统评价手册5.1.0偏倚风险评价标准判断为偏倚风险低、偏倚风险高及风险不清楚, 结果见图2和图3。
 | 图2 偏倚风险图:每个条目每种判断(低风险、高风险、风险不确定)的比例Figure 2 Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies |
 | 图3 偏倚风险总结图:各个研究的每个条目的判断结果交叉表Figure 3 Risk of bias summary: review authors’ judgments about each risk of bias item for each included study |
4项研究按照MMA百分比(25%、50%、75%)分组, 2项研究按毫米数分组, 1项研究按照60%MMA+毫米数分组, 表4为MMA百分比与毫米数对应关系。由表4可估算出平均MMA约9.5 mm, 25%MMA约2.4 mm, 50%MMA约4.8 mm, 75%MMA约7.0 mm。按毫米数分组的研究只有2篇(分别为2、4、6 mm和2、4、6、8 mm), 其前伸度与50%MMA(约4.8 mm)、75%MMA(约7.0 mm)相差较大, 不宜合并分析, 并且这两项研究质量不高, 故仅作描述性评价, 不进行汇总分析。按照MMA百分比分组的4项研究质量较高, 其中Tegelberg等[23]的RCT研究6个月失访率小(< 20%), 1年失访率高(> 20%), 鉴于其他研究随访期限约6个月, 所以提取随访6个月的数据进行meta分析。此4项研究的下颌前伸度分组不完全相同, 均有50%MMA与75%MMA分组, 而25%MMA组仅有1篇文献进行了研究, 因此25%MMA组无法进行汇总分析。对4项研究[20, 21, 22, 23]的50%MMA与75%MMA组提取数据, 以治疗有效率、治愈率分别作为观察指标进行meta分析。
| 表4 MMA百分比与对应毫米数 Table 4 The percentage of maximal mandibular advancement and corresponding millimeters |
2.4.1 50%MMA与75%MMA治疗有效率的比较 对这4项研究进行异质性检验, 计算统计量(P=0.70, I2=0%), 因异质性小, 故采用固定效应模型对数据进行合并。合并效应量RR值 0.93, 95%CI为0.80~1.09, 落在森林图无效竖线上, 证据尚不足以证明两组治疗有效率有差异(图4)。
 | 图4 50%MMA与75%MMA有效率比较Figure 4 Comparison of the success rate between group 50%MMA and group 75%MMA |
2.4.2 50%MMA与75%MMA治愈率的比较 对这4项研究进行异质性检验, 计算统计量(P=0.14, I2=45%), 因可能存在中度异质性, 故采用固定效应模型对数据进行合并。合并效应量RR值0.85, 95%CI为0.68~1.06, 落在森林图无效竖线上, 证据尚不足以证明两组治愈率有差异(图5)。
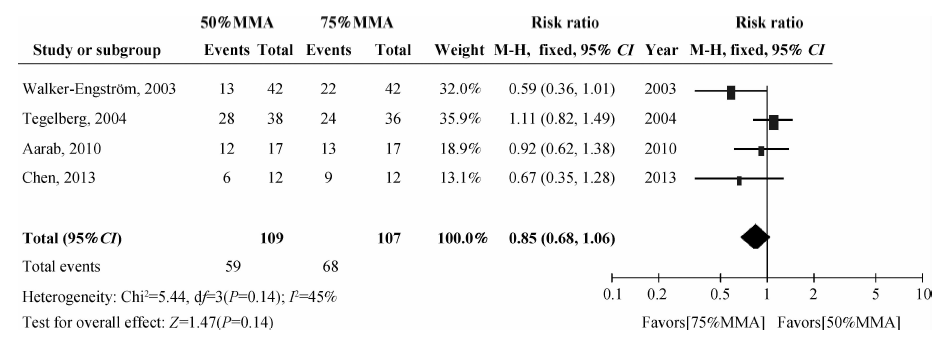 | 图5 50%MMA与75%MMA治愈率比较Figure 5 Comparison of the normalization rate between group 50%MMA and group 75%MMA |
临床上认为口腔矫治器对于轻中、重度OSAHS的疗效有差别, 纳入meta分析的4个研究中, Walker-Engströ m等[22]的研究对象是重度OSAHS(AHI> 30次/h)患者, 而Aarab等[20]、陈荟[21]、Tegelberg等[23]的研究对象是轻中度OSAHS(5次/h< AHI< 30次/h)患者。治疗有效率的meta分析异质性小(I2=0%), 治愈率的meta分析异质性中等(I2=45%), 按照病情轻重进行亚组分析, 组间异质性I2=64.1%, 两亚组的效应量差异较大(图6), 提示病情严重程度不同, 治愈率有差异。由于纳入文献数量及样本量少, 证据尚不足以证明下颌前伸达到75%MMA时治愈率高于50%MMA。
 | 图6 50% MMA与75% MMA治愈率亚组分析Figure 6 Subgroup analysis of the normalization rate between group 50% MMA and group 75% MMA |
本系统评价共纳入7篇研究, 其中2篇RCT分别研究了轻中、重度OSAHS患者两种不同下颌前伸度(50%和75%MMA)的疗效[22, 23], 其余5篇BAT进行了下颌前伸的滴定式研究, BAT的优点是消除了个体差异的影响, 可靠性高。研究均发现下颌前伸度是影响AHI降低率的重要因素, 下颌前伸过小(如25%MMA或者2 mm), 有效率低(约20%), 随着前伸增大, 在一定范围内, 有效率和治愈率均有所增加(50%MMA有效率约73%, 75%MMA有效率约81%), 这与临床观察是一致的, Walker-Engströ m等[22]将50%MMA组部分疗效不佳者前伸度提高至75%MMA, 有效率和治愈率明显增加。
有意思的是, meta分析显示, 50%MMA与75%MMA位点的有效率和治愈率均无统计学差异, 但有效率的异质性小, 治愈率的异质性变大, 提示随着下颌前伸, 疗效并不随之呈线性关系改变, 较小的下颌前伸(50%MMA)即可带来一定疗效。随着下颌前伸度增大, 颞下颌关节及口周肌肉负担增加, 副反应增多, 所以建议临床实践以50%MMA作为初始的下颌前伸度, 特别是对轻中度OSAHS患者。但治愈率的研究异质性大, 提示可能在增加样本数量后出现新的结论。
本研究亚组分析显示, 初始病情严重程度不同者治愈率有差异, 但还缺乏足够的证据证明75%MMA优于50%MMA, Liu等[19]发现治疗有效患者的最适前伸度随患者原始AHI值的增加而增大, 临床上一般主张治疗重度OSAHS患者可适当增大下颌前伸度。
下颌前移矫治器的疗效不仅与矢状向下颌前伸度有关, 还受垂直方向的咬合打开距离的影响。下颌张开的程度应因人而异, 需参考有关颅颌面形态、上气道狭窄部位等检查结果[24]。我们纳入的7项研究中, 不同研究间垂直打开距离差别较大(2 mm、6 mm或5~8 mm), meta分析纳入的4项研究保证了各研究内组间垂直打开距离一致。若不控制垂直距离一致, 则下颌前伸越多越容易发生后旋, 会影响矫治器的疗效评价。
文献分析发现, 虽然有大量的口腔矫治器研究, 但对于下颌定位这一临床核心问题缺乏系统的研究, 基本上是各位临床医生采用自己习惯的操作方法、标准和评价指标来处理临床病例, 导致各研究之间分组情况不尽相同, 因此能够合并分析的研究不多。口腔矫治OSAHS疗效显著, 可能是该方面的临床研究有些忽视随机和对照的原因。本系统评价纳入的RCT研究较少, 几项BAT研究质量也不高, 因此, 研究结论还需要未来更多设计和实施严格的试验加以确证。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|