

{kind=link}
{kind=link}
{kind=link}
{kind=link}
锥形束CT分析下颌无牙颌患者前部颌弓形态对“All-on-4”种植设计的影响
[李世赢1 , 李刚2 , 冯海兰1 , 潘韶霞1, △  ]
]
]
|
|


目的:通过测量分析下颌无牙颌患者的锥形束CT(conebeam computed tomography, CBCT)图像,测量可能植入种植体的A-P距离(anterior-posterior distance),分类前部颌弓形态,探究颌弓形态对“All-on-4”远中倾斜种植体临床设计的影响。方法:收集下颌无牙颌患者的CBCT图像共74例,其中男性35例,女性39例,拟行“All-on-4”种植固定义齿修复。在经颏孔并平行于牙合平面的平面上测量可能植入种植体的A-P距离,分类前部颌弓形态,测量由颏孔往近中方向7.5 mm的颌骨段所跨过的颌弓弧度,探究A-P距离与该弧度的相关性。结果:74例患者测得可植入的颏孔间区种植体的A-P距离为(8.5±1.5) mm(最小为4.5 mm,最大为11.8 mm),其中≤7 mm者占12.2%(男性3例,女性6例),颌弓为方圆形;>7 mm、≤9 mm者占54.0%(男性20例,女性20例), 颌弓为卵圆形;>9 mm者占33.8%(男性12例,女性13例),颌弓为尖圆形。测量患者颏孔前方7.5 mm颌弓段转角弧度,左、右两侧共测得148个数据,平均为15.9°±5.5°(最小为5.6°,最大为35.2°)。统计分析发现,A-P距离与转角弧度呈显著负相关。结论:本研究中下颌无牙颌患者的前部颌弓形态中,卵圆形所占百分比最多,尖圆形次之,方圆形最少。女性方圆形颌弓者多于男性,卵圆形和尖圆形颌弓与性别无明显相关。颌弓越方,A-P距离越小,颏孔前区颌弓弧度就越大,远中斜行种植体所需要的骨宽度就越大。下颌无牙颌患者的“All-on-4”种植固定修复采用远中斜行种植体,术前应评估颌弓形态,设计远中种植体的合理倾角,远中种植位点的骨宽度应在常规要求外留有余量。方圆形颌弓是“All-on-4”种植固定修复的不利因素。
Objective:To classify the interforaminal arch form of edentulous mandibles by measuring the anterior-posterior distance (A-P distance) of implants planned to be inserted in “All-on-4” protocol using conebeam computed tomography (CBCT) data, and to investigate the influence of the arch form on the “All-on-4” distally tilted implants.Methods:Seventy-four CBCT images of edentulous mandibles were collected, including 35 males and 39 females respectively. “All-on-4”implant supported fixed prostheses were designed for these patients based on the CBCT data. The A-P distance was measured in the plane which crossed bilateral mental foramens and was parallel to the occlusal plane. The interforaminal arch form of edentulous mandibles were classified according to the A-P distance. The radian of the jaw arch 7.5 mm mesially to the mental foramen was measured bilaterally, and its correlation with the A-P distance was studied.Results:The average A-P distance of implant supported fixed prostheses planned in the interforaminal region was (8.5±1.5) mm (minimum 4.5 mm, maximum 11.8 mm). In the study, 12.2% of the subjects’ mandibles were classified as square arch form with A-P distances ≤7 mm, 54.0% were classified as ovoid with A-P distances >7 mm and ≤9 mm, 33.8% were classified as tapered with A-P distances >9 mm. Bilaterally, 148 results of the radian of the jaw arch 7.5 mm mesially to the mental foramen were obtained, and the average radian was 15.9°±5.5° (minimum 5.6°, maximum 35.2°). The radian and the A-P distance showed a negative correlation with statistical significance.Conclusion:In this research, the ovoid arch form was the most common type in edentulous mandibles, followed by tapered arch form. The square arch form showed the lowest percentage. As the arch form went squarer, the A-P distance became shorter, the radian of the jaw arch mesially to the mental foramen went greater, and the bone width that distally tilted implants need became bigger. The interforaminal arch form of the edentulous mandible should be analyzed before an implant supported fixed restoration is designed in the interforaminal region. The angle of inclination of distal implants should be reasonable. The bone width of the distal implant site must be adequate. The square arch form contributes negatively to the structure of implant supported fixed prostheses with distal cantilever design.
下颌牙列缺失的种植固定义齿修复能显著提高患者满意度, 增进咀嚼功能, 但由于拔牙后磨牙区的牙槽嵴不断吸收, 该区域的骨量不足常常限制了种植体植入。对此, 学者们提出了各种解决方法, 如短种植体的应用、上置法块状骨移植、下牙槽神经移位术等[1, 2, 3, 4, 5], 但较大的手术创伤、较高的技术难度以及可能的神经损伤等因素[6]使得许多学者转而寻找其他的解决方案。
颏孔间区骨质较密, 骨量相对充足, 重要解剖结构少, 因而成为种植体植入的合适区域[7]。在很多情况下可在颏孔间区植入种植体, 种植体上部连接带有远中悬臂梁的固定修复体。Maló 等[8, 9, 10]提出了下颌牙列缺失的“ All-on-4” 种植技术, 于下颌无牙颌患者的颏孔间区植入4颗种植体, 颌骨前部中线两侧植入两颗种植体, 两侧远中紧邻颏孔前各植入一颗向远中倾斜的种植体, 利用4颗种植体实现对上部固定修复体的支持。
远中倾斜的种植体可以避开颏神经环, 并通过倾斜植入来增加种植体长度, 减少远中悬臂梁长度, 最重要的是其可增大前、后种植体间距离。Bevilacqua等[11]发现上颌远中种植体倾斜度越大(0° ~45° ), 悬臂梁长度越短, 越可以保护义齿结构免受损伤, 同时也有研究表明, 种植体垂直或倾斜植入在减轻种植体周围骨内压力和支持义齿方面并没有显著差异[12]。Takahashi等[13]则发现虽然单个种植体倾斜角度的增加会增加周围骨内应力, 但是如果4个种植体相连, 由于倾斜角度的增加可以减少悬臂梁的长度, 反而可以使周围骨内应力下降。Francetti等[14]的临床研究也表明, 采用种植体垂直植入与倾斜植入, 其边缘骨吸收无显著差异。
虽然无牙颌种植固定修复中, 种植体倾斜植入会使外科手术的复杂程度增加, 但是仍然不失为减少悬臂梁长度、为种植固定义齿提供稳定支持的有效办法, 然而, 这种远中倾斜种植体的植入需要在前、后向跨越一段颌骨长度, 下颌颏孔间区的弓形结构是否会对种植体的植入有一定影响, 目前尚未见研究对此加以分析论证。此外, 无牙颌种植固定修复如采用远中悬臂梁设计, 悬臂梁的长度也与患者颌骨颌弓形态有关。因此, 本研究拟通过对无牙颌患者锥形束CT(conebeam computed tomography, CBCT)的测量分析, 探讨下颌无牙颌患者的“ All-on-4” 种植修复中, 下颌前部颌弓形态对颏孔前方倾斜种植体植入的影响, 以及其对颏孔间区植入种植体的A-P距离(anterior-posterior distance)和修复体远中悬臂梁长度的影响。
本研究收集就诊于北京大学口腔医院修复科的下颌无牙颌患者的CBCT图像。CBCT图像均使用Vatech DCT PRO(韩国)拍摄, 工作电压为90.0 kV, 电流为7.0 mA, 拍摄于北京大学口腔医院放射科。患者拍摄时面部中线与地面垂直, 端坐放松, 眶耳平面与地面平行, 并保持下颌姿势位, 固定头位。使用Ez3D2009软件(怡友公司, 韩国)进行图像测量。
本研究纳入的CBCT图像均包含完整、清晰的下颌无牙颌以及上颌牙列或牙槽嵴图像, 对于视野不够而未能显示全部颏孔前区的CBCT予以排除, 图像模糊者予以排除。
由于牙列缺失, 失去了牙合平面的参考, 本研究采用下列方法确定牙合平面:(1)对于上颌有牙列的患者, 综合参考上颌牙合平面、下颌牙槽嵴顶平面等因素, 确定下颌无牙颌牙合平面; (2)对于全口无牙颌患者, 综合参考上、下颌牙槽嵴顶平面, 梨状孔下缘与髁状突或外耳道的连线(鼻翼耳屏线)确定下颌无牙颌的牙合平面。所有图像都由同一观测者采取统一标准调整至牙合平面观察测量。
截取经双侧颏孔并平行于牙合平面的水平横断面, 在此平面观察颌弓形态。以颏孔前沿对应的下颌骨颊舌向中点作为远中种植体的远中边缘所在点, 左、右各一, 相连成一条直线, 再经下颌前部中线处唇舌向中点作一条直线与之平行, 测量两线之间的距离即为A-P距离(图1)。下颌前部牙弓形态按方圆型、卵圆形、尖圆形进行分类。方圆型牙弓指下颌前部颏孔间区牙槽嵴形态呈方圆型, 前部相应于中切牙及侧切牙部位的牙槽嵴呈一条直线型, 从尖牙区开始向远中旋转, 与前磨牙区牙槽嵴相连续成一方圆形弧形。卵圆形牙弓则为双侧相应于中切牙区的牙槽嵴呈一直线, 从侧切牙区开始轻度向远中旋转, 与前磨牙区连续成为卵圆形弧形。尖圆型牙弓则从中切牙区或侧切牙区开始即依次向远中旋转, 在中线部位形成前突的亭台, 呈尖圆形弧形与前磨牙连续。以方圆形颌弓A-P距离≤ 7 mm, 卵圆形颌弓> 7 mm、≤ 9 mm, 尖圆形颌弓> 9 mm为标准, 对颌弓形态进行分类[15]。
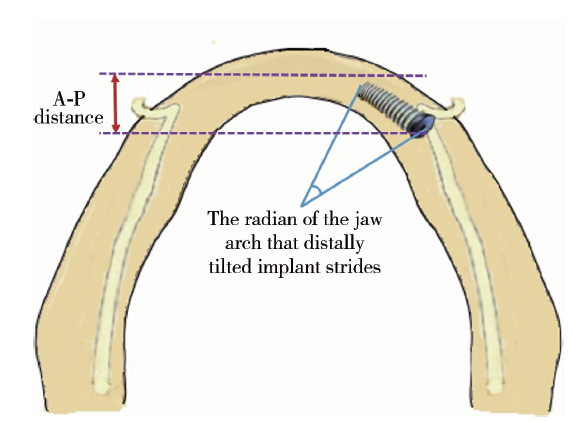 | 图1 A-P距离及远中倾斜种植体在颏孔前跨过的颌弓弧度示意图 A-P distance, anterior-posterior distance.Figure 1 A-P distance and the radian of the jaw arch that distally tilted implant strides |
为了测量远中种植体在近、远中方向上跨过的颌弓弧度, 本研究以该处30° 角倾斜植入长15 mm的种植体为例进行测量, 种植体向前所跨过的弧度也就是从颏孔往近中方向7.5 mm(15 mm× sin 30° )所跨过的颌弓弧度(图1), 每位患者可测得左、右各一个颌弓弧度。使用Ez3D 2009软件的Panoramic Curve+Angle工具进行测量。
所有数据使用SPSS 20.0软件进行统计分析, 使用均数± 标准差对A-P距离及测得的颌弓弧度进行描述, 应用单因素方差分析比较不同牙弓形态所测颌弓弧度的差异, P< 0.05为差异有统计学意义。
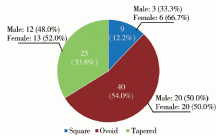
本研究共收集无牙颌患者全口CBCT图像74例, 其中男性35例, 女性39例。74例患者测得A-P距离平均为(8.5± 1.5) mm(最小为4.5 mm, 最大为11.8 mm), 其中≤ 7 mm有9例(男性3例, 女性6例), 占12.2%, 颌弓为方圆形; > 7 mm、≤ 9 mm有40例(男性20例, 女性20例), 占54.0%, 颌弓为卵圆形; > 9 mm有25例(男性12例, 女性13例), 占33.8%, 颌弓为尖圆形(图2)。
 | 图2 下颌无牙颌患者颌弓形态分类Figure 2 Percentage of three arch forms of edentulous mandibles in 74 subjects |
74例患者左、右两侧共测得颏孔前方颌弓转角弧度共计148个, 平均值为15.9° ± 5.5° (最小为5.6° , 最大为35.2° )。使用Pearson相关性分析发现, A-P距离与转角弧度呈显著负相关(r=-0.541, P< 0.05)。
绘制A-P距离与转角弧度的散点图可以发现, A-P距离越大, 即颌弓越呈尖圆形, 远中倾斜种植体所跨过的颌骨段转角弧度越小; A-P距离越小, 即颌弓越呈方圆形, 远中倾斜种植体所跨过的颌骨段转角弧度越大(图3)。
 | 图3 远中倾斜种植体跨过的颌弓弧度(角度)随A-P距离的变化 A-P distance, anterior-posterior distance.Figure 3 The scatter diagram of the radian and the A-P distance |
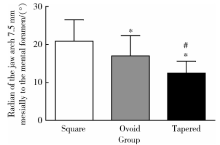
使用单因素方差分析统计3种颌弓形态的下颌无牙颌患者颏孔前7.5 mm颌弓转角弧度, 各组方差不齐, 故使用未假定方差齐性的Tamhane’ s T2 (M)两两比较方法, 结果见表1和图4。
| 表1 3种颌弓形态的下颌无牙颌患者颏孔前7.5 mm颌弓弧度统计描述及比较 Table 1 Statistical description and comparison of radian of the jaw arch 7.5 mm mesially to the mental foramen of three different arch forms |
 | 图4 3种颌弓形态的下颌无牙颌患者颏孔前7.5 mm颌弓弧度 * P< 0.05, compared with square form; # P< 0.05, compared with ovoid form.Figure 4 Radian of the jaw arch 7.5 mm mesially to the mental foramen of three different arch forms |
有研究表明, 单个种植体对于牙槽骨应力随着倾斜角度的增大而增大, 而对于“ All-on-4” 来说, 如果4个种植体相连, 由于倾斜角度的增加可以减少悬臂梁的长度, 远中游离端悬臂梁的长度越小, 对于种植体周围牙槽骨的应力越小, 反而可以使周围骨内应力下降[13], 因此, 牙槽骨内应力的改变是由上述两种作用交互影响的结果。根据研究发现, 在30° 时, 这两种影响可以将牙槽骨内应力降到很低[16], 是临床上常用的选择。因此, 本研究选择30° 的倾斜角度作为假想的远中种植体的标准倾斜角度, 并设定15 mm的长度对该种植体在前、后向所经过的颌弓段形态进行测量分析。实际临床操作中, 远中种植体的倾斜角度可以达到45° , 在0° ~45° 范围内, 可通过种植体配套的多牙基台对角度进行纠正, 使其达到能进行整体支架式固定义齿修复的目的。通过计算可知, 如果种植体植入的倾斜角度为45° , 则15 mm的种植体将在前、后向跨越10.6 mm的距离, 则下颌颌弓形态对种植体植入的影响将更为显著。
本研究根据A-P距离所分类的下颌无牙颌患者前部颌弓形态中, 卵圆形多于尖圆形, 尖圆形多于方圆形, 与有些文献报道(卵圆形> 方圆形> 尖圆形)不同[17], 推测可能与人种有关。
方圆形颌弓中女性多于男性, 卵圆形和尖圆形与性别无明显相关。
在无牙颌整体支架式种植固定修复中, 将两侧远中种植体后缘连线, 通过前部种植体的中心作一条平行于该连线的直线, 那么两线之间的距离称为A-P距离[18]。修复过程中, A-P距离在很大程度上可以决定远中悬臂梁的合理长度。在其他的影响因素(如牙合力大小、对颌牙列情况、口腔副功能、颌骨密度、种植体直径、种植体数量、牙冠高度等)不变的情况下, A-P距离越大, 理论上远中悬臂梁就可以设计得越长。Misch[15]认为, 在咬合力较小的情况下, 远中悬臂梁的长度可以达到A-P距离的1~2倍, 对于咬合力大的患者, 远中悬臂梁的长度则应尽可能减小。
A-P距离主要受颌弓形态的影响, 方圆形颌弓的A-P距离一般较小, 尖圆形颌弓的A-P距离一般较大, 卵圆形颌弓的A-P距离则介于两者之间。本研究正是利用颌弓形态与A-P距离的这种关系, 通过测量A-P距离来对颌弓形态进行分类的。
临床实践中, 设计无牙颌整体支架式固定桥时, A-P距离越小, 出于防止机械并发症及保证种植体安全受力范围的考虑, 其后部所能设计的悬臂梁长度就越短, 因此, A-P距离越小, 所能形成的总体颌弓长度也越短。本研究经测量可知, 仅约1/3的无牙颌患者为尖圆形颌弓, 而约1/8的无牙颌患者为方圆形颌弓, 因此, 在与患者讨论治疗设计时, 如果选择类似“ All-on-4” 的治疗设计, 需要参考患者下颌颌弓形态进行修复体设计, 所能获得的修复体长度与颌弓形态密切相关, 与患者在这一点上的沟通也尤为重要, 事先向患者说明由于解剖条件的限制, 后牙区所能达到的悬臂梁长度的范围, 可以帮助患者理解修复后后牙区咀嚼功能恢复的状况限制、可能的机械力学风险以及美学上可能需要的妥协设计, 如由于形成的牙弓长度过短而有可能在口角处看见牙弓的末端等。
当下颌无牙颌磨牙区的牙槽骨高度不足时, 在颏孔间区植入种植体进行种植固定修复是常用的方法。在类似“ All-on-4” 的设计中, 远中倾斜种植体的位置一般在颏孔前, 由于下颌骨的弓形结构, 往往在此部位会形成一定弧度。如果种植体向远中倾斜, 则其骨内段会跨越一段有弧度的颌骨区域, 从数学上来讲, 种植体的倾斜对种植区域骨量宽度的要求更大。
本研究结果提示, A-P距离与颏孔前方一定距离内颌弓转角弧度呈反比关系, 可以推知, 方圆形颌弓, 颏孔前方的斜行种植体需要跨越较大的颌弓弧度, 这时所需的颊舌侧骨量大于跨越颌弓弧度较小的颌骨量, 尤其在前磨牙区舌侧倒凹较大的情况时需要特别注意, 以免种植体在倾斜植入时引起唇侧或舌侧骨壁的穿通, 损伤软组织[19]。
总结上述无牙颌颌弓所能允许植入的种植体, 颌弓越呈方圆形, 则A-P距离越小, 颏孔前方颌弓拐角弧度就越大, 颏孔前方倾斜种植体所需要的骨宽度就越大。同时, 方圆形颌弓的A-P距离越小, 所能支持的远中悬臂梁就越短, 整体恢复的牙弓长度也越短, 再加上远中种植体倾斜角度也受限, 所需骨宽度更多, 因此, 方圆形颌弓是无牙颌整体支架式种植固定修复的不利因素(种植体植入在颏孔间区)。
本研究的样本量较少, 对各类颌弓形态所占百分比的评价还需更大的样本量才能获得更接近整体人群的真实数据。研究中所采用的颌弓形态判定方法以颏孔水平为准, 在临床上很多无牙颌患者从颏孔到牙槽嵴顶尚有剩余牙槽嵴存留, 因此在实际植入位点设计时, 还可有一定的宽容度。尽管有医师指出在“ All-on-4” 类种植固定修复设计中需要在上、下颌大量去骨以形成牙合台[20], 但真正的植入位点还需要在临床上根据患者的个体情况做出个性化判定。
综上所述, 下颌无牙颌患者前部颌弓形态分类中以卵圆形最多, 尖圆形次之, 方圆形最少。方圆形颌弓中女性多于男性, 卵圆形和尖圆形与性别无明显相关。A-P距离越小, 颌弓越呈方圆形, 颏孔前方颌弓拐角就越大, 远中种植体所需要的骨宽度就越大。下颌无牙颌患者的“ All-on-4” 类种植固定修复前应评估前部颌弓形态, 设计远中种植体的合理倾角, 远中种植位点的骨宽度应格外充足。方圆形颌弓是“ All-on-4” 类种植固定修复的不利因素。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|