







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
多重竞争性荧光PCR检测X连锁Alport综合征大片段缺失突变
[王芳, 张琰琴, 丁洁 , 俞礼霞]
, 俞礼霞]
, 俞礼霞]
|
|


目的 探讨多重竞争性荧光PCR在X连锁Alport综合征分子诊断中的应用。方法 选择20例在北京大学第一医院确诊且未进行基因诊断的X连锁Alport综合征患者为研究对象,同时选择2例经多重连接依赖性探针扩增技术检测到 COL4A5基因大片段缺失突变的患者作为阳性对照和1例经肾活检组织电子显微镜检查证实非Alport综合征的男性作为正常对照。首先应用多重竞争性荧光PCR技术扩增 COL4A5基因53个外显子和4个参照基因,对于检测到 COL4A5基因缺失第1外显子者,进而应用相同技术扩增 COL4A5基因外显子1~4、 COL4A6基因外显子1~4、两基因共用启动子以及3个参照基因;对于检测到拷贝数缺失者,应用琼脂糖凝胶电泳鉴定扩增后的PCR产物或直接测序。结果 两例阳性对照应用多重竞争性荧光PCR技术检测到的 COL4A5基因缺失突变与应用多重连接依赖性探针扩增技术检测到的 COL4A5基因缺失突变一致。20例患者中6例(30%)明确了基因型,其中2例患者具有累及 COL4A5和 COL4A6两个基因5'端的大片段缺失,2例患者具有累及 COL4A5基因30个外显子以上的大片段缺失,1例患者具有累及 COL4A5基因至少1个外显子的大片段缺失,1例患者具有 COL4A5基因缺失13个碱基的小的缺失突变,未检测到重复突变。结论 多重竞争性荧光PCR技术可用于检测X连锁 Alport 综合征大片段缺失突变,是对该病分子诊断检测方法的重要补充。
Objective: To evaluate the ability of multiplex competitive fluorescence polymerase chain reaction in detection of large deletion and duplication genotypes of X-linked Alport syndrome.Methods: Clinical diagnosis of X-linked Alport syndrome was based on either abnormal staining of type Ⅳ collagen α5 chain in the epidermal basement membrane alone or with abnormal staining of type Ⅳ collagen α5 chain in the glomerular basement membrane and Bowman’s capsule/ultrastructural changes in the glomerular basement membrane typical of Alport syndrome. A total of 20 unrelated Chinese patients (13 males and 7 females) clinically diagnosed as X-linked Alport syndrome were included in the study. Their genotypes were unknown. Control subjects included a male patient with other renal disease and two patients who had large deletions in COL4A5 gene detected by multiplex ligation-dependent probe amplification. Genomic DNA was isolated from peripheral blood leukocytes in all the participants. Multiplex competitive fluorescence polymerase chain reaction was used to coamplify 53 exons of COL4A5 gene and four reference genes in a single reaction. When a deletion removed exon 1 of COL4A5 gene was identified, the same method was used to coamplify the first 4 exons of COL4A5 and COL4A6 genes, a promoter shared by COL4A5 and COL4A6 genes, and three reference genes in a single reaction. Any copy number loss suggested by this method was verified by electrophoresis of corresponding polymerase chain reaction amplified products or DNA sequencing to exclude possible DNA variations in the primer regions.Results: Genotypes of two positive controls identified by multiplex competitive fluorescence polymerase chain reaction were consistent with those detected by multiplex ligation-dependent probe amplification. Deletions were identified in 6 of the 20 patients, including two large deletions removing the 5' part of both COL4A5 and COL4A6 genes with the breakpoint located in the second intron of COL4A6, two large deletions removing more than 30 exons of COL4A5 gene, one large deletion removing at least 1 exon of COL4A5 gene, and one small deletion involving 13 bps. No duplication was found.Conclusion: Our results show that multiplex competitive fluorescence polymerase chain reaction is a good alternative to classical techniques for large deletion genotyping in X-linked Alport syndrome.
Alport综合征(Alport syndrome, AS)是一种并不罕见的遗传性肾疾病。编码Ⅳ 型胶原α 5链的基因COL4A5或COL4A5和编码Ⅳ 型胶原α 6链的基因COL4A6两个基因突变致X连锁显性遗传AS, 编码Ⅳ 型胶原α 3或α 4链的基因COL4A3或COL4A4突变致常染色体遗传AS, 其中X连锁显性遗传AS最常见, 约占80%。该病患者在疾病早期仅表现为血尿, 随着疾病进展, 逐渐出现蛋白尿、进行性肾功能减退, 且大多数患者于青壮年时期发展至终末期肾病, 需要透析和肾移植治疗。此外, 部分患者可以出现感音神经性耳聋和眼部异常, 极少数患者出现食管、支气管树等处的弥漫性平滑肌瘤, 由此可见AS是一种预后差、危害极大的慢性肾病, 给社会和家庭带来沉重的负担。已有研究显示, 基因诊断除了有利于AS患者的诊断、客观地为患者及其家系提供遗传和婚育咨询外, 且有利于指导患者相应治疗[1, 2, 3]。在已报道的众多COL4A5基因突变中, 大片段缺失突变为3.0%~19.5%[1, 2, 4, 5, 6]。如何能够简单、快捷、高通量的检测出这些大片段缺失突变是对AS进行分子诊断不可缺少的一个重要环节。目前基于多重聚合酶链反应(polymerase chain reaction, PCR)的多重连接依赖性探针扩增(multiplex ligation-dependent probe amplification, MLPA)技术是检测基因大片段缺失和重复的主要技术手段[7], 因此以往我们和其他研究者应用MLPA检测COIAA5基因大片段缺失突变[8, 9, 10, 11, 12, 13]。然而, 一次MLPA实验需要1~3 d以完成过夜分子杂交、PCR扩增和毛细管电泳3个步骤, 且反应体系因多步骤操作受到污染的机会大。多重竞争性荧光PCR技术与MLPA高度接近, 但是前者与后者的重要区别在于前者仅PCR扩增和毛细管电泳两个步骤, 花费时间不足1 d, 从而不但大大减少了工作量和时间, 而且降低了反应体系受污染的机会[7]。鉴于此, 本研究应用多重竞争性荧光PCR技术检测分析COL4A5基因53个外显子和COL4A6基因第1~4外显子, 旨在补充X连锁显性遗传AS大片段缺失和重复突变检测方法。
X连锁显性遗传AS临床诊断标准为:(1)皮肤基底膜Ⅳ 型胶原α 5链间接免疫荧光染色异常; (2)肾小球基底膜和包曼氏囊Ⅳ 型胶原α 5链间接免疫荧光染色异常; (3)肾活检组织电子显微镜检查示肾小球基底膜呈典型AS改变。选择1996年12月至2013年7月北京大学第一医院住院和门诊患者中符合上述3种诊断标准中的(1)或(1)+(2)或(1)+(3)而确诊为X连锁显性遗传AS、且未进行基因诊断的患者20例(男13例, 女7例), 其中符合诊断标准中(1)者16例、(1)+(2)者1例以及(1)+(3)者3例。这些患者就诊北京大学第一医院时表现为血尿者6例、血尿伴蛋白尿者14例, 14例进行肾功能评估的患者中出现肾功能下降甚至终末期肾病者7例, 8例进行眼部检查的患者中2例表现为白内障(年龄分别为6岁和9.5岁), 11例进行纯音测听检查的患者中7例表现为感音神经性耳聋, 仅1例患者9岁因出现吞咽困难进而发现食管平滑肌瘤(其母表现为血尿伴少量蛋白尿, 亦有食管平滑肌瘤病史)。20例患者中17例有血尿或终末期肾病家族史。
与此同时, 选择2例(男、女各1例)经MLPA检测到COlAA5基因大片段缺失突变的患者作为本研究阳性对照, 1例经肾活检组织电子显微镜检查证实非Alport综合征的男性作为本研究的正常对照。
本试验获得北京大学第一医院临床研究伦理委员会批准, 研究对象包括患者和对照或其父母均签署知情同意书。
参照以往我们采用的方法[8]提取全部研究对象的外周血基因组DNA。采用多重竞争性荧光PCR技术(AccuCopyTM多重基因拷贝数检测试剂盒, 上海天昊生物科技有限公司)对所纳入研究对象的COL4A5基因(NM_000495.3)53个外显子共46个区段和4个参照基因(POP1、POLR2A、RPP14和TBX15)进行拷贝数检测。对于检测到COL4A5基因缺失第1外显子者, 进而应用相同技术扩增COL4A5基因外显子1~4、COL4A6基因(NM_033641.2)启动子(与COL4A5基因共用)和外显子1~4以及3个参照基因(10号染色体短臂31120531-31120675, 20号染色体长臂35865921-35866142, 16号染色体短臂25258129-25258426)。AccuCopyTM多重基因拷贝数检测技术原理参照Du等[14]的报道。根据试剂盒说明进行PCR扩增:取2 μ L样本DNA(浓度20 g/L)与2 μ L竞争DNA混合液混匀后, 加入10 μ L 2× PCR Master Mix、1 μ L多重PCR引物混合液以及5 μ L 无菌蒸馏水。PCR循环程序:95 ℃ 10 min, 94 ℃ 20 s、65~0.5 ℃/循环 40 s、72 ℃ 90 s循环11圈、94 ℃ 20 s、59 ℃ 30 s、72 ℃ 90 s循环24圈、60 ℃ 1 min。取1 μ L PCR产物稀释为5%后, 取1 μ L 与0.5 μ L 500 LIZTM Size Standard、8.5 μ L Hi-Di 混匀, 95 ℃变性5 min后用ABI3130XL测序仪进行毛细管电泳, 利用 GeneMapper 4.0对ABI3130XL测序仪生成的数据文件进行分析, 输出所有特异产物峰的峰高以及峰面积。计算每个靶片段及参照基因的样本峰高与竞争DNA峰高比值(S/I), 分别用参照基因S/I值对靶片段S/I值进行校正后获取靶片段的准确拷贝数。如果某个参照基因校正后的S/I值偏离其他参照基因校正后的S/I值25%以上, 则该参照基因被排除, 不用做进一步分析。参照基因的拷贝数均为2, 每个靶片段的拷贝数为平均S/I值乘以2。
对于检测到有缺失信号的样本, 进而应用2%(质量分数)琼脂糖凝胶电泳鉴定扩增相应外显子的PCR产物或直接测序, 以排除引物区域可能的变异。引物设计及 PCR 扩增条件同我们以前的报道[15, 16]。
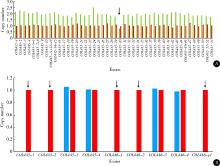
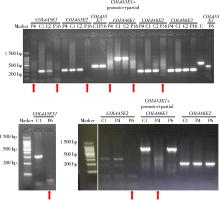
以往我们的研究显示[8], 阳性对照1(女)其子经MLPA检测到缺失COL4A5基因第30外显子, 而阳性对照1表现为血尿伴蛋白尿, 故推测其基因型为COL4A5基因第30外显子杂合缺失; 阳性对照2(男)经MLPA检测到缺失COL4A5基因外显子1~2和COL4A6基因外显子1~2。多重竞争性荧光PCR技术检测结果显示这两例阳性对照均检测到相应的已知基因型(图1)。
 | 图1 阳性对照多重竞争性荧光聚合酶链反应检测结果Figure 1 Genotypes of positive controls detected by multiplex competitive fluorescence polymerase chain reaction COL4A5/6-n (n=1, 2, 3……) indicates individual COL4A5 or COL4A6 exons; COL4A6-p1 indicates the promoter shared by COL4A5 and COL4A6 genes; the arrow indicates deleted exons; red indicates normal control; green indicates positive control 1; blue indicates positive control 2. A, genotype of positive control 1; B, genotype of positive control 2. |
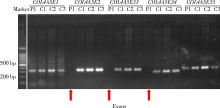
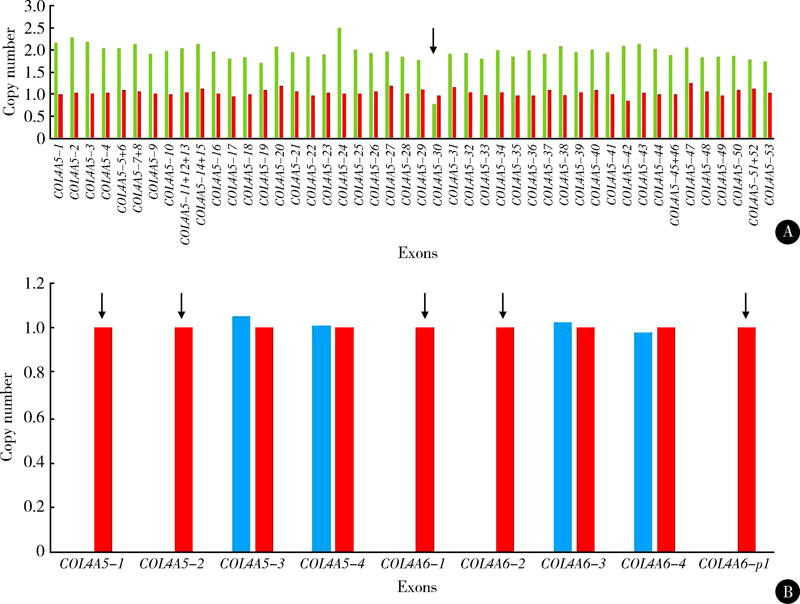
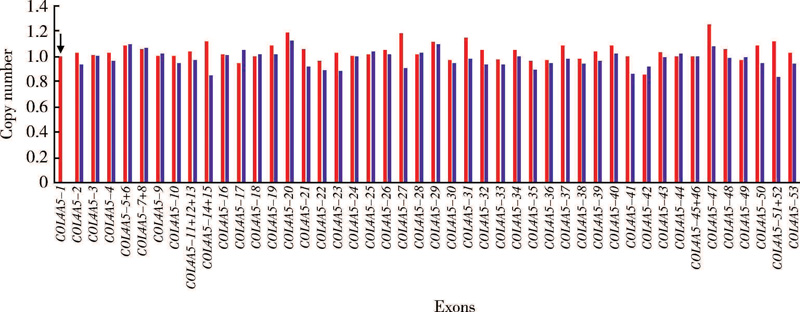
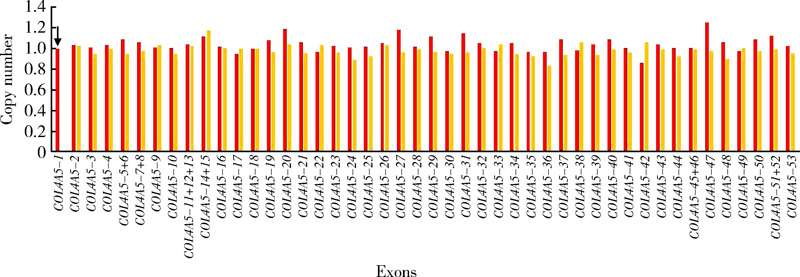
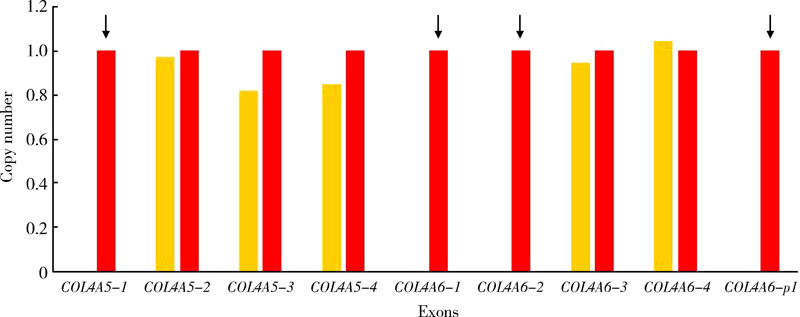
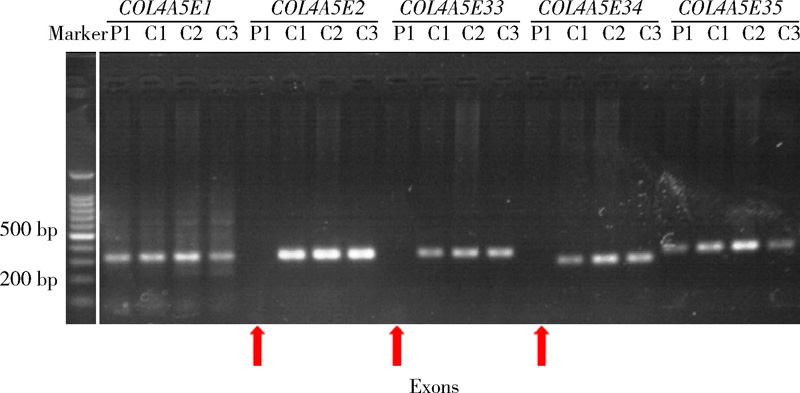
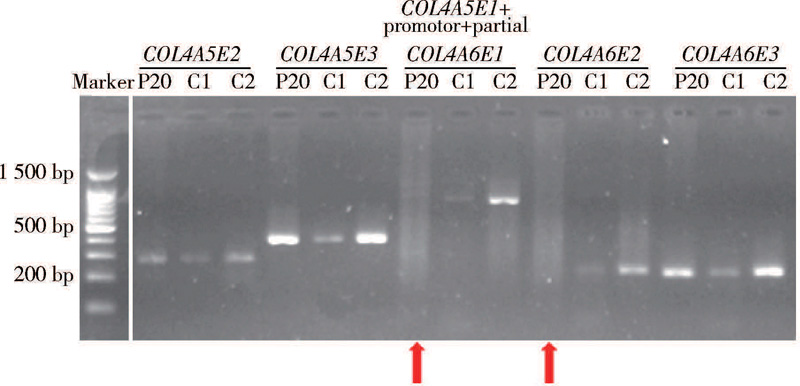
在20例X连锁型AS患者中(图2~14), 7例患者经多重竞争性荧光PCR技术检测到COL4A5基因异常(图2、3、5、6、8和10):患者1缺失外显子2~34, 患者4和患者20缺失外显子1, 患者6缺失外显子2~53, 患者10和患者18分别在外显子14~15和外显子24的数据明显异常于正常对照, 患者16缺失外显子1~2。对患者4、16和20进一步应用多重竞争性荧光PCR技术检测分析COL4A5基因和COL4A6基因, 结果显示患者4除缺失COL4A5基因外显子1外, COL4A6基因启动子的数据明显异常于正常对照(图4); 患者16缺失COL4A5基因外显子1~2以及COL4A6基因启动子和外显子1~2(图7); 患者20缺失COL4A5基因外显子1以及COL4A6基因启动子和外显子1~2(图9)。应用琼脂糖凝胶电泳鉴定扩增后的PCR产物显示:成功扩增了患者1的COL4A5基因外显子1和35, 但其COL4A5基因外显子2、33和34无相应扩增产物(图11); 成功扩增了患者4的COL4A5基因外显子2和COL4A6外显子2及3, 但其COL4A5基因外显子1、COL4A6外显子1及两基因共用启动子无相应扩增产物(图12); 成功扩增了患者6 的COL4A5基因外显子1、COL4A6基因外显子1~2及两基因共用启动子, 但其COL4A5基因外显子2和51无相应扩增产物(图12); 成功扩增了患者16的COL4A5基因外显子3和COL4A6外显子3, 但其COL4A5基因外显子1~2和COL4A6外显子1~2以及两基因共用启动子无相应扩增产物(图12); 成功扩增了患者20的COL4A5基因外显子2~3和COL4A6外显子3, 但其COL4A5基因外显子1、COL4A6外显子1~2及两基因共用启动子无相应扩增产物(图13)。应用PCR方法分别扩增了患者10和18的COL4A5基因外显子14~15和24, 继而进行直接测序, 结果显示患者10的外显子14~15序列无异常, 而患者18外显子24存在13个碱基的缺失突变(c. 1742-1754del, p.Asp581Glyfs* 33, 图14)。
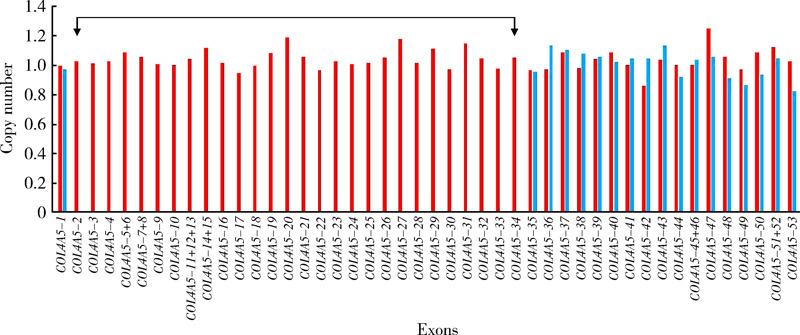 | 图2 患者1多重竞争性荧光聚合酶链反应检测结果Figure 2 Multiplex competitive fluorescence polymerase chain reaction analysis of patient 1 COL4A5-n (n=1, 2, 3……) indicates individual COL4A5 exons; red column indicates normal control, light blue column indicates patient 1; the arrow indicates deleted exons. |
 | 图3 患者4多重竞争性荧光聚合酶链反应检测COL4A5基因结果Figure 3 Multiplex competitive fluorescence polymerase chain reaction analysis of COL4A5 gene in patient 4 COL4A5-n (n=1, 2, 3……) indicates individual COL4A5 exons; red column indicates normal control, purple column indicates patient 4; the arrow indicates deleted exons. |
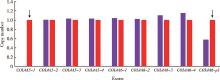
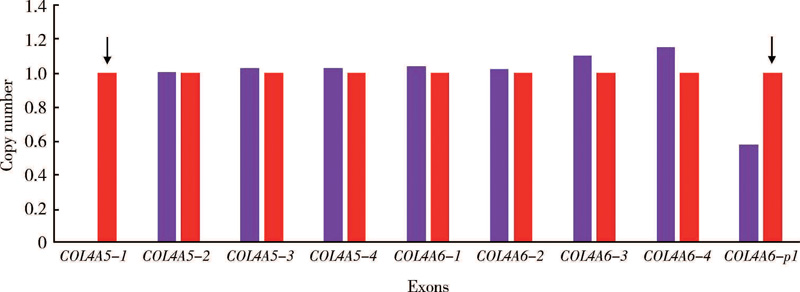 | 图4 患者4多重竞争性荧光聚合酶链反应检测COL4A5和COL4A6基因结果Figure 4 Multiplex competitive fluorescence polymerase chain reaction analysis of COL4A5 and COL4A6 genes in patient 4 COL4A5/6-n (n=1, 2, 3……) indicates individual COL4A5 or COL4A6 exons; COL4A6-p1 indicates the promoter shared by COL4A5 and COL4A6 genes; red column indicates normal control, purple column indicates patient 4; the arrow indicates deleted exons. |
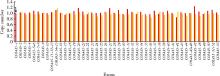
 | 图5 患者6多重竞争性荧光聚合酶链反应检测结果Figure 5 Multiplex competitive fluorescence polymerase chain reaction analysis of patient 6 COL4A5-n (n=1, 2, 3……) indicates individual COL4A5 exons; red column indicates normal control, navy blue column indicates patient 6; the arrow indicates deleted exons. |
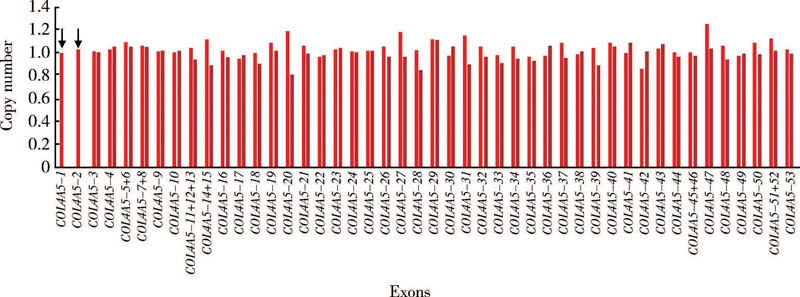 | 图6 患者16多重竞争性荧光聚合酶链反应检测COL4A5基因结果Figure 6 Multiplex competitive fluorescence polymerase chain reaction analysis of COL4A5 gene in patient 16 COL4A5-n (n=1, 2, 3……) indicates individual COL4A5 exons; red column indicates normal control, deep red column indicates patient 16; the arrow indicates deleted exons. |
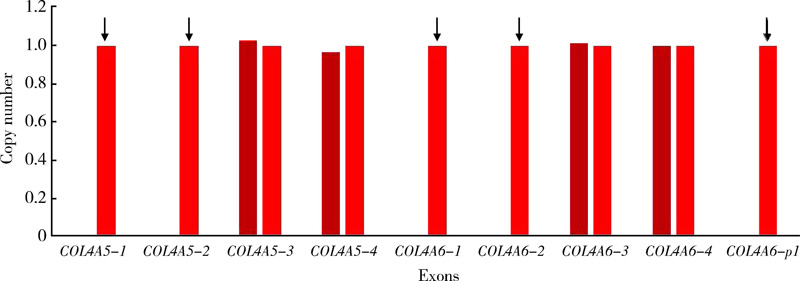 | 图7 患者16多重竞争性荧光聚合酶链反应检测COL4A5和COL4A6基因结果Figure 7 Multiplex competitive fluorescence polymerase chain reaction analysis of COL4A5 and COL4A6 genes in patient 16 COL4A5/6-n (n=1, 2, 3……) indicates individual COL4A5 or COL4A6 exons; COL4A6-p1 indicates the promoter shared by COL4A5 and COL4A6 genes; red column indicates normal control, deep red column indicates patient 16; the arrow indicates deleted exons. |
 | 图8 患者20多重竞争性荧光聚合酶链反应检测COL4A5基因结果Figure 8 Multiplex competitive fluorescence polymerase chain reaction analysis of COL4A5 gene in patient 20 COL4A5-n (n=1, 2, 3……) indicates individual COL4A5 exons; red column indicates normal control, orange column indicates patient 20; the arrow indicates deleted exons. |
 | 图9 患者20多重竞争性荧光聚合酶链反应检测COL4A5和COL4A6基因结果Figure 9 Multiplex competitive fluorescence polymerase chain reaction analysis of COL4A5 and COL4A6 genes in patient 20 COL4A5/6-n (n=1, 2, 3……) indicates individual COL4A5 or COL4A6 exons; COL4A6-p1 indicates the promoter shared by COL4A5 and COL4A6 genes; red column indicates normal control, orange column indicates patient 20; the arrow indicates deleted exons. |
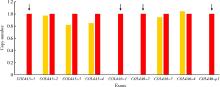
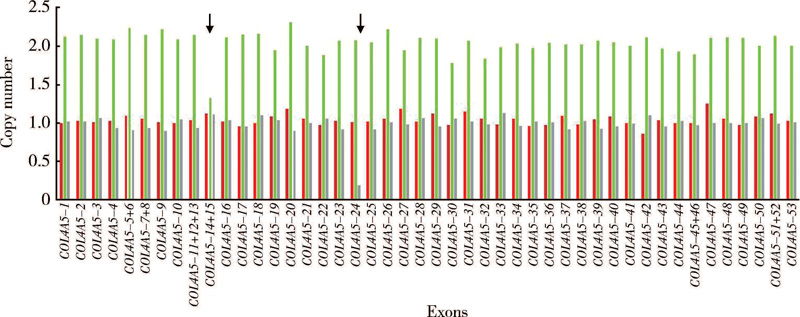 | 图10 患者10和18多重竞争性荧光聚合酶链反应检测结果Figure 10 Multiplex competitive fluorescence polymerase chain reaction analysis of patients 10 and 18 COL4A5-n (n=1, 2, 3……) indicates individual COL4A5 exons; red column indicates normal control, green column indicates patient 10, and gray column indicates patient 18; the arrow indicates exons having abnormal signal or the breakpoint of a deletion. |
 | 图11 患者1琼脂糖凝胶电泳检测结果Figure 11 Agrose gel electrophoresis of patient 1 COL4A5En (n=1, 2, 3……) indicates individual COL4A5 exons; Mark, 1 kb plus DNA ladder; P, patient; C, control; the arrow indicates deleted exons. |
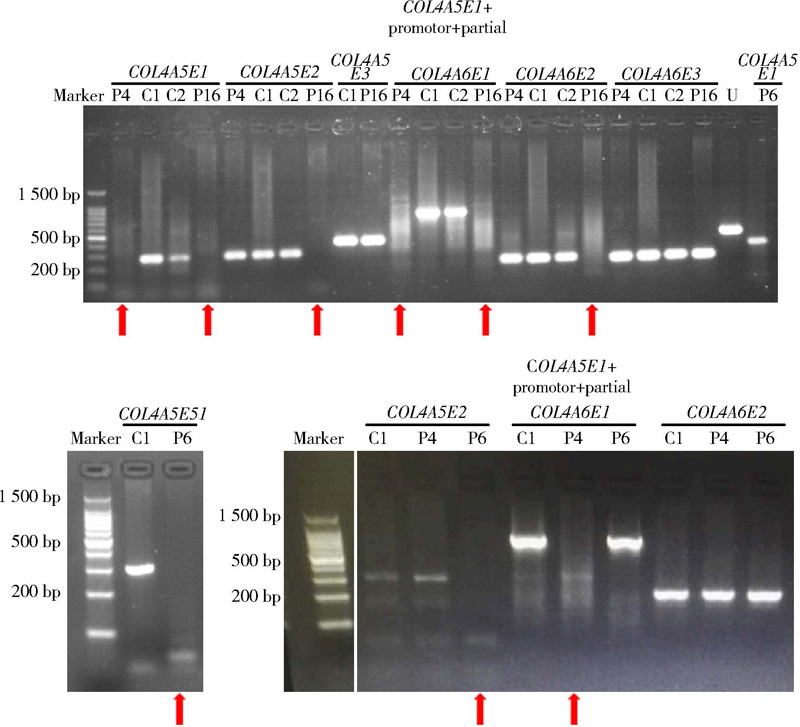 | 图12 患者4、6和16琼脂糖凝胶电泳检测结果Figure 12 Agrose gel electrophoresis of patients 4, 6 and 16 COL4A5/6En (n=1, 2, 3……) indicates individual COL4A5 or COL4A6 exons; Marker, 1 kb plus DNA ladder; P, patient; C, control; U, unrelated sample; the arrow indicates deleted exons. |
 | 图13 患者20琼脂糖凝胶电泳检测结果Figure 13 Agrose gel electrophoresis of patient 20 COL4A5/6En (n=1, 2, 3……) indicates individual COL4A5 or COL4A6 exons; Marker, 1 kb plus DNA ladder; P, patient; C, control; the arrow indicates deleted exons. |
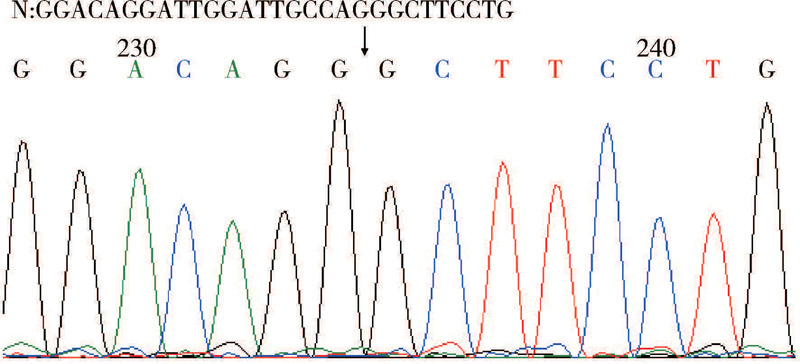 | 图14 患者18直接测序检测结果Figure 14 Direct sequence analysis of PCR amplified product of exon 24 in patient 18 N, normal sequence; the arrow indicates the breakpoint of a deletion. |
2013年发表的关于Alport综合征和薄基底膜肾病专家共识建议将基因诊断作为诊断AS和判断遗传方式的金标准[17], 因此探索新的致病基因检测方法将有助于完善该病基因诊断平台。以往研究显示, COL4A5基因大片段缺失突变可达 3.0%~19.5%[1, 2, 4, 5, 6], 可以应用经典方法如Southern杂交和十余年前发展起来的MLPA技术进行检测[2, 8, 9, 10, 11, 15, 18, 19]。然而, Southern杂交因操作复杂和花费时间长而不适合应用于临床, MLPA技术存在花费时间偏长、反应体系步骤多、操作易受污染等缺点, 因而本研究采用与MLPA高度接近的多重竞争性荧光PCR技术检测了X连锁显性遗传AS患者的COL4A5基因和COL4A6基因, 同时应用琼脂糖凝胶电泳或直接测序验证其检测结果的准确性。
本研究中两例阳性对照应用多重竞争性荧光PCR技术检测到的基因型与应用MLPA检测到的基因型一致, 说明多重竞争性荧光PCR技术用于检测X连锁显性遗传AS大片段缺失突变是可行的。
20例X连锁显性遗传AS患者中, 经多重竞争性荧光PCR技术和琼脂糖凝胶电泳或直接测序明确了基因型者6例, 其中4/6例患者多重竞争性荧光PCR结果提示检测到累及COL4A5基因或COL4A5和COL4A6两个基因的大片段缺失突变, 琼脂糖凝胶电泳结果显示确实未能成功扩增相应外显子; 1/6例患者多重竞争性荧光PCR结果提示缺失COL4A5基因外显子1, 需对COL4A6基因启动子区应用其他方法证实有无异常, 琼脂糖凝胶电泳结果显示其确实缺失COL4A5基因外显子1, 但由于所用引物扩增的片段包括了COL4A5基因外显子1、COL4A6基因启动子区及外显子1部分序列, 因此该片段无相应扩增产物不除外因缺失COL4A5基因外显子1所致, 不能判断出启动子区是否存在缺失; 1/6例患者多重竞争性荧光PCR结果提示需对COL4A5基因外显子24应用其他方法证实有无异常, 进而直接测序显示其缺失13个碱基。此外, 1例患者虽然多重竞争性荧光PCR结果提示COL4A5基因外显子14~15需应用别的方法证实有无异常, 但是直接测序并未检测到异常, 这些研究结果提示多重竞争性荧光PCR检测X连锁显性遗传AS大片段缺失突变具有很高程度的可靠性和准确性, 然而是否适用于20个碱基以内的缺失突变需要增加样本例数以证实。
COL4A5基因大片段缺失突变因检测方法不同检出率存在很大差异, 如来自日本、韩国及以往我们的研究显示, COL4A5基因大片段缺失突变为1%~4%(分别为1/61例、1/25例和3/106例)[2, 5, 6], 而美国患者中COL4A5基因大片段缺失突变为8%(14/175例)[4], 欧洲患者中COL4A5基因大片段缺失突变为19.5%(38/195例)[1]。本研究应用多重竞争性荧光PCR技术检测到COL4A5基因大片段缺失突变者5/20例, 包括累及COL4A5和COL4A6两个基因5'端的大片段缺失者2例, 累及COL4A5基因30个外显子以上的大片段缺失者2例和累及COL4A5基因至少1个外显子的大片段缺失1例, 与来自欧洲的报道[1]类似。
本研究中2例患者检测到的大片段缺失突变累及COL4A5和COL4A6两个基因5'端, 其中患者20因其临床表现除血尿、蛋白尿、终末期肾病、白内障和感音神经性耳聋外, 尚有食道平滑肌瘤表现, 因此未进行基因检测分析前便考虑其基因型为累及COL4A5和COL4A6两个基因的大片段缺失突变, 且COL4A6基因缺失断点在第2内含子中[1, 2, 19], 基因检测结果证实了我们的推测。然而患者18尽管COL4A6基因缺失断点亦在第2内含子中, 但其临床表现为血尿、蛋白尿、肾功能减退、白内障和感音神经性耳聋, 随访至18岁时尚未出现吞咽困难等表现, 因而未进行基因检测分析前并未猜测到其基因型为累及COL4A5和COL4A6两个基因的大片段缺失突变。
总之, 本研究显示多重竞争性荧光PCR可用于X连锁显性遗传AS大片段缺失突变的检测, 是对该病分子诊断检测方法的重要补充。
(志谢:谨此对患者及其家属的配合与支持深表谢意!)
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|