



{kind=link}
{kind=link}
{kind=link}
{kind=link}
锁定钢板治疗非骨质疏松性复杂肱骨近端骨折的中期临床及影像学随访研究
[李旭, 李奉龙, 鲁谊, 朱以明, 郭斯翊, 李屹钧, 姜春岩 ]
]
]
|
|


目的 回顾性分析采用锁定钢板治疗非骨质疏松性三部分和四部分肱骨近端骨折的临床效果。方法 回顾性评估锁定钢板治疗非骨质疏松性三部分和四部分肱骨近端骨折的临床效果,统计患肢的肩关节活动度、临床评分、视觉模拟评分(visual analogue scale,VAS)和影像学检查的结果。结果 自2007年1月至2014年10月,采用锁定钢板共治疗107例新鲜非骨质疏松性三部分和四部分肱骨近端骨折,其中67例患者完成至少2年的随访,平均随访时间(43.9±23.3)个月(24~108个月)。在最终随访时,Constant评分平均为(87.1±11.7)分(51~100分),加州大学肩关节评分(the University of California at Los Angeles shoulder score, UCLA)平均为(30.5±3.9)分(18~35分),VAS疼痛评分为(1±2)分(0~7分);主动前屈上举为159.0°±19.3°(80°~180°),体侧外旋为36.8°±19.5°(0°~80°),体侧内旋为T11水平(T2~LS水平)。术后11例患者出现并发症,包括5例螺钉穿出(7.5%),9例肱骨头缺血坏死(13.4%)及5例创伤性骨性关节炎(7.5%),6例合并两种或两种以上并发症。三部分骨折和四部分骨折术后患者的肩关节活动度、临床评分和VAS疼痛评分差异无统计学意义。四部分骨折的术后并发症率及术后肱骨头缺血坏死概率显著高于三部分骨折。结论 应用肱骨近端锁定钢板治疗非骨质疏松性三、四部分复杂肱骨近端骨折可得到满意的术后肩关节功能恢复,严格的适应证选择与精细的手术操作是取得手术成功的关键,骨折的复杂程度亦对术后结果产生影响,四部分骨折的并发症发生率以及术后肱骨头缺血坏死率高于三部分骨折。
Objective: To describe long-term results of locking plate used for the treatment of non-osteoporotic fresh three- and four-part proximal humeral fractures with at least 2 years follow-up.Methods: The functional outcomes and the complications of non-osteoporotic three- and four-part fresh proximal humeral fractures treated with locking plate were assessed retrospectively. The active range of motion, the Constant score, the University of California at Los Angeles (UCLA) shoulder score, the visual analogue score (VAS) were employed to evaluate the postoperative shoulder function, and the radiographic images were taken to evaluate the neck-shaft angle of the proximal humeral and postoperative implant-related complications.Results: From January 2007 to October 2014, 107 consecutive fresh three- and four-part non-osteoporotic fresh proximal humeral fractures were treated with a locking plate in our department. Among them, 67 patients completed at least 2 years follow-up. The average follow-up time was (43.9±23.3) months (range: 24-108 months). The mean Constant score was 87.1±11.7 (range: 51-100), the mean UCLA score was 30.5±3.9 (range: 18-35), the mean VAS score was 1±2 (range: 0-7). The mean active forward flexion was 159.0°±19.3° (range: 80°-180°), the mean external rotation was 36.8°±19.5°(0°-80°) and the mean internal rotation was T11 level (T2-LS level). There were 11 patients who suffered from complications. Screw perforations were observed in 5 (7.5%) patients, avascular necrosis of the humeral head was observed in 9 (13.4%) patients and traumatic osteoarthritis was observed in 5 (7.5%) patients. Six patients showed two or more complications. There was no significant difference in outcomes when comparing the patients with three-part fractures (31 patients) with those with four-part fractures (36 patients). The rates of complications and avascular necrosis were significantly higher in the four-part fracture group than in the three-part fracture group.Conclusion: The locking plate is an effective method in treating three- and four-part non-osteoporotic fresh proximal humeral fractures. Strict surgical indication and precise surgical skill are the key points for successful treating non-osteoporotic fresh proximal humeral fractures. There is a higher rate of complications and avascular necrosis of the humeral head in the four-part fractures than in the three-part fractures.
肱骨近端骨折在临床工作中非常常见, 约占全身骨折的5%[1]。对于复杂的肱骨近端骨折(Neer分型中的三部分和四部分骨折)的治疗一直存在争议。一些文献报道应用切开复位、锁定钢板固定治疗复杂肱骨近端骨折可获得良好疗效, 但亦有很多研究报道应用锁定钢板治疗骨质疏松性复杂肱骨近端骨折的术后并发症率较高[2, 3, 4, 5, 6, 7, 8]。本研究回顾性分析了北京积水潭医院运动损伤科采用锁定钢板治疗非骨质疏松性三、四部分肱骨近端骨折的病例在中期随访时的临床及影像学结果, 希望能够为优化肱骨近端骨折的治疗选择提供临床依据。
患者的入选标准:(1)新鲜骨折(手术时间距受伤时间不超过4周); (2)术前诊断为Neer三部分或四部分骨折(可同时合并或不合并肱骨头脱位); (3)采用切开复位, 锁定钢板固定; (4)随访超过24个月以上。
患者的排除标准:(1)合并同侧上肢其他需手术治疗的骨骼或肌肉、软组织损伤; (2)合并血管神经损伤的患者; (3)病理性骨折; (4)患者骨骺尚未闭合。
采用切开复位, 锁定钢板固定治疗三、四部分肱骨近端骨折的适应证包括:(1)术中可达到解剖或接近解剖复位; (2)CT显示肱骨头骨折块厚度> 5 mm; (3)无严重骨质疏松者(骨皮质厚度> 6 mm[9])。
采用Tingart等[10]报道的方法评价骨质疏松, 在术前测量患者的肩关节正位X线片, 评估肱骨近端骨皮质的厚度。首先在肱骨头下方确认肱骨近端内侧骨皮质外缘和外侧骨皮质开始变得平行的点, 经此点作垂直于内侧骨皮质外缘和外侧骨皮质的垂线, 在此线上测量整个骨干的直径(M1), 即内侧骨皮质内缘至外侧骨皮质外缘的距离; 然后在此线上测量整个髓腔的直径(M2), 即内侧骨皮质外缘至外侧骨皮质内缘的距离, 此时骨皮质的厚度=M1-M2; 最后在距离此线以远20 mm处, 以相同方法测量此处的骨皮质厚度(M3-M4), 取两次骨皮质厚度的平均值, 即为该患者肱骨近端骨皮质的厚度(图1)。
患者置于沙滩椅位, 经三角肌-胸大肌入路逐层切开显露骨折端, 辨认大小结节, 以5号聚酯不可吸收缝合线(商品名:爱惜邦)分别穿过冈上、冈下肌及肩胛下肌作为牵引线。透视下复位颈干角, 角度满意后以1或2枚螺纹导针穿过肱骨干及肱骨头作为临时固定。在结节间沟外侧放置解剖钢板(Philos, Proximal Humeral Internal Locking Plate, Synthes, Oberdorf, Switzerland或LPHP, Locking Proximal Humerus Plate, Synthes, Oberdorf, Switzerland)并打入锁定螺钉以固定骨折。固定过程中, 我们特别注意在贴近肱骨头外科颈的内侧皮质内置入支撑螺钉(calar screw), 以保证足够的内侧支撑。螺钉置入后, 必须在多个体位透视下确认螺钉未穿出肱骨头(图2)。透视确认骨折复位及钢板、螺钉位置满意后, 以多个纵行及横行张力带方式缝合加强固定大小结节, 或视大小结节骨质情况附加钛缆作加强固定。将切断的长头腱缝合到联合腱和胸大肌上后, 逐层关闭切口。
患肢以颈腕吊带固定至术后6周。术后第2天开始, 患者需在理疗师指导下进行肩关节被动活动练习。手术后6周开始辅助的主动活动, 3个月开始完全的主动活动练习, 术后6个月确定骨折愈合后开始肌力训练。
临床评估:要求患者在术后1年及此后每整年时复查。所有患者在最终随访时记录患肢的肩关节活动度(前屈上举、体侧外旋和内旋), 并以Constant评分、加州大学肩关节评分(the University of California at Los Angeles shoulder score, UCLA)和视觉模拟评分(visual analogue scale, VAS)对患者的肩关节功能及疼痛情况加以评估。
影像学评估:术前及随访过程中均拍摄患者肩胛骨正位(保证肱骨近端处于旋转中立位)、侧位及腋位(或改良腋位)X线片。根据术前X线片采用Neer肱骨近端骨折分型系统对患者的骨折进行分型; 根据术后即刻X线片在肩胛骨正位片上测量肱骨近端颈干角, 并在各个角度的X线片上观察是否存在螺钉穿出肱骨头关节面的情况; 根据术后随访时的X线片评估骨折愈合情况, 同时观察是否存在肱骨头缺血坏死、螺钉穿出肱骨头关节面及创伤后关节炎等情况。还需要测量随访时肱骨近端颈干角, 并与术后即刻时颈干角对比, 以评估术后骨折复位丢失情况。
 | 图1 骨皮质厚度的确定Figure 1 Measurement for the cortical bone thickness |
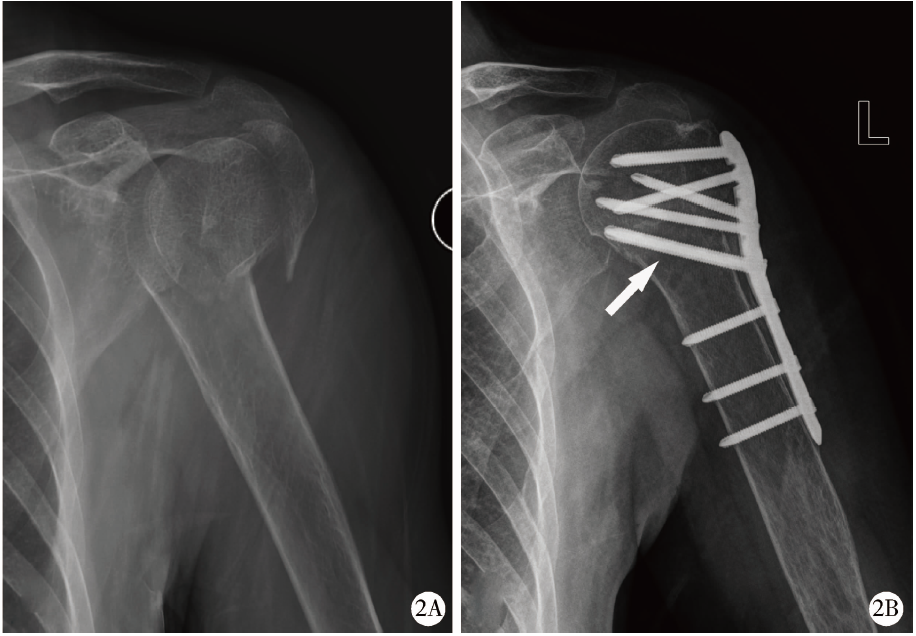 | 图2 61岁女性患者, 走路时摔伤致左肱骨近端骨折, 为经典三部分骨折Figure 2 A 61 years old female, fell down and injured her left arm, the true anterior-posterior view showed proximal humeral fracture (classical three-part fractures) M1 and M3, the thickness of the entire bone; M2 and M4, the width of the intramedullary canal; (M1-M2+M3-M4)/2, the cortical bone thickness. 2A, preoperative anterior-posterior view showed classical three-part proximal humeral fractures; 2B, postoperative anterior-posterior view, note the position of the calar screw (white arrow). |
数据结果以SPSS 13.0软件(Chicago, Illinois)进行分析。对患者的性别、患侧别和并发症情况采用χ 2检验, 对患者的年龄、患肢活动度、临床评分和骨皮质厚度进行秩和检验, 对即刻颈干角和最终随访时的颈干角进行配对t检验。以P< 0.05为差异有统计学意义。
自2007年1月至2014年10月, 共收治三部分和四部分肱骨近端骨折456例, 其中107例新鲜的三部分或四部分骨折采用切开复位、锁定钢板固定治疗。依据本研究的入选及排除标准, 最终入组67例患者(62.6%)。患者平均年龄为(47.1± 14.8)岁(18~82岁), 平均随访时间(43.9± 23.3)个月(24~108个月), 其中男性43例, 女性24例; 主力侧65例, 非主力侧2例; 左侧36例, 右侧31例。患者受伤距手术时间平均为(10.6± 3.4) d(7~16 d)。三部分骨折31例, 四部分骨折36例, 其中经典三部分骨折23例, 三部分骨折脱位8例, 经典四部分骨折7例, 四部分骨折脱位7例, 四部分外展嵌插型22例。
最终随访时, 患者肩关节前屈上举平均为 159.0° ± 19.3° (80° ~180° ), 体侧外旋为36.8° ± 19.5° (0° ~80° ), 体侧内旋为T11水平(T2~LS水平)。术后UCLA肩关节评分平均为(30.5± 3.9)分(18~35分), Constant评分平均为(87.1± 11.7)分(51~100分), VAS评分平均为(1± 2)分(0~7分)。
所有患者患侧肱骨近端骨皮质厚度平均为(7± 1) mm(6~13 mm)。术后即刻正位片显示颈干角为141° ± 10° (119° ~169° ), 最终随访时正位片显示颈干角为139° ± 12° (114° ~174° ), 两者之间差异无统计学意义(P=0.158, 表1)。
最终随访时, 65例(97.0%)骨折愈合, 2例(3.0%)不愈合, 其中1例术后早期出现深部感染, 经清创并取出内固定后伤口愈合, 1例术后大结节移位且未愈合, 患者拒绝进一步手术治疗。
| 表1 不同骨折分型即刻颈干角和最终颈干角的比较 Table 1 Comparison of neck-shaft angle measured immediately after surgery and in the final follow-up for different fracture types |
11例(16.4%)患者出现术后并发症, 其中6例出现两种或两种以上并发症。术后切口血肿1例, 螺钉穿出肱骨头关节面5例(7.5%), 肱骨头缺血坏死9例(13.4%), 创伤性关节炎5例(7.5%), 术后感染1例。
按骨折分型统计, 三部分骨折患者中2例出现并发症(3.0%), 其中包括1例螺钉穿出肱骨头关节面和1例肱骨头缺血坏死合并创伤性关节炎。四部分骨折患者中9例(13.4%)出现并发症, 其中经典四部分骨折3例, 包括1例肱骨头缺血坏死, 2例肱骨头缺血坏死合并螺钉穿出并继发创伤性关节炎; 四部分骨折脱位2例, 1例肱骨头缺血坏死, 1例螺钉穿出; 四部分外展嵌插型4例, 1例肱骨头缺血坏死, 1例肱骨头缺血坏死合并螺钉穿出, 2例肱骨头缺血坏死继发创伤性关节炎(图3、4, 表2)。
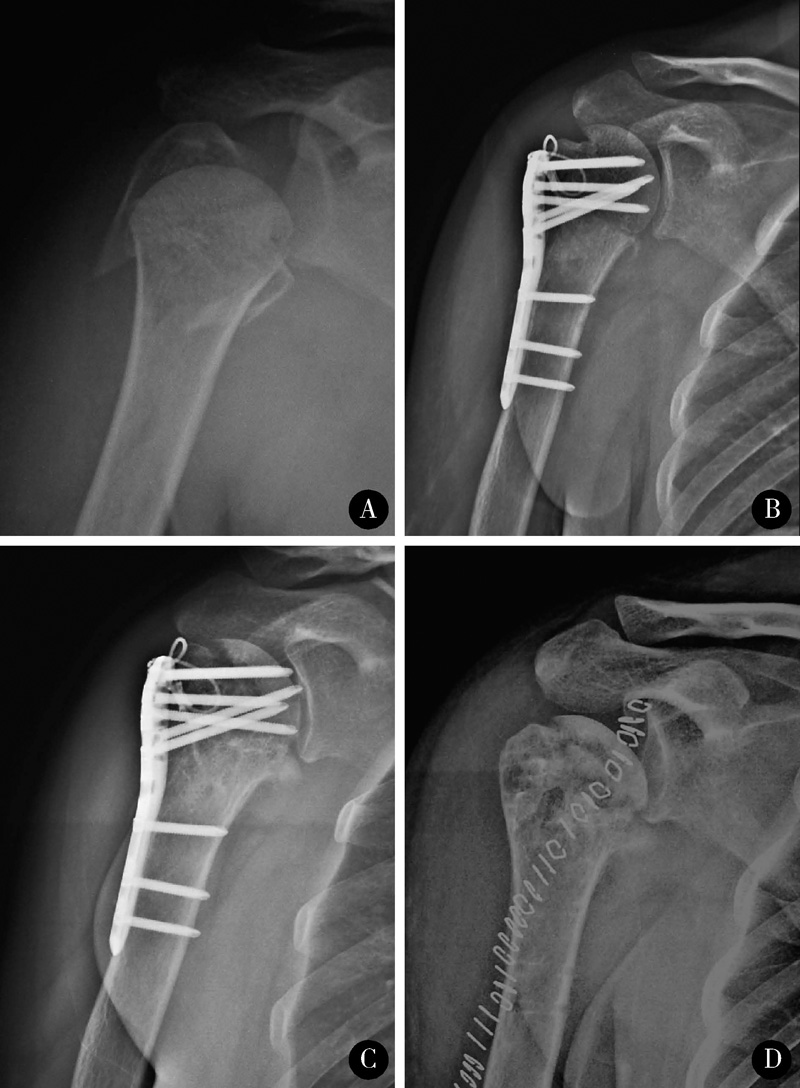 | 图3 42岁女性患者, 车祸致右肱骨近端骨折, 为四部分外展嵌插型Figure 3 A 42 years old female, involved in an traffic accident and injured her right arm, the true anterior-posterior view showed proximal humeral fracture (four-part valgus impaction fractures) A, preoperative true anterior-posterior view showed four-part valgus impaction proximal humeral fractures; B, postoperative true anterior-poste-rior view showed good reduction and fixation; C, 6 months postoperative true anterior-posterior view showed screw perforation, the penetrated screws were removed; D, all implant were removed 1 year postoperatively. |
 | 图4 32岁患者女性, 走路摔伤致左肱骨近端骨折Figure 4 A 32 years old female, fell down and injured her left arm, the true anterior-posterior view showed proximal humeral fracture A, preoperative true anterior-posterior view showed four-part valgus impaction proximal humeral fractures; B, postoperative true anterior-posterior view showed good reduction and fixation; C, avascular necrosis and traumatic osteoarthritis were observed 5 years postoperatively. |
本组患者中三部分骨折和四部分骨折患者在年龄、性别、患侧别和随访时间上差异均没有统计学意义(P> 0.05), 两组患者术后的患肢活动度、Constant评分、UCLA评分和VAS疼痛评分上差异也均无统计学意义(P> 0.05, 表2), 但两组在并发症发生率与术后肱骨头坏死发生率上, 四部分骨折组明显高于三部分骨折组(P< 0.05, 表3)。
| 表2 不同骨折分型的比较 Table 2 Comparison between three- and four-part fractures |
| 表3 不同骨折类型术后并发症的比较 Table 3 Comparison of complications between three- and four-part fractures |
锁定钢板的出现为复杂肱骨近端骨折的治疗带来革命性进展[11], 很多研究报道其治疗满意率很高。Sproul等[3]对以往文献进行了回顾性分析, 发现采用锁定钢板治疗肱骨近端骨折的骨折愈合率高达 96.6%, 术后Constant评分平均为73.6分。Brunner等[7]对158例患者进行平均12个月的随访, Constant评分平均为72分。
也有较多文献报道锁定钢板治疗复杂肱骨近端骨折的并发症发生率较高[2, 3, 5, 6, 7, 8, 12, 13, 14, 15, 16, 17]。Sproul等[3]的回顾性综述显示, 514例患者中, 总体并发症发生率高达48.8%, 其中, 内翻畸形占16.3%, 肱骨头缺血坏死占10.8%。Owsley等[2]随访了53例患者, 19例(36%)出现并发症, 包括12例(23%)螺钉穿出、13例(25%)内翻畸形和2例(4%)肱骨头缺血坏死。Brunner等[7]报道158例患者的并发症发生率为44%, 主要包括螺钉穿出(22%)和肱骨头缺血坏死(8%)等。
许多研究探讨了可能影响手术效果的原因。Krappinger等[4]的研究发现, 骨折后的肱骨头骨质疏松情况[骨密度(bone mineral density, BMD)]显著影响锁定钢板治疗肱骨近端骨折的成功率。Gardner等[18]认为, 锁定钢板的螺钉和钢板间界面强大的抵抗屈服应力的作用, 会将应力传递给螺钉-骨界面, 导致螺钉穿出, 若患者同时合并骨质疏松, 则这个作用就会更明显。还有许多研究表明, 复杂肱骨近端骨折锁定钢板固定术后的复位丢失与骨质疏松程度密切相关[2, 3, 4, 5, 6, 18]。
由此可见, 术前骨质疏松是影响复杂肱骨近端骨折切开复位、锁定钢板固定疗效的重要原因, 因而在选择适应证时应强调患者需具备良好的骨质(肱骨头骨折块厚度> 5 mm, 骨皮质厚度> 6 mm)。本研究中复杂肱骨近端骨折的患者中相当一部分(217/456例, 47.6%)由于合并严重骨质疏松而采用了人工肩关节置换的治疗方式, 这大大降低了患者并发症的发生率, 提高了患者的临床疗效。从本研究结果看, 应用肱骨近端锁定钢板治疗非骨质疏松性新鲜三、四部分复杂肱骨近端骨折可得到满意的疗效。
本研究根据肱骨近端骨皮质厚度来评价局部骨质情况。Virtima等[19]早在1962年就研究确认肱骨近端骨皮质与局部骨量相关。Tingart等[10]也发现X线片上测量的肱骨近端骨皮质厚度与肱骨近端双能X线吸收测定法(dualenergy X-ray absorptiometry, DXA)的结果有很好的相关性。Mather等[9]将肱骨近端骨皮质厚度与股骨、腰椎的DXA进行相关性分析后发现, 当肱骨近端骨皮质厚度的阈值为6 mm时, 其对判断骨质疏松的敏感性为93%, 阴性预测值可达95%。本研究中所有患者肱骨近端的骨皮质厚度平均为(7± 1) mm(6~13 mm), 根据本研究严格的适应证选择, 只有同时肱骨头骨块厚度> 5 mm 时, 我们才会采用锁定钢板治疗。
虽然本组病例的术后并发症发生率明显低于大多数文献报道的结果, 但仔细分析可以发现, 四部分骨折的术后并发症发生率显著高于三部分骨折, 四部分骨折术后最常见的并发症为肱骨头缺血坏死, 其发生率显著高于三部分骨折组。由此可见, 四部分骨折对肱骨头血运的破坏更加显著, 可明显增加术后肱骨头缺血坏死率, 医师需要在术前对此有足够重视并与患者进行充分沟通。
本研究存在以下局限性:首先, 本研究是回顾性研究, 还需要设计前瞻性研究, 以进一步明确锁定钢板在治疗非骨质疏松性三部分和四部分骨折中的作用; 其次, 未设置对照组, 如果能把本组患者与存在骨质疏松的患者进行对比, 可以更好地说明锁定钢板在治疗非骨质疏松性三部分和四部分肱骨近端骨折中的优势; 第三, 未采用股骨或腰椎的DXA进行骨质评估, 但根据肱骨近端骨皮质厚度评价局部骨质情况的方法已经得到公认, 且股骨或腰椎的DXA并不能反映骨折部位骨质的真实情况; 第四, 本组病例的失访率较高, 尽管患者平均随访时间43个月, 但仍属早中期随访, 随访时间仍不足以评估中远期疗效(尤其是创伤性骨性关节炎的评估), 而且在进行并发症对比时, 有并发症患者的随访时间明显长于没有并发症的患者, 因此, 如果进一步增加随访时间, 也会对结果产生一定影响。
综上所述, 应用肱骨近端锁定钢板治疗非骨质疏松性新鲜三、四部分复杂肱骨近端骨折可得到满意的术后肩关节功能恢复, 严格的适应证选择与精细的手术操作是取得手术成功的关键。骨折的复杂程度亦对术后结果产生影响, 四部分骨折与三部分骨折相比, 并发症发生率以及术后肱骨头缺血坏死率更高。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|