


{kind=link}
{kind=link}
{kind=link}
美克尔憩室癌变及肝多发转移并消化道出血1例
[赵轶国, 杨晓东△  , 张雁凯, 宁宁, 邢兆东, 叶颖江]
, 张雁凯, 宁宁, 邢兆东, 叶颖江]
, 张雁凯, 宁宁, 邢兆东, 叶颖江]
|
|


SUMMARY Meckel’s diverticulum is the most common congenital anomaly of the gastrointestinal tract; affecting approximately 2% of the population. It is a true diverticulum occurring on the anti-mesenteric border of the distalileum typically within 100 cm of the ileo-caecal valve. Neoplasms arising in Meckel’s diverticula are uncommon; and those reported in the literature are mainly carcinoid tumors followed by gastrointestinal stromal tumors (GIST) and benign leiomyomas. Adenocarcinomas are extremely rare. Tumors in Meckel’s present non-specifically with gastrointestinal complaints; such as bleeding obstruction inflammation or perforation. The suspicion of a Meckel’s tumor is often not thought of at the initial. In this article we describe a 57-year-old woman who presented with massive rectal bleeding and severe anemia; later found to be caused by a adenocarcinoma arising from Meckel’s diverticulum. The tumor was unfortunately highly aggressive. Multiple liver metastases had already existed when we discovered the primary mass. Later we performed a partial resection of the ileumto cease the bleeding. Meckel’s diverticulum and the tumor were resected simultaneously. The pathological diagnosis confirmed adenocarcinoma arising from the Meckel’s diverticulum. The final stage was pT4NxM1; stage Ⅳ according to the Union for International Cancer Control (UICC) classification. After operation we gave the patient first-line; mFOLFOX6 chemotherapy but it turned out to be not effective. Rapid progress of the liver metastases and suspicion of multiple lung metastasis in short time after therapy indicated a bad outcome. We believe this is the first case of adenocarcinoma in a Meckel’s diverticulum to be reported in domestic literature. The diagnosis of Meckel’s tumor should be considered as inpatients’ acute gastrointestinal complaints; when found incidentally at laparotomy it should be carefully examined for any gross abnormality and resection should be considered.
美克尔憩室为成人最常见的消化道畸形, 而该憩室合并癌变则极为罕见。北京大学国际医院胃肠外科近期收治1例消化道出血患者, 经诊治证实为美克尔憩室癌变, 现报告如下。
患者, 女性, 57岁, 2015年11月23日主因“ 间断腹部不适4年余, 加重20天, 黑便2周” 就诊于北京大学国际医院。患者近4年来间断出现进食后腹部胀痛不适, 20 d来症状加重, 伴食欲减退, 餐后有剑突下饱胀感; 2周前无明显诱因出现紫黑色成形便, 每日2~3次, 量约50~100 mL/次, 伴乏力、活动后心悸。患者既往体健。查体:神志清, 贫血貌, 体温36.6 ℃, 脉搏78次/min, 呼吸15次/min, 血压118/54 mmHg(1 mmHg=0.133 kPa)。心肺查体未见明显异常, 腹平软, 无压痛、反跳痛或肌紧张, 移动性浊音阴性, 肝浊音界存在, 肠鸣音活跃。实验室检查:白细胞8.04× 109/L, 中性粒细胞百分比81%, 血红蛋白含量56 g/L, 红细胞压积17.6%。便常规显示暗红色稀便, 潜血(+)。门诊以“ 消化道出血, 重度贫血” 收住院。入院后完善相关检查, 肿瘤标志物结果:糖类抗原(carbohydrate antigen, CA)19-9为64.84 U/mL, CA72-4为12.58 U/mL, 癌胚抗原(carcino-embryonic antigen, CEA)为635.7 μ g/L, 均呈不同程度升高。腹部B超显示:肝内见多发混合回声团, 较大者位于左叶, 大小约7.0 cm× 6.3 cm× 6.9 cm, 边界不清, 形态不规则, 超声考虑肝内多发实性占位, 肝弥漫性病变。腹部增强CT显示肝内多发占位(图1A), 考虑肝多发转移瘤; 右下腹回肠近回盲部区域可见不规则团块影(图1B), 大小约3.1 cm× 2.8 cm, 密度不均, 增强后不均匀强化, 周围脂肪间隙模糊, 见多枚结节影, 考虑回肠远端恶性占位性病变伴系膜淋巴结转移可能。入院 2 d 后行纤维结肠镜, 进镜110 cm至回肠末段距回盲部25 cm, 肠腔内可见大量血水及少量血凝块, 全结肠及部分回肠末段未见异常。
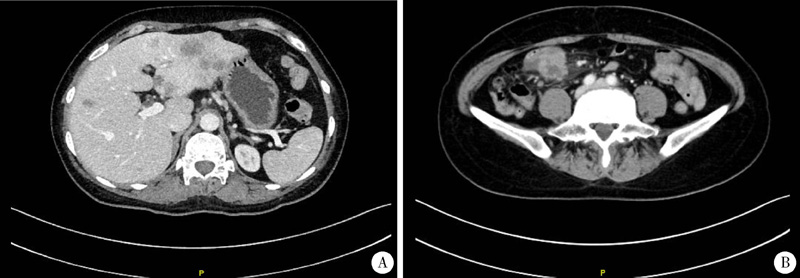 | 图1 增强CT显示肝多发转移(A)和右下腹回肠占位并不均质强化(B)Figure 1 CT showed the multiple liver metastases (A) and the heterogeneous mass of the distalileum (B) |
治疗和随访情况:结合患者病情及相关检查, 考虑患者消化道出血源于回肠, 小肠肿瘤出血合并肝转移可能性大。给予患者多次输注浓缩红细胞纠正贫血, 提高患者手术耐受能力, 但其间患者仍间断大量便血, 贫血纠正效果不明显。入院8 d后患者血红蛋白浓度暂时提升至76 g/L, 为解决出血问题, 为后续治疗创造条件, 遂决定尽快行手术探查。当日于全身麻醉下行腹腔镜探查、小肠肿瘤切除术。术中腹腔内未见明显腹水, 肝两叶多发转移结节, 部分结节融合成团, 以左肝为著, 大网膜、盆腔、腹壁未见种植。右下腹小肠及部分系膜粘连成团, 分离粘连后发现粘连处肠管为美克尔憩室, 憩室距回盲瓣80 cm, 长约6 cm。病变部及以远肠腔内可见血性内容物, 肠周系膜可见肿大淋巴结。切除病变肠管、憩室及相应肠管系膜直至系膜根部, 系膜根部未触及肿大淋巴结, 结合术前多学科会诊意见, 考虑患者肿瘤已存在肝多发转移, 且转移灶肝内分布广泛, 无法实现R0切除, 故放弃同期肝手术, 行断端回肠-回肠侧侧吻合, 吻合满意。探查全部剩余小肠及结肠无异常后关腹。手术用时1.5 h, 出血 50 mL。切除标本剖面可见美克尔憩室盲端一枚菜花样新生物, 直径约2 cm, 质硬伴出血(图2)。术后5 d患者排气, 进流食, 血红蛋白85 g/L。术后2周患者腹壁切口脂肪液化, 给予每日换药处理。术后33日患者收入肿瘤内科, 拟行辅助化疗。术后病理报告:小肠(美克尔憩室)隆起型中-低分化腺癌, 未见明确脉管内癌栓及神经侵犯, 癌肿大小2 cm× 2 cm× 1 cm, 侵及肠壁全层达浆膜外脂肪组织, 癌周肠黏膜慢性炎症; 标本两断端未见癌。肠系膜淋巴结未见癌转移(0/11)。免疫组织化学标记物:CK20(+)、CDX-2(+)、CD34(-)、Ki-67(70%+)、P53(+)、MLH1(+)、MSH2(+)、MSH6(+)、PMS2(+)。术后患者行BRAF、KRAS和NRAS基因检测, 结果显示相应基因均为野生型。转入内科后患者复查肿瘤标志物, CA19-9为110.10 U/mL、CA72-4为39.49 U/mL、CEA> 1 000.00 μ g/L, 较一个月前明显升高。复查腹部增强CT, 肝内转移灶较前增大(图3A); 胸部CT提示右肺多发微结节, 考虑转移(图3B)。患者为Ⅳ 期小肠癌(pT4NxM1), 予mFOLFOX6方案化疗, 患者因经济原因暂放弃西妥昔单抗治疗。
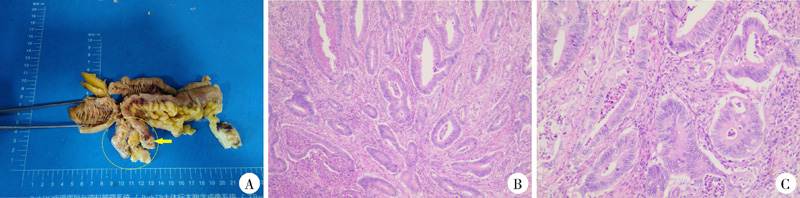 | 图2 回肠部分切除标本(A)及组织病理切片(B, C)Figure 2 Gross resection specimen of ileum (A) and histopathological finding (B, C) |
 | 图3 术后1个月CT复查显示肝转移灶进展(A)和右肺多发微转移(B, 箭头所指处)Figure 3 CT showed the progress of liver metastases (A) and the multiple micro-metastases of lung (B, arrow) 1 month after surgery |
美克尔憩室来源于胚胎发育期的卵黄管, 为成人最常见的先天性消化道畸形, 发病率约为2%[1], 常见于回肠末端, 最常见于距回盲部60~100 cm处, 憩室长度在3~6 cm间。美克尔憩室为真性小肠憩室, 具备小肠肠壁的所有结构, 憩室内可含有异位的黏膜组织, 以胃黏膜组织异位最为多见(发生率为10%~34%)[2], 胰腺组织次之(发生率为5%~16%)[3]。一般而言, 如果憩室狭长, 异位组织常常位于憩室顶端; 如果憩室基底宽广而长度短, 则异位组织可位于近端或憩室内任何部位[4]。目前认为美克尔憩室癌变可能与异位黏膜分泌消化液造成慢性刺激有关。大多数美克尔憩室并无临床症状, 约2%~4%的患者可出现包括憩室出血、肠梗阻、肠套叠、憩室炎、Littre疝、憩室异物、穿孔、癌变等在内的临床并发症[5]。美克尔憩室肿瘤非常罕见, 约占有症状憩室患者的0.5%~1.9%[4], 良性肿瘤与恶性肿瘤均可出现:良性肿瘤可见脂肪瘤、平滑肌瘤等; 恶性肿瘤则包括类癌(77.30%)、腺癌(11.04%)、间叶和平滑肌肿瘤(10.43%)、淋巴瘤(1.23%)等。较之恶性类癌(平均发病年龄61.5岁), 腺癌发病年龄略早(平均55.9岁)[4]。本例患者以消化道出血为突出表现, 出血量大且迁延不止, 患者出现重度贫血, 不易纠正, 强烈具备手术探查指征, 以为后续治疗创造条件[6]。术中发现为美克尔憩室肿瘤, 憩室较长, 肿瘤位于憩室顶端, 符合文献报告规律。本例患者术后病理报告为中-低分化腺癌, 对于美克尔憩室肿瘤而言属于更为少见的病理类型, 国内尚未见类似报告。美克尔憩室恶性肿瘤总中位生存期为173个月:类癌预后较好, 为243个月; 腺癌预后极差, 文献报告中位生存期仅为13个月[4], 化学治疗反应不佳。本例患者术后短期内即可见肝内转移灶进展, 右肺多发微转移灶, 肿瘤标志物水平较术前明显升高, 提示预后极差。有学者曾报告采用卡铂联合培美曲塞的三线方案治疗美克尔憩室腺癌取得了较好效果[2], 但仅限于个案。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|