

{kind=link}
{kind=link}
{kind=link}
乳腺癌保乳术后容积旋转调强和切线野调强放疗的剂量学比较
[孙海涛, 杨瑞杰△  , 江萍, 姜伟娟, 李金娜, 孟娜, 王俊杰]
, 江萍, 姜伟娟, 李金娜, 孟娜, 王俊杰]
, 江萍, 姜伟娟, 李金娜, 孟娜, 王俊杰]
|
|


目的 比较左侧乳腺癌保乳术后容积旋转调强和切线野调强的剂量学差异。方法 选择接受放射治疗的左侧乳腺癌保乳术后患者10例,采用Eclipse计划系统分别设计容积旋转调强(2F-RapidArc)与切线野调强(2F-IMRT)计划,2F-RapidArc采用机架角287°~293°至152°~162°的两个部分弧,中间0°~90°避免照射,2F-IMRT采用机架角301°~311°和125°~135°的切线野照射,处方剂量均为46 Gy/23次,所有计划要求95%靶区体积达到处方剂量。比较2种计划靶区、危及器官剂量分布、机器跳数(MU)和治疗时间。结果 2F-RapidArc和2F-IMRT计划均匀性指数分别是1.12±0.02和1.11±0.03( P=0.282),适形度指数分别是0.80±0.03和0.65±0.04( P<0.001),计划靶区(PTV)V110分别是20.98%±14.47%和10.43%±10.49%( P=0.030)。与2F-IMRT计划相比, 2F-RapidArc计划增加了左侧肺的V5(48.06%±17.32% vs. 24.23%±6.56%, P=0.001)、V10(28.89%±9.28% vs. 17.07%±4.78%, P=0.004)、Dmean[(9.70±2.14) Gy vs. (6.86±1.77) Gy, P=0.002],增加了双肺的V5(22.85%±7.55% vs. 11.01%±2.95%, P=0.001]、V10(13.16%±4.33% vs. 7.76%±2.16%, P=0.006)、Dmean[(4.66±0.95) Gy vs. (3.17±0.82) Gy, P=0.001),但降低了左侧肺的V40(3.58%±1.46% vs. 6.19%±3.04%, P=0.006),同时降低了双肺的V40(1.61%±0.64% vs. 2.81%±1.39%, P=0.005)。增加了心脏的V5(39.3%±17.19% vs. 8.79%±4.24%, P<0.001)、V10(21.31%±13.8% vs. 5.73%±3.42%, P=0.002)、V20(7.80%±6.08% vs. 4.05%±2.85%, P=0.018)、Dmean[(0.64±0.25) Gy vs. (0.29±1.39) Gy, P<0.001],降低了心脏的V40(0.50%±0.40% vs. 1.86%±1.94%, P=0.037)。增加了对侧乳腺的Dmean[(1.63±1.26) Gy vs. (0.09±0.05) Gy, P=0.004]。与2F-IMRT计划相比,2F-RapidArc治疗时间略有增加[(132.9±7.2) s vs. (140.3±11.6) s, P=0.030],两者的机器跳数相当[(467.0±30.4) MU vs. (494.7±44.9) MU, P=0.094]。结论 2F-RapidArc和2F-IMRT计划皆能满足临床需要,2F-RapidArc计划比2F-IMRT计划有更好的适形度,更低的高剂量区,但是增加了患侧肺、双肺、心脏的低剂量区及对侧乳腺的平均剂量;2F-RapidArc计划的治疗时间比2F-IMRT计划略长;2F-RapidArc计划的机器跳数与2F-IMRT计划相当。
Objective: To compare the dosimetric differences between volumetric modulated arc therapy and intensity modulated radiotherapy for breast cancer patients after breast-conserving surgery.Methods: Ten patients who received radiotherapy after breast-conserving surgery were selected. Eclipse planning system was used to design volumetric rotating intensity-modulated (2F-RapidArc) and two field intensity-modulated radiation therapy (2F-IMRT) planning for each patient. 2F-RapidArc plans were made using two partial arcs with gantry rotation from 287°-293° to 152°-162°, and 0° to 90° was avoidance sector. The gantry angle of 2F-IMRT were 301°-311° and 125°-135°. The prescription dose was 46 Gy/23 fractions. All plans required 95% of the target volume receiving the prescription dose. The dose distribution of the target, organs at risk, machine unit (MU) and treatment time were compared.Results: 2F-RapidArc and 2F-IMRT plans’ uniformity index was 1.12±0.02 and 1.11±0.03 ( P=0.282), respectively; conformal index was 0.80±0.03 and 0.65±0.04 ( P<0.001), respectively. V110 of plan target volume was 20.98%±14.47% and 10.43%±10.49% ( P=0.030), respectively. Compared with the 2F-IMRT, 2F-RapidArc plans had a higher dosimetric parameters for left lung: V5(48.06%±17.32% vs. 24.23%±6.56%, P=0.001), V10(28.89±9.28 vs.17.07±4.78 %, P=0.004), Dmean[(9.70±2.14) Gy vs. (6.86±1.77) Gy, P=0.002], increased the double lung: V5(22.85%±7.55% vs. 11.01%±2.95%, P=0.001), V10(13.16%±4.33% vs. 7.76%±2.16%, P=0.006), Dmean[(4.66±0.95) Gy vs. (3.17±0.82) Gy, P=0.001], reduced the left lung: V40(3.58%±1.46% vs. 6.19%±3.04%, P=0.006), reduced the double lung: V40(1.61%±0.64% vs. 2.81%±1.39%, P=0.005), increased cardiac: V5 (39.3%±17.19% vs. 8.79%±4.24%, P<0.001), V10(21.31%±13.8% vs. 5.73%±3.42%, P=0.002), V20(7.80%±6.08% vs. 4.05%±2.85%, P=0.018), Dmean[(0.64±0.25) Gy vs. (0.29±1.39) Gy, P<0.001],reduced the heart: V40(0.50%±0.40% vs. 1.86%±1.94%, P=0.037),increased the contralateral breast Dmean[(1.63±1.26) Gy vs. (0.09±0.05) Gy, P=0.004]. Compared with 2F-IMRTplan, 2F-RapidArc increased the treatment time [(132.9±7.2) s vs. (140.3±11.6) s, P=0.030]. Both the machine units were almost the same [(467.0±30.4) MU vs. (494.7±44.9) MU, P=0.094].Conclusion: Both 2F-RapidArc and 2F-IMRT plans could reach the clinical requirements. 2F-RapidArc had a better conformal index, reduced the high dose area, but increased the low dose regions of the lung, heart, body area, and increased the average dose of the contralateral breast. The treatment time of 2F-RapidArc was longer than that of 2F-IMRT, and the MU of 2F-RapidArc and 2F-IMRT plans were almost the same.
调强放疗(intensity modulation radiated therapy, IMRT)是放疗技术的高级阶段, 是21世纪放射治疗技术发展的方向。有学者报道[1, 2], 乳腺癌采用逆向调强放疗技术代替传统切线野技术, 可以得到更好的靶区剂量分布和降低心脏、肺等重要器官的放射损伤。容积调强放疗(volume modulated arc therapy, VMAT)是IMRT照射方式的突破, 已在复杂靶区乳腺癌照射及鼻咽癌旋转调强放疗中显示了其优势[3]。本研究选用10例左侧乳腺癌患者制定切线野逆向调强放疗计划和容积调强放疗计划, 从靶区剂量分布的适行度和均匀性及心脏、肺、对侧乳腺受照剂量等方面比较两种计划优缺点, 为临床选择治疗方案提供依据。
选择2012年5月至2013年4月左侧乳腺癌保乳术后患者10例, 术后病理分期Ⅰ 期, 病理类型为浸润性导管癌, 需要接受术后放疗。患者年龄 35~50岁, 中位年龄42岁。
患者仰卧于乳腺托架上, 双臂外展上举, 采用Civco公司MT-350乳腺托架固定, 激光灯标记。采用Philips Brilliance大孔径CT, 在患者平静呼吸状态下进行扫描。扫描范围为下颌骨至肝上缘, 层厚为5 mm。扫描后将CT图像经Aria网络系统传输至VARIAN Eclipse 10.0 治疗计划系统。
胸壁靶区勾画标准:参照肿瘤放射治疗协作组织(the radiation therapy oncology group, RTOG)乳腺癌放疗计划图谱(RTOG breast cancer atlas radiation therapy planning: consensus definitions), 内界到胸-肋关节, 外界到背阔肌前缘, 下界到乳腺下缘皮肤皱褶下1.5 cm; 参照正常乳腺, 上界到锁骨头下缘, 前界到皮肤, 后界到肋-胸膜交界, 包括胸壁肌肉和肋骨。实际勾画过程中根据肿瘤分期、部位及手术方式进行相应的调整。
应用VARIAN Eclipse 10.0 计划系统针对每位患者设计IMRT和VMAT治疗计划。采用VARIAN Trilogy直线加速器的6-MV光子线进行设计。处方剂量为46 Gy/23次。IMRT通过调整机架角度, 选择最优化的内切线野入射角度, 使胸壁靶区在射野方向观(beam eye’ s view, BEV)上投射最小, 小机头旋转10° 左右, 外切线野尽量避免与内切野对穿, 根据剂量分布优化靶区及器官剂量, 最后使用Eclipse 10.0功能Skin flash调整叶片位置, 使射野前届在胸壁皮肤表面外露空1 cm。VMAT采用机架角287° ~293° 和152° ~162° 的两个部分弧, 中间0° ~90° 避免照射(图1)。根据剂量分布情况优化靶区和周围危及器官受照剂量。
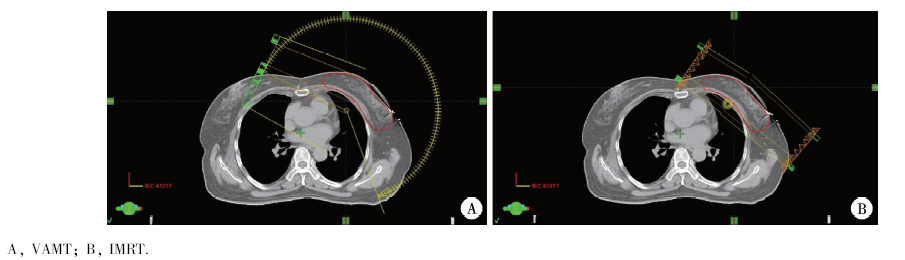 | 图1 两种计划机架角度Figure 1 Two kinds of Plan’ s gantry angle |
使用比利时IBA 公司生产的matrixx检测横断面剂量分布, 使用其自带软件进行γ 检验, 计划输出与实测值在靶区内剂量相差3%, 高梯度区等剂量线位置相差< 3 mm, 在治疗时使用加速器自备装置CBCT与CT计划体位相比较, 确认摆位误差< 3 mm 后方可进行治疗。
比较2种计划的靶区、危及器官剂量分布, 机器跳数(MU)和治疗时间。靶区评价参数为平均剂量Dmean、V105、V110以及靶区均匀指数(homogeneity index, HI)和适形指数(conformal index, CI)。HI的计算公式为:HI=D5%/D95%, 式中D5%和D95%分别为5%和95%计划靶区(planning target volume, PTV)体积所接受到的照射剂量, HI越大, 说明该计划的剂量分布均匀性越差。CI计算公式为CI=VTref/VT× VTref/Vref, 式中VTref为参考等剂量线所覆盖的靶体积, VT为靶体积, Vref为参考等剂量线所覆盖的总体积。CI值的范围是0~1, 值越大适形度越好。危及器官的评价包括患侧肺及全肺平均剂量及V5、V20、V30、V40, 心脏评价平均剂量及V5、V30、V40, 对侧乳腺平均剂量, 全身V5、V20、V30、V40, Vx定义为x%的处方剂量所包绕的靶区体积。
使用SPSS 13.0软件, 计量资料以均数± 标准差表示, 组间比较采用配对t检验, P< 0.05认为差异有统计学意义。
2F-RapidArc和2F-IMRT计划均匀性指数分别是1.12± 0.02和1.11± 0.03(P=0.282), 适形度
指数分别是0.80± 0.03和0.65± 0.04(P< 0.001), 计划靶区V110分别是20.98%± 14.47%和10.43%± 10.49%(P=0.030), 其他参数指标容积调强与切线野调强计划比较差异无统计学意义(表1)。
与2F-IMRT计划相比, 2F-RapidArc计划增加了左侧肺的V5(48.06%± 17.32% vs. 24.23%± 6.56%, P=0.001)、V10(28.89%± 9.28% vs.17.07%± 4.78%, P=0.004)、Dmean[(9.70± 2.14) Gy vs.(6.86± 1.77) Gy, P=0.002], 增加了双肺的V5(22.85%± 7.55% vs. 11.01%± 2.95%, P=0.001)、V10(13.16%± 4.33% vs. 7.76%± 2.16%, P=0.006)、Dmean[(4.66± 0.95) Gy vs.(3.17± 0.82) Gy, P=0.001], 但降低了左侧肺的V40(3.58%± 1.46% vs. 6.19%± 3.04%, P=0.006), 同时降低了双肺的V40(1.61%± 0.64% vs. 2.81%± 1.39%, P=0.005)。增加了心脏的V5(39.3%± 17.19% vs. 8.79%± 4.24%, P< 0.001)、V10(21.31%± 13.80% vs. 5.73%± 3.42%, P=0.002)、V20(7.80%± 6.08% vs. 4.05%± 2.85%, P=0.018)、Dmean[(-0.64± 0.25) Gy vs.(0.29± 1.39) Gy, P< 0.001], 降低了心脏的V40(0.50%± 0.40% vs. 1.86%± 1.94%, P=0.037)。增加了对侧乳腺的Dmean[(1.63± 1.26) Gy vs. (0.09± 0.05) Gy, P=0.004, 表2, 图2~4]。
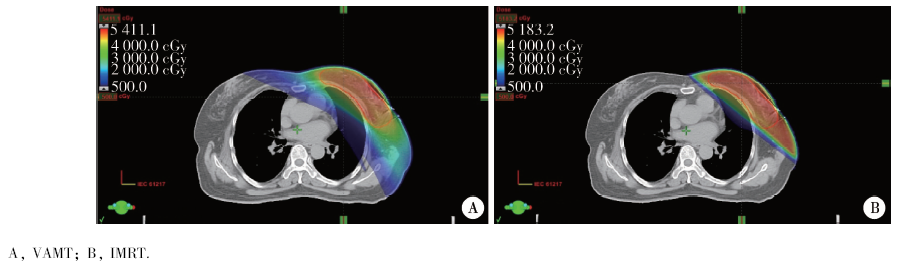 | 图2 两种计划5 Gy覆盖区域Figure 2 Two kinds of plan’ s 5 Gy coverage area |
 | 图3 两种计划10 Gy覆盖区域Figure 3 Two kinds of plan’ s 10 Gy coverage area |
与2F-IMRT计划相比, 2F-RapidArc治疗时间略有增加[(132.9± 7.2) s vs. (140.3± 11.6) s, P=0.030], 两者的机器跳数相当分别是[(467.0± 30.4) MU vs. (494.7± 44.9) MU, P=0.094]。
| 表1 容积调强和切线野调强计划靶区剂量学比较( $\bar{x}$ ± s) Table 1 Comparison of VMAT and IMRT target dosimetric parameters ( $\bar{x}$ ± s) |
放射治疗作为一种局部治疗手段不仅能提高乳腺癌局部控制率, 而且能改善患者远期生存[4]。容积旋转调强作为新的放疗技术, 在头颈部肿瘤已经证实与固定机架角调强相比具有高效、快速等优点[5], 许多研究表明, 乳腺靶区内的剂量不均匀性与乳房组织纤维化有关, 可直接影响到保乳治疗后长期的美容效果[6]。剂量分布不均匀、不良反应严重、设野困难的主要原因是由于同一患者不同层面胸壁的弯曲度及厚度变化相差较大, 造成靶区内剂量不均匀性超过20%[7] , 不同患者胸壁的弯曲度及厚度变化亦有较大差异, 均给放疗设野带来困难。随着患者对美容和生活质量的要求越来越高, 对术后放疗技术提出了相应的更高的要求。
本研究结果显示, 2F-RapidArc技术增加了靶区的适形度, 使等剂量线与靶区贴合更紧密、正常组织的高剂量区更少。
在正常组织保护方面, 应尽可能降低心脏和肺的受照剂量, 从而降低远期心肺损伤的发生率。本研究发现2F-RapidArc计划较2F-IMRT计划降低了心脏的高剂量受照体积, 但增加了心脏的低剂量受照体积和心脏的平均剂量。由于放射导致的冠状动脉缺血性心脏病主要与心脏冠状动脉的损伤相关, 而冠状动脉属于串联器官, 因此高剂量受照体积的减少对心脏的保护具有重要意义[8]。已有研究显示, 可预测肺放射性损伤的指标是Vmean 、V5、V10、V20、V30等一系列剂量体积参数[9]。本研究2F-RapidArc计划较2F-IMRT 计划降低了患侧肺和双肺的V40, 但是显著增加了两者的低剂量区V5、V10、Vmean, 虽然2F-RapidArc计划低剂量区较高, 但是仍然在可接受的范围内, 其临床意义尚需临床实践的进一步证实。国内铁剑等[10]也做过类似的对比研究, 与本研究有相似的结果。
| 表2 容积调强和切线野调强危及器官剂量比较( $\bar{x}$ ± s) Table 2 Comparison of VMAT and IMRT organ at rist dosimetric parameters ( $\bar{x}$ ± s) |
综上所述, 2F-RapidArc计划增加了正常组织的低剂量区范围, 同时减少了心脏和肺的高剂量区照射范围。2F-IMRT计划靶区均匀性、适形度均能满足临床需要, 低剂量区、平均剂量区范围较少, 治疗时间较2F-RapidArc计划更短, 执行更便利。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|