
{kind=link}
{kind=link}
{kind=link}
microCT下钩骨骨内微小动脉三维构筑的临床解剖学研究
[王鼎予1 , 李旭1 , 沈重成1 , 谷培良1 , 裴玉茹2 , 曾钢2 , 冷慧杰3 , 张卫光1, △  ]
]
]
|
|


钩骨钩骨折可见于高尔夫球、网球和棒球运动员, 其原因可能与握拍时的钩骨钩反复受力有关[1, 2]。钩骨钩骨折的并发症较为严重, 可以影响到正中神经和尺神经的感觉运动功能, 而钩骨钩骨折采用保守治疗后骨折不愈的发生率较高[2, 3, 4, 5], 有学者认为骨折造成钩骨的骨内血供破坏是钩骨骨折不愈的主要原因[6]。此前对钩骨内血管解剖学的研究大多采用X线下造影剂灌注等方法, 难以显示骨内微小动脉, 并无法显示钩骨内的血管三维立体分布状况。本研究旨在利用显微计算机断层扫描(micro-computed tomography, microCT)成像, 对钩骨内微小动脉进行扫描和三维重建, 得到高精度的钩骨内动脉的三维构筑模型, 显示钩骨内微小动脉的来源、走行和分布状况, 为临床上钩骨病变的诊治提供解剖学依据。
使用新鲜上肢标本3例, 所有标本均来自无偿遗体捐献者, 年龄45~93岁, 生前同意遗体用于医学教学和科学研究, 均签署遗体捐献同意书, 并经北京市公证部门公证。标本排除上肢外伤、手术、瘫痪、血管疾病和糖尿病等可能影响血管灌注的情况。血管灌注在北京大学解剖模拟手术室进行, microCT扫描成像在北京大学第三医院骨科实验室进行。
在配备有除尘器的实验室内将红色氧化铅颗粒研磨至粒径40 μ m以下, 将氧化铅(Lead mono-xide, Sinopharm Chemical Reagent Beijing Co. Ltd)与松节油(Turpentine oil, Chemical Reagent Beijing Co. Ltd)混合形成均匀的悬浊灌注液, 以不同的红色氧化铅质量与松节油的体积比, 形成1 g :1.5 mL、1 g :1 mL、1 g :0.5 mL共3种灌注液。分离同侧肱动脉, 行肱动脉插管, 依次将45 mL 1 g :1.5 mL、30 mL 1 g :1 mL、15 mL 1 g :0.5 mL的氧化铅松节油悬浊液灌注入肱动脉。整个实验操作全程佩戴防PM2.5口罩。灌注24 h后钩骨取材, 进行microCT扫描。
使用Siemens InveonTM PET/CT扫描钩骨。扫描设置为total rotation [Degrees] 360, rotation steps 360。X线探测仪设置为Transaxial 2048, Axial 2048, 曝光时间为1 500 ms, Binning 1。系统分辨率为high-med。 X线管设置为80 kV, 500 mA。重建设置为Down sample factor 2。图像最终分辨率为27.30 μ m。采用Multimodal 3D Visualization模式生成钩骨二维切片和三维模型。
从掌侧面观察, 钩骨体的3大关节面分别为远端的腕掌关节面、近端的钩三角关节面和桡侧的钩头关节面。钩骨钩近似于椭圆柱型, 桡侧和尺侧的面比较大。桡侧下接钩骨体掌侧平台, 即钩骨钩基底部。
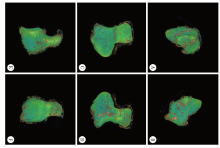
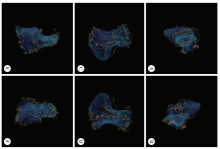
经钩骨microCT三维重建显示:钩骨的非关节面表面主要有4大血管分布区域, 分别位于钩骨体掌侧平台、钩骨背侧、钩骨尺侧和钩骨钩顶端。钩骨表面存在大量的滋养孔, 钩骨周围存在丰富的动脉网, 吻合支多见, 这些钩骨外的动脉网主要分布于骨间韧带内, 关节面处没有动脉进入骨内(图1、2)。
 | 图1 钩骨三维模型显示了钩骨外血管的分布情况, 钩骨体掌侧平台、钩骨背侧、钩骨尺侧和钩骨钩顶端有密集的血管骨外血管Figure 1 The 3D model of the hamate showed the distribution of extraosseous vascularity. There was abundant vessels on the volar side, dorsal side, ulnar side and tip of the hamate hook A, volar; B, dorsal; C, radial; D, ulnar; E, proximal; F, distal; image settings, C 6 W 1 471; color scheme, hue ramp. |
 | 图2 钩骨的三维模型显示了钩骨周围四个供血区域的骨内血管延伸方向和分布区域Figure 2 The 3D model showed the intraosseous vascular distributions in the hamate A, volar; B, dorsal; C, radial; D, ulnar; E, proximal; F, distal; image settings, C 1 582 W 4 624; color scheme: hue ramp. |
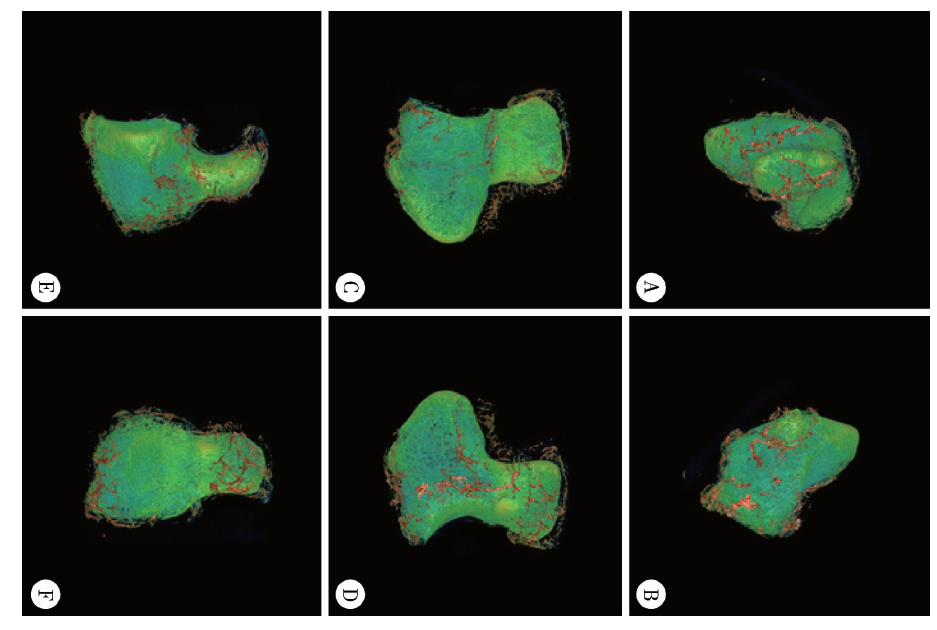
钩骨尺侧骨外的动脉主干呈T形走行(图1D), 位于钩三角关节面和腕掌关节面之间的韧带附着点、钩三角关节和掌侧平台基底之间的韧带附着点以及钩骨钩尺侧。该区域的动脉从钩骨尺侧进入骨内, 发出二级分支到达钩骨头和钩骨体(图3A)。
 | 图3 钩骨尺侧的T形区域骨内血管的分布, 动脉由钩骨尺侧进入, 供应钩骨头和钩骨体(A); 钩骨体掌侧平台血管的骨内分支向掌侧和背侧两个方向延伸, 供应钩骨钩和钩骨体, 同时可见钩骨钩顶端有大量的细小动脉进入(B); 大量粗大的动脉由钩骨背侧进入钩骨内, 同时可见到尺侧T形区的动脉和位于钩骨体掌侧平台的动脉(C)Figure 3 A showed the intraosseous branches from the radial T-shaped vascular zone. The arteries entered from the radial side and perfused the hamate body and the hamulus. B indicated that the intraossous branches of the volar base extended to both hamulus and hamate body. Numbers of small arteries could be observed on the tip of the hamulus. C suggested that some large arteries entered the hamate from the dorsal side. Arteries from ulnar T-shaped zone and volar base were also showed in C Image settings, C 270 W 1 780; color scheme: sky; slice thickness, 1.1 mm. |
钩骨体掌侧平台有大量动脉覆盖, 动脉沿腕掌关节和钩头关节间的韧带附着处向背侧延伸(图1C), 该区域血管的骨内分支向掌侧和背侧两个方向延伸, 到达钩骨钩和钩骨体, 在骨内与钩骨钩顶端和背侧的微动脉相吻合(图3B)。
钩骨钩的顶端有动脉网覆盖, 相比于钩骨其他部位血管, 该处动脉的骨内分支血管细而短。钩骨钩顶端的骨内动脉分支向尺侧延伸, 与钩骨尺侧T形区域的骨内动脉相吻合, 而向背侧延伸的骨内分支与来自钩骨体掌侧平台的动脉相吻合(图3B), 在钩骨体和钩骨钩交界区, 骨内动脉的来源和密度均未见明显的缺失(图3C)。
在钩骨背侧可见较粗大的动脉吻合成网, 发出分支进入钩骨体, 并向掌侧延伸, 与来自钩骨掌侧平台的骨内分支相吻合, 来自钩骨背侧的动脉供应了钩骨体的大部分(图3C)。
钩骨位于远端腕骨组的尺侧, 其桡侧与头状骨相邻, 远端与第4、5掌骨相邻, 近端与三角骨和豌豆骨相邻。钩骨由钩骨体和钩骨钩两部分组成, 各自有骨化中心, 在15岁左右骨化完成。钩骨钩从钩骨的掌面突出, 位于豌豆骨的远端。钩骨钩附着屈肌支持带、豆钩韧带、尺侧腕屈肌腱等多个韧带和肌腱[7]。钩骨钩组成了腕管的尺侧边界和尺管(Guyon管)的桡侧边界。
研究采用microCT成像技术成功地获得了钩骨内微小动脉的三维构筑, 相比X线平片成像, microCT血管成像有效避免了骨内大量微小血管的相互叠加。此外, microCT成像的分辨率高, 可达到微米级, 骨内血管分布显示可精确到毛细血管层面, 故对血管分支状况和分布范围的显示更加精准, 对临床诊治更加具有指导性。
Failla[6]研究了钩骨滋养孔的分布情况, 显示100%的样本在桡侧基底面存在滋养孔, 71%的样本有尺侧钩骨钩顶端的滋养孔, 尺侧基底面和桡侧钩骨钩顶端的滋养孔出现概率较小, 分别为23%和12%, 但因条件所限, 所报道的钩骨各个区域的滋养孔均较少。本研究microCT重建的钩骨外血管的结果显示, 钩骨表面主要有4大血管分布区域, 分别位于钩骨体掌侧平台、钩骨背侧、钩骨尺侧和钩骨钩顶端。钩骨的周围存在丰富的动脉网, 吻合支多见。这些钩骨外的动脉网主要分布于骨间韧带内, 骨内血管的进入位点分布在肌腱和韧带的附着处, 关节面处没有动脉进入。本研究与此前的研究结果存在明显的不同, 即钩骨并不是由少数穿经滋养孔的小动脉供血, 在钩骨表面存在大量的滋养孔动脉进入钩骨内, 形成骨内微小动脉网, 而钩骨的血供与周围组织构成一个整体, 钩骨骨内血管来源广泛, 并非此前认为的仅有数支主干动脉。
1955年, Gettve[8]利用X线观察到钩骨的背侧面有4~7支动脉进入, 钩骨钩的尺侧也有小动脉进入, 钩骨钩掌面桡侧存在向背侧和近端延伸的动脉, 同时在此区域存在一些小动脉供应钩骨远端和钩骨钩。Travaglini[9]也观察到钩骨钩桡侧基底处和钩骨钩顶端尺侧有动脉进入。Panagis等[10]通过X线造影观察到钩骨主要血供来源于钩骨钩桡侧基底面的一支大血管, 钩骨的骨内血管主要由桡侧基底部和钩骨钩顶端的两个血管系统吻合形成, 但未见对钩骨骨内血管的精细描述。本研究发现钩骨的骨内血供非常丰富, 钩骨钩和钩骨体的动脉来源至少都存在3个方向, 钩骨背侧的动脉骨内分支供应钩骨体的大部分区域, 进入钩骨体并且向掌侧延伸, 并且与来自钩骨掌侧平台的骨内分支相吻合, 钩骨
的尺侧动脉的骨内分支供应钩骨头和钩骨体, 钩骨体的掌侧平台有大量动脉覆盖, 发出的骨内分支向掌侧和背侧两个方向延伸, 到达钩骨钩和钩骨体, 在骨内与钩骨钩顶端血管与背侧血管相吻合, 而钩骨钩的顶端有动脉网覆盖, 该区域动脉的骨内分支血管细而短, 向尺侧延伸与钩骨尺侧T形区骨内动脉相吻合, 而向背侧与钩骨体掌侧平台的动脉相吻合。
综上所述, 钩骨体和钩骨钩的骨内微小动脉各自存在丰富的吻合并有多个来源, 出现缺血性钩骨坏死的概率较小。钩骨钩的骨折会造成来自于钩骨钩基底面和来自钩骨体的吻合血管的血供中断, 但从血管解剖学角度来看, 其发生缺血坏死的风险仍然较小, 钩骨钩骨折后骨折不愈可能是由于对线不良等其他原因造成的。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|