

{kind=link}
{kind=link}
{kind=link}
{kind=link}
哮喘样表现的支气管腺样囊性癌1例
[路明1 , 王敏1 , 朱翔2, 3, △  , 陈亚红
, 陈亚红1 , 姚婉贞1 ]
, 陈亚红|
|


Here we reported a case of bronchial adenoid cystic carcinoma from Peking University Third Hospital. A 40-year-old female presented with dry cough for 1 year and nocturnal paroxysmal attacks of wheezing for 4 months. She was a non-smoker, and did not have past histories of asthma or allergy. On physical examination, no stridor, wheezing and cyanosis were present and the general appearance was good. The results of the laboratory analysis, including blood eosinophils count, immunoglobulin E level and chest X-ray were normal. Spirometry revealed reversible airflow obstruction, and post-bronchodilator forced expiratory volume in one second (FEV1) showed an increase of 12% and 230 mL from baseline. Bronchial asthma was diagnosed, however, she responded poorly despite the adequate anti-asthma therapy including high dose inhaled corticosteroid plus long-acting beta2-agonist, theophylline and montelukast. Then chest computed tomography (CT) was performed which showed a polypoid mass occupying the lumen of left main bronchus. Then the bronchoscopy revealed a polypoid endo-bronchial mass arising from the left main bronchus, causing subtotal obstruction of the lumen. Biopsy was carried out through the bronchoscopy, the pathological findings showed characteristic cribriform and tubular pattern which was formed by two-layered cells with ductal and myoepithelial phenotypes, which were consistent with adenoid cystic carcinoma. Re-examining the patient, the lung was clear without any wheeze when she was seated. However, inspiratory wheeze was heard in her left upper lung when she was supine, and disappeared after sitting up again. Subsequently the patient underwent a resection surgery. At the operational site, the tumor was seen on the anterolateral wall of the left main bronchus, without submucosally expanding histologically. Therefore, a sleeve resection surgery of the left main bronchus was performed. Following surgery, chest CT scan revealed complete resolution of the tumor. Her symptoms improved significantly, as did her pulmonary function tests, although all the medicines for asthma were stopped. Now, two years after the operation, the patient remained asymptomatic, and spirometry was performed again which showed normal completely. The presenting case report emphasizes the fact that not all wheezes and reversible airflow obstruction are asthma. It is critical to bear in mind that if a “difficult asthma” patient does not respond to appropriate anti-asthma therapy; localized obstructions should be differentiated.
哮喘是呼吸科常见病, 典型表现为慢性咳嗽、喘息, 夜间症状为著, 以及可逆性气流阻塞。腺样囊性癌是一种少见的特殊类型的气道恶性肿瘤, 常见于气管中下段, 临床上以慢性咳嗽、喘鸣、进行性呼吸困难、固定性中心气道狭窄为主要表现[1]。现将北京大学第三医院2015年收治的1例发生于左主支气管, 肺功能表现为可逆性气流阻塞, 被误诊为难治性哮喘的支气管腺样囊性癌报告如下, 并进行临床分析和文献复习。
患者, 女性, 40岁。咳嗽1年余, 伴夜间喘息4个月。既往体健, 否认过敏性鼻炎、荨麻疹等过敏史和家族史。8个月前无明显诱因出现轻微干咳, 给予阿奇霉素抗感染及对症止咳治疗, 咳嗽无明显好转。近4个月来出现夜间平卧后喘息, 自可闻及喘鸣音, 白天无明显喘息发作, 但逐渐出现活动后气短。于北京大学第三医院门诊体格检查未见异常, 查血常规正常, 胸部X线片未见异常。肺功能检查提示阻塞性通气功能障碍, 第1秒用力呼气容积/用力肺活量(forced expiratory volume in one second/forced vital capacity, FEV1/FVC)53%, FEV1占预计值52%, 支气管舒张试验阳性(FEV1增加绝对值为230 mL, 改善率为15%, 图1)。诊断为支气管哮喘, 查血嗜酸粒细胞计数、免疫球蛋白E正常, 吸入和食物过敏原检测均阴性。给予布地奈德/福莫特罗吸入剂2吸, 每日2次, 夜间喘鸣无明显好转; 后联合孟鲁斯特、茶碱缓释胶囊口服, 仍有夜间反复喘鸣和憋醒, 坐起后可减轻。胸部CT显示左主支气管前壁可见一球状软组织影突向管腔(图2), 支气管镜见左主支气管近端息肉状新生物, 致管腔明显狭窄(图3), 黏膜活检病理诊断为腺样囊性癌(图4)。再次体格检查, 患者坐位, 查体双肺呼吸音对称, 未闻及干湿啰音, 让患者平卧后, 于左上肺可闻及吸气相哮鸣音, 坐位后左上肺哮鸣音消失。
 | 图1 肺功能流速容积曲线Figure 1 Flow-volume curve of lung function test Spirometry displays reversible airflow obstruction and flow-volume curve (pre- and post-bronchodilator, black arrow) |
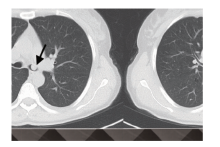
 | 图2 胸部CT表现Figure 2 The image of chest computed tomography st CT scan reveals a polypoid mass occupying the lumen of left main bronchus. |
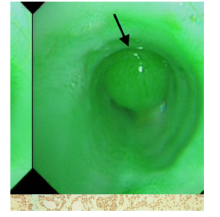
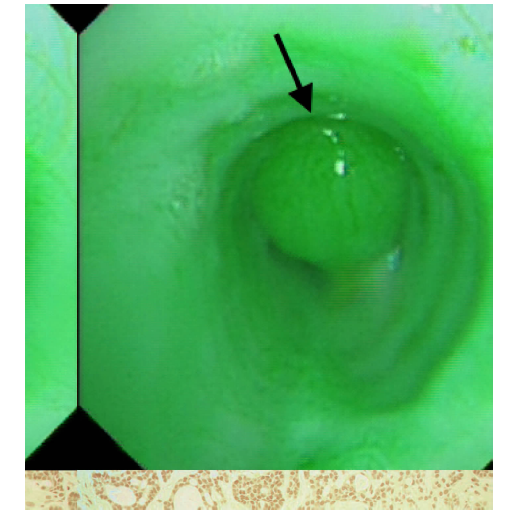 | 图3 支气管镜下表现Figure 3 The manifestation of bronchoscopy Bronchoscopic examination reveals a polypoid intra-luminal mass arising from the left main bronchus, causing almost totally obliteration of the lumen. |
 | 图4 支气管黏膜活检病理Figure 4 The histological characteristics of bronchial mucosal biopsy The tumor showed characteristiccribriform and tubular pattern which formed by two-layered cells with ductal and myoepithelial phenotypes (HE × 200). |
患者于外院行左主支气管袖状切除端端吻合并局部淋巴结清扫术, 后未再发生喘鸣。术后2个月复查肺CT示左主支气管管腔通畅, 新生物消失, 肺功能显示通气功能正常, 支气管激发试验阴性, 呼出气一氧化氮浓度正常。术后2年随访, 患者一切良好, 未再喘息发作, 复查肺功能仍完全正常。
本例患者为中年女性, 慢性病程, 具备哮喘的两个特征性的临床表现, 夜间发作性咳嗽、喘息和可逆性气流受限, 同时, 胸部X线片未见异常, 因此很容易被临床医师诊断为哮喘。但该患者使用了大剂量吸入糖皮质激素/长效β 2受体激动剂、茶碱和孟鲁司特后, 仍难以达到可接受的哮喘控制水平, 这又和临床常见的哮喘特征不符。
按照哮喘的临床思维, 给予上述强有力的抗哮喘治疗后, 症状仍控制不佳者, 应属于“ 难治性哮喘” 范畴。但评价难治性哮喘通常需要遵循以下基本程序[2]:(1)药物治疗是否充分; (2)是否存在未去除的诱发哮喘加重的危险因素, 比如反复过敏原接触等; (3)是否存在相关或使哮喘加重的合并疾病, 比如合并过敏性鼻炎、胃食管反流等; (4)是否存在导致慢性咳嗽、喘息症状的其他疾病, 包括声带功能障碍、中心气道狭窄、支气管肺癌等。该患者前三项均不符合, 后行肺CT发现了左主支气管肿瘤的存在, 最终得以修正诊断, 提示对于临床上的“ 难治性哮喘” , 应按照上述程序逐一评估, 而不是盲目的增加药物, 从而避免漏诊和误诊的发生。
腺样囊性癌又名圆柱瘤, 是一种少见的涎腺源性肿瘤, 在气道肿瘤中占第二位, 仅次于鳞状细胞癌。该肿瘤起源于气道黏膜下腺体, 好发于40~50岁, 男女发病比例相近, 与吸烟无相关性。气管/支气管腺样囊性癌常在黏膜下潜在扩展, 生长相对缓慢, 属低度恶性[1, 3], 因此, 临床上大多数患者起病隐匿, 疾病进程相对缓慢。文献报道, 患者从出现症状到确诊的时间通常较长, 平均需2年左右[4]。早期多无症状, 或仅有刺激性干咳, 当管腔被肿瘤阻塞50%以上时才表现为进行性加重的喘鸣和呼吸困难[4]。应该注意的是, 该病听诊时肺内的哮鸣音多位于胸骨上窝或单侧肺, 且是吸气相的, 而不是哮喘常见的双肺对称性呼气相的哮鸣音。该病的临床症状常与肿瘤的生长部位和患者的体位有关。本病例的肿瘤生长于左主支气管前壁, 因此在平卧位时肿瘤因重力效应会导致气道狭窄加重, 出现“ 夜间发作性喘鸣音” 和左肺吸气相哮鸣音, 在坐位时气道狭窄随之减轻, 从而出现立卧位查体时显著的哮鸣音变化。
腺样囊性癌可发生于从声门会厌至气管、主支气管、叶/段支气管的各级气道, 其中最好发于气管的下1/3段。Zhao等[5]总结发现, 腺样囊性癌发生于气管者占65%, 主支气管占20%, 叶/段支气管占15%。当肿瘤发生于气管时, 肺功能检查的流量-容积曲线会出现中心气道狭窄特征性的呼气、吸气相平台和矩形波, 有助于早期识别[6]。而本病例肿瘤阻塞部位发生于左主支气管, 并没有出现上述特征性表现。与支气管平滑肌痉挛导致的哮喘可逆性气道阻塞不同, 肿瘤压迫和阻塞气道通常引起的是固定性气流阻塞。关于该患者为什么会出现可逆性的气道阻塞, 具体原因并不清楚, 复习文献也未检索到相似病例, 推测患者左主支气管阻塞已很严重, 此时吸入支气管扩张剂后所致的气道扩张效应使得支气管舒张试验的结果更容易判定为阳性。关于本病例是否会存在支气管腺样囊性癌合并哮喘的可能, 经长期随访发现, 肿瘤切除术后患者未再有咳嗽、喘息发作, 且否认所有过敏疾病和家族史, 复查肺功能显示正常, 支气管激发试验阴性, 呼出气一氧化氮浓度正常, 因此, 考虑支气管腺样囊性癌合并哮喘的诊断依据不足。
由于常规胸部X线片很难发现中心气道内肿瘤, 因此胸部CT和支气管镜是早期发现支气管腺样囊性癌的重要检查, 可显示肿瘤突入管腔呈息肉状或结节状, 或肿瘤沿管壁长轴浸润生长, 导致气道管腔狭窄[7]。外科手术切除和术后放疗是气管/支气管腺样囊性癌的主要治疗手段, 近年来随着支气管镜的普及和相关介入技术的发展, 经支气管镜腔内介入治疗, 如激光、微波、高频电刀切割、支架植入等也为腺样囊性癌的治疗提供了新的方法[8]。
总之, 本例患者症状和肺功能的“ 欺骗性” 导致了诊断延误。临床出现喘息症状和可逆性气流阻塞, 并非哮喘所特有, 很多可引起气道狭窄的疾病, 包括支气管肺癌、气管/支气管腺样囊性癌亦可出现相似表现, 临床应加以重视和鉴别。对于“ 难治性哮喘” 患者, 应及早行胸部CT和支气管镜检查以排除气道肿瘤的可能性。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|