

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
光学相干断层扫描技术诊断牙根裂的实验研究
[陈晨1* , 章文欣2 , 戚苈源1 , 高学军1 , 梁宇红1, 3, Δ  ]
]
]
|
|


*现在口腔医学院·口腔医院门诊部
目的:以组织学切盘检查作为金标准,评价光学相干断层扫描技术(optical coherence tomography, OCT)诊断根管预备后牙根裂的准确性。方法:收集20颗完整的离体下颌切牙,使用自凝树脂和藻酸盐印模材料进行包埋,暴露根尖区3 mm,使用旋转镍钛器械预备根管至 #30/0.09,每次更换器械,使用1%(质量分数)的次氯酸钠溶液冲洗根管。应用扫频OCT(swept source OCT,SS-OCT)系统及驱动装置,对牙根根尖部进行360°均匀环扫,对距根尖孔1、2和3 mm处的牙根横断面进行图像重建,由两名观察者诊断扫描图像中的牙根裂。OCT扫描后,对牙根进行组织学观察,在距根尖孔1、2和3 mm处制作横切盘,利用立体显微镜观察并记录牙根不同横截面根裂的发生情况,并作为金标准评价OCT诊断根管预备后牙根裂的准确性。结果:20个离体下颌切牙样本进行根管预备后,组织学检查60个(20牙×3 截面/牙)根尖区牙根截面上,有9颗牙共13个截面存在牙根裂;应用OCT扫描成像,正确诊断了其中12个截面牙根裂,即OCT扫描阳性预测值为1.000;对于组织学切盘检查未发现根裂的47个牙根截面,OCT 无误诊发生,OCT发现根裂的阴性预测值为0.979。OCT诊断牙根裂的准确性为0.983,灵敏度为0.923,特异度为1.000。结论:OCT系统可以准确诊断根管预备后根尖部管壁牙根裂。
Objective:To evaluate the accuracy of optical coherence tomography (OCT) in detecting root cracks after root canal instrumentation using histological gold standard.Methods:Twenty complete extracted human mandibular incisors that were free of caries, calculus, and root treatment were chosen and accessed coronally with a diamond bur, then mounted in resin blocks with alginate impression material using simulated periodontal ligaments, and the apex was exposed 3 mm. The teeth were stored in water at room temperature. Then the teeth were then instrumented to the major apical foramen (AF) at #30/0.09 using ProTaper Universal rotary nickel titanium system(Dentsply Maillefer, Ballaigues, Switzerland), irrigation with 1% sodium hypochlorite (NaOCl) by using a 26-gauge needle followed after each instrument. The apical root was scanned with 360° of rotation by Swept-Source Optical Coherence Tomography (SS-OCT) (wavelength: 1 310 nm, scan rate: 20 kHz, axial resolution: 16 μm) with driving device(stepper motor and lifting platform). The reconstruction images of axial planes 1, 2 and 3 mm from the apex were examined and the root cracks were blindly diagnosed by two observers. The horizontal section was performed at 1, 2 and 3 mm from the apex using low speed disc saw (Leica SP1600, Wetzlar, Germany). The presence of cracks was noted under an optical stereomicroscope (ZOOM-630E) with a cold light source using as gold standard to evaluate the accuracy of OCT in detecting root cracks after root canal instrumentation.Results:After canals instrumentation with ProTaper Universal rotary nickel titanium system to #30/0.09, root cracks were detected in 9 of 20 teeth by histological examination. Crack lines were observed on 13 of 60 horizontal sections and cracks on 12 of the 13 sections were detected by OCT. No cracks were observed in the other 47 of the 60 horizontal sections,none of which was misdiagnosed by OCT. The overall accuracy rate for detection of root cracks with OCT was 0.983, the sensitivity was 0.923, the specificity was 1.000, the positive predictive value (PPV) was 1.000 and the negative predictive value (NPV) was 0.979.Conclusion:OCT may be a promising nondestructive imaging method for diagnosing root canal cracks after canal instrumentation.
根管的充分清创和良好成形, 是根管预备的关键[1], 充分的机械预备, 有利于清除根管内的感染[2, 3, 4], 但研究发现, 使用大锥度旋转镍钛器械进行根管预备后, 在牙根的不同水平可以观察到牙根微裂的产生[5, 6, 7], 而这些微裂损伤最终可能会导致根折裂[8, 9, 10]。近期研究中关于根管预备损伤的研究最常用的手段为组织形态学观察, 即使用显微放大设备如立体显微镜对牙根裂进行观察, 如不破坏实验样本的完整性, 仅可以观察延伸至牙根表面的微裂隙[9, 10, 11]。对根管预备完成后的牙根进行不同水平的切盘检查, 能够观察到牙根内部裂纹, 但是由于切盘检查需要破坏样本, 无法动态观察到机械预备过程中牙根裂的产生和发展[5, 6, 12]。光学相干断层扫描技术(optical coherence tomography, OCT)是一种将光学成像技术与计算机技术相结合的成像手段, 具有非侵入式、高分辨率、零辐射等特点, 在生物医学领域的应用日渐广泛。2008年, Shemesh等[13]首次报道了使用OCT观察人造的牙根裂, 结果显示OCT用于诊断人造根裂, 其灵敏度和特异度达90%以上。那么, 是否可以应用OCT, 在不破坏牙根样本完整性的前提下, 发现根管预备中的管壁微裂, 尚未见报道。结合以上临床需求和研究事实, 本研究旨在评价光学相干断层扫描技术发现根管预备后牙根裂的准确性, 探索其未来在牙科领域的应用前景。
1.1.1 OCT系统主体
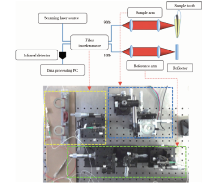
OCT系统由低相干光源和光纤干涉系统、新型光学延时线快速扫描臂装置、样品臂装置、光信号探测及处理系统等部分组成(图1)。探测光为中心频率1 310 nm的中红外光, 扫频激光器中心波长 1 310 nm, 输出波长半高全宽为80 nm, 频率为20 kHz。
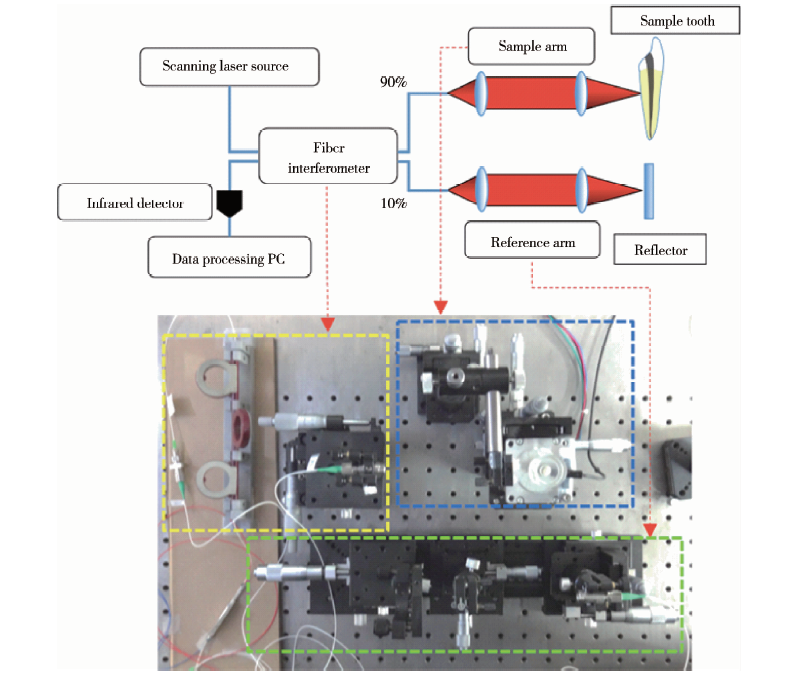 | 图1 扫频OCT系统示意图及装置图Figure 1 Schematic representation of SS-OCT system |
红外波成像源通过光纤干涉系统传输, 经光纤干涉系统分为两束。本实验设定光源进入参考臂和样品臂的比例为1︰9, 以提高信噪比, 优化图像质量。10%的红外光进入参考臂, 由反射镜反射后原路返回, 另一束90%的红外光进入样品臂, 经汇聚透镜聚焦后入射至牙根样本中, 其中一部分入射光发生背向散射并且返回样品臂。参考臂与样品臂中的返回光经由耦合器合成一路并发生干涉, 干涉信号由探测器采集并进入计算机中进行数据处理分析, 通过高精度触发同步实时环形成像程序, 即刻得到扫描样本的图像。
1.1.2 环扫驱动装置
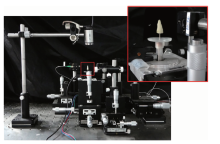
牙根样本倒置, 固定于定轴连接装置(加工定制, 速比科技有限公司, 深圳), 该装置主要由两部分组成:上方的垂直向金属轴插入根管, 沿长轴方向将牙根固定; 下方的水平向帽状玻璃结构用于连接步进电机。
配置动力驱动装置包括步进电机(57BYCH56-401A电机, 宇辉精密电机有限公司, 浙江)和升降平台(GCM-420302M精密平移台, 大恒新纪元科技股份有限公司, 北京, 图2)。通过步进电机带动牙根样本旋转(转速:300 r/min), 对根尖区进行360° 均匀环扫; 利用升降平台, 完成对牙根不同水平的扫描成像。扫描过程中, 于牙根表面均匀涂抹液体丙三醇。
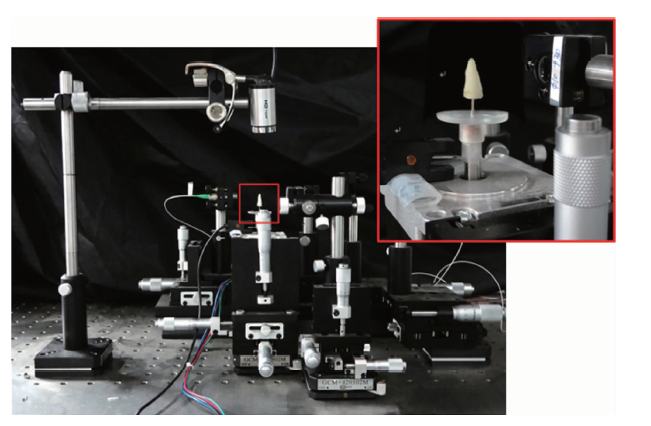 | 图2 扫频OCT系统动力装置Figure 2 Schematic representation of SS-OCT system |
选取牙冠完整、根尖发育成熟、未曾行牙髓治疗的离体下颌切牙(n=20)。立体显微镜(ZOOM-630E, 长方光学仪器有限公司, 上海)下, 观察牙根表面, 排除牙根吸收、根裂的下切牙。拍摄近远中向和颊舌向根尖片, 根据Schneider法[14], 测量根管弯曲度, 选择单根管, 直或轻度弯曲根管(< 10° ), 于釉牙骨质界冠方2 mm处截冠, 使用手用锉通畅根管。用自凝树脂进行包埋, 内衬亲水性藻酸盐印模材料, 以模拟牙槽骨及牙周膜, 暴露根尖区 3 mm的牙根。在实验过程中, 离体牙保存于去离子水中。
离体牙样本(n=20)由一名牙髓专科医生进行根管预备。根管预备流程:不锈钢K锉#10~#15(DW, Munich, Germany)通畅根管, 以根尖孔为止点确定工作长度, 应用16 :1减速马达TCM Endo Ⅲ (Nouvag AG, Goldach, Switzerland), 转速250 r/min, 扭矩2.5 Ncm, 使用ProTaper Universal镍钛系统 (Dentsply Maillefer, Ballaigues, Switzerland)预备根管:Sx锉扩大根管冠方1/3, S1、S2、F1、F2、F3依次进行根管预备, 每根镍钛器械均达到工作长度, 每次更换器械时, 使用2 mL新鲜配制的1%(质量分数)次氯酸钠溶液冲洗根管(图3)。
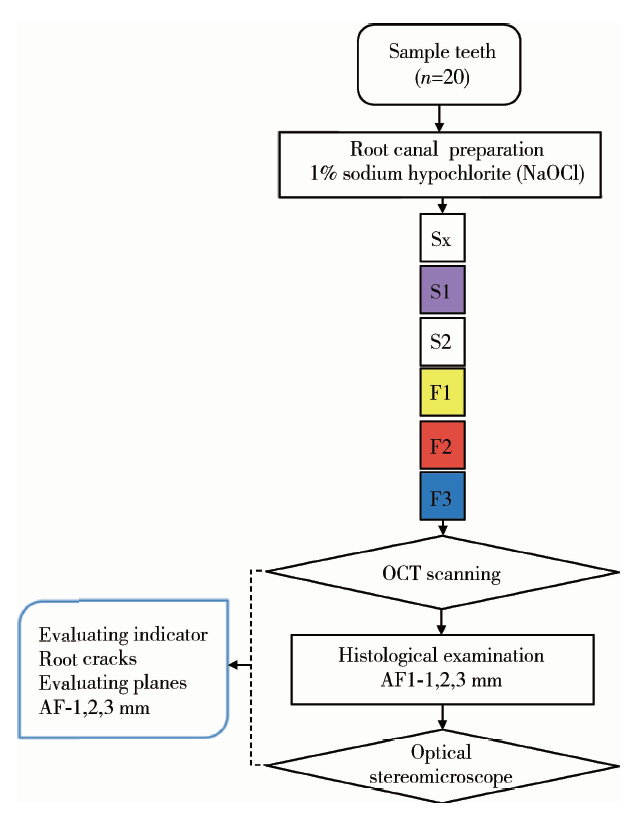 | 图3 实验流程图Figure 3 The flow chart of the experiment |
1.4.1 应用OCT观察根尖区牙根裂
根管预备后, 应用构建的OCT系统, 对根尖区进行外部环扫, 通过高精度触发同步实时环形成像程序进行图像重建, 扫描图像即刻呈现于分辨率为1 024× 1 024的24英寸(1英寸=2.54 cm)BenQ电脑显示屏(BL2410PT, 明基公司, 中国台湾), 调节样本相对于等光程点的位置, 调整图像的亮度, 以获得清晰的图像质量。实验观察评价距根尖孔1、2和3 mm处的牙根截面图像。对两名观察者:一名牙髓专科医师和一名OCT专业技术人员进行培训, 两名观察者盲法、独立观察记录图像中牙根裂的发生情况(以牙根截面为单位), 对判断不一致的图像进行讨论后达成一致, 并将扫描图像保存为psd格式。
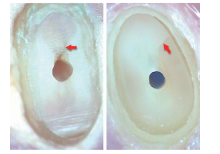
1.4.1.1 根裂判断标准(图4) 当管壁牙本质中出现一条“ 亮线(折射率突变)” (图4A)或两条“ 亮线” 之间存在裂隙(图4B)时, 则记为根裂。
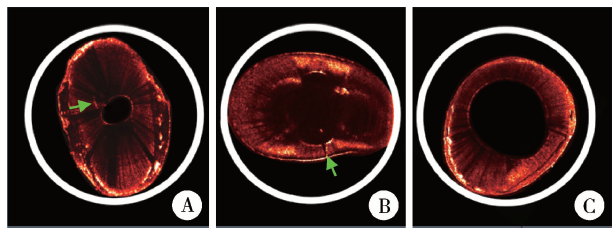 | 图4 OCT扫描图像Figure 4 OCT images of three cross-sections A and B, crack lines were visible (green arrow); C, crack lines cannot be seen. |
1.4.1.2 一致性检验 两名观察者对10个相同牙根截面分别进行观察, 记录牙根裂的发生情况, 一周后再次进行判断, 评价两名观察者的自身一致性和观察者之间的一致性。
1.4.2 应用体视镜观察根尖区牙根裂
1.4.2.1 切盘制作 OCT扫描后, 在距根尖孔1、2和3 mm处分别使用低速盘锯(Leica SP1600, Wetzlar, Germany), 厚度0.300 mm, 转速600 r/min, 水冷却下进行横切盘, 为排除切盘过程本身对牙根的损伤, 对20个未进行根管预备的牙根进行切盘, 作为阴性对照。
1.4.2.2 组织学观察 应用立体显微镜, 使用冷光源, 在25倍放大条件下, 由一名有经验的牙髓专科医师(非OCT扫描图像观察者)观察判断切盘表面是否存在牙根裂, 并统计发生根裂的切盘数。采用二维图像处理系统(Image Measure, CF-2000C, 长方光学仪器有限公司, 上海)拍摄并保存切盘图像(图5)。
 | 图5 使用体视镜观察切盘图像, 红色箭头所示即为根裂Figure 5 Root cross-sections revealed by histology, and crack lines were visible (red arrow) |
应用SPSS 13.0统计软件, 对观察者自身一致性和观察者之间一致性进行检验, 计算Kappa值; 以组织学检查作为金标准, 计算两名观察者应用OCT发现根管预备后根裂的准确性、灵敏度、特异度、阳性预测值和阴性预测值。
应用扫频OCT系统(波长1 310 nm, 频率20 kHz, 理论横向分辨16 μ m), 观察根管预备后根尖区牙根裂的发生情况。两位观察者自身一致性的Kappa值分别为1.000、0.800, 两位观察者之间的Kappa值为0.900。
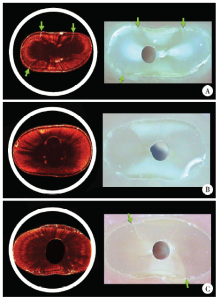
本实验条件下, 作为阴性对照的牙根, 通过切盘组织学检查未发现牙根裂。20个离体下颌切牙样本进行根管预备后, 组织学检查60个(3截面/牙× 20牙)根尖区牙根截面上, 有9颗牙共13个截面存在牙根裂; 应用OCT扫描成像, 正确诊断了其中12个截面牙根裂, 即真阳性; 对于切盘检查未发现根裂的47个牙根截面, OCT无误诊发生(图6)。
 | 图6 相同牙根截面OCT扫描光程图像(左)与组织学切盘图像(右)Figure 6 Three cross-sections revealed by OCT (right) and histology (left) A, crack lines were visible on both images (green arrow); B, crack lines cannot be seen on either image; C, only histology image showed crack lines (green arrow). |
以组织学检查作为金标准, OCT系统诊断根管预备后根尖部牙根裂的准确性为0.983, 灵敏度为0.923, 特异度为1.000, 阳性预测值为1.000, 阴性预测值为0.979(表1、2)。
| 表1 应用OCT诊断根管预备后根尖区牙根裂的准确性评价 Table 1 Diagnostic performance of the SS-OCT of root cracks after root canal preparation |
| 表2 两名观察者应用OCT诊断根裂的结果 Table 2 Positive and negative results of detecting root cracks with OCT by two observers |
OCT是一种将光学成像技术与计算机技术相结合的成像手段, 凭借非侵入式、高分辨、无损伤等诸多特点, 在生物医学领域广泛应用。但在牙科应用的研究报道较少见, 有研究者尝试应用OCT扫描成像手段, 观察牙釉质、牙本质、釉牙骨质界、牙龈、龈沟等软硬组织[15, 16], 检查早期龋坏、釉质脱矿, 观察再矿化动态过程[17, 18]。已有学者报道[19], 应用OCT观察牙髓牙本质的位置与边界, 测量剩余牙本质厚度。
2008年, Shemesh等[13]首次尝试利用OCT观察牙根折裂, 对下颌前磨牙根管垂直加压制造人为根裂, 后使用M2-CV OCT进行内窥扫描观察, 实验结果显示其诊断根裂的灵敏度和特异度达90%以上, 但是通过物理加压手段、利用肉眼观察制造根裂, 裂纹宽度较宽。2013年, Yoshioka等[20]应用扫频OCT诊断离体磨牙“ 天然根裂” , 以microCT的图像结果作为金标准, 发现OCT的准确性为0.89, 但是研究仅对牙根外表面进行平扫观察, 并未形成牙根截面的重建图像, 对于外表面的成像存在一定的形变。
本研究研发构建了一套适用于牙体成像的扫频OCT系统, 获得牙根截面的扫描图像, 观察镍钛器械根管预备后, 下切牙根尖区域牙根裂的发生情况。该OCT系统中心波长为1 310 nm, 频率为20 kHz, 分辨率为16 μ m。本研究对离体牙根尖区域采用外部扫描成像, 然而由于OCT的成像深度所限, 不足以在同一方向上扫描得到整个牙体的横截面图像, 所以, 实验配置升降平台和步进电机等驱动装置带动样品旋转, 以实现对牙根不同水平的360° 均匀环扫, 并于牙根表面均匀涂布液体丙三醇, 以减少表面散射、加深成像深度, 通过高精度触发同步实时环形成像程序, 配合计算机处理输出系统, 获得牙根横截面的图像。
已有研究发现[5, 6, 7], 使用大锥度旋转镍钛器械进行根管预备后, 可能会造成牙根裂的产生, 牙根裂发生率为5%~85%[5, 6, 21, 22, 23]。本研究对20个离体下颌切牙样本进行根管预备, 为排除高浓度次氯酸钠对牙本质性状的影响[24], 选择1%(质量分数)次氯酸钠作为冲洗剂。根管预备完成后(#30/0.09), 组织学检查60个(3截面/牙× 20牙)根尖区牙根截面上, 有9颗牙的13个截面存在牙根裂; 应用OCT扫描成像, 正确诊断了其中12个截面牙根裂, 即真阳性。牙本质中的裂纹会引起折射率突变, 这一光学特性, 在OCT扫描图像上表现为细窄的“ 亮线” , 或当裂纹较宽牙本质有缺隙时, 则表现为在两条“ 亮线” 之间存在裂隙的暗区, 其中一个截面发生漏诊, 该OCT图像上表现为欠连续的分段“ 亮线” , 因此造成了结果的误判, 分析原因可能该牙根截面中的裂纹宽度不均或牙本质一些性状的改变, 从而引起裂纹在OCT图像上的特殊表现。对于切盘检查未发现根裂的47个牙根截面, OCT无误诊发生。与25倍放大条件下的组织学金标准相比, 该扫频OCT诊断根管预备后根裂的准确性为0.983, 灵敏度为0.923, 特异度为1.000。
在本实验条件下, OCT系统可以准确诊断下颌切牙根管预备后根尖部管壁的根裂, 实验结果证实了OCT作为无损的成像技术在根管治疗中的应用前景。然而OCT系统也存在局限性, 就目前的技术水平, OCT对于口腔内硬组织的成像深度约为1.0~1.5 mm, 因此, 本研究仅对离体牙根尖3 mm进行了扫描。受到光纤直径的局限, 本研究为外部扫描, 随着技术的进步, 极细光纤的获得, 把OCT技术应用于内窥扫描, 将在临床应用更有前景。此外, 如果OCT技术的扫描深度能进一步增加, 则具有更重要的意义。
综上所述, 本实验条件下, 扫频OCT能够准确地发现下颌切牙根管预备后根尖区牙根裂的产生。随着系统的日益完善以及光纤探头改造的技术攻关, OCT凭借其安全、无创、零辐射, 以及高分辨率的优势, 期望应用于牙髓研究和临床诊疗。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|