{kind=link}
上颌反复扩缩前方牵引三维变化的锥形束CT分析
[王怡然1, 2 , 周彦恒1 , 王雪东1 , 魏松1 , 刘伟涛1, 3, △  ]
]
]
|
|


目的: 利用锥形束计算机体层摄影术(cone-beam computed tomography, CBCT)探讨扩弓前牵对上颌标志点三维方向变化的影响,为骨性Ⅲ类错牙合畸形的早期治疗提供参考。方法: 选择36例上颌后缩患者,使用随机化区组设计分为反复扩缩组(alternating rapid palatal expansion and constriction group, RPE/C)和对照组(rapid palatal expansion group, RPE), 各18例。RPE/C按照上颌快速扩弓两周、缩弓两周的顺序重复扩缩共10周,最后两周扩弓后行面罩前方牵引,RPE上颌快速扩弓两周后行面罩前方牵引,分别于治疗前(T1)、扩弓后(T2)、前牵后(T3)拍摄CBCT。利用Mimics 10.01软件进行颌面部三维重建、上颌标志点定点和测量分析。结果: RPE/C治疗结束上齿槽座点(subspinale, A)前移(3.06±1.29) mm,RPE(2.16±1.27) mm,组间差异具有统计学意义( P < 0.05);RPE/C治疗各阶段标志点变化更对称;两组患者总治疗时间差异无统计学意义( P > 0.05)。RPE/C上颌骨性标志点矢状向、冠状向和水平向变化趋势:扩弓T2-T1阶段前下、增宽变化,前牵T3-T2阶段前上、缩窄变化,总治疗T3-T1阶段前下、增宽变化,其余测量项目组间差异无统计学意义( P>0.05)。结论: 上颌反复快速扩缩后前方牵引对早期治疗上颌后缩畸形有效;与上颌单次扩弓前方牵引的方法相比,上颌反复扩缩前方牵引对治疗中的上颌骨前移和对称性变化有利;CBCT在正畸测量分析中的应用需要进一步探讨。
Objective: To use the cone-beam computed tomography (CBCT) to evaluate the three-dimensional (3D) changes of maxillary landmarks in the maxillary protraction with alternating rapid palatal expansion and constriction and with rapid palatal expansion, and to provide some clinical suggestions for the early treatment of Class Ⅲ malocclusion.Methods: A total of 36 maxillary retrusive patients were included and randomized in a 1 :1 ratio to either the intervention group (alternating rapid palatal expansion and constriction group, RPE/C) or the control group (rapid palatal expansion group, RPE). Randomization was accomplished with permuted block randomization based on participation sequence. The patients in the RPE/C were treated for 10 weeks (0.5 mm/d ) with the repetition of two-week palatal expansion and two-week palatal constriction. The patients in the RPE were taught to complete rapid palatal expansion for 2 weeks (0.5 mm/d ).The patients were instructed to come to the office for the follow-up to ensure the correct procedures. Damaged expanders were repaired (or replaced) and rebanded quickly. Sequential CBCT images including pretreatment (T1), post-expansion (T2) and post-protraction (T3) were required for 3D reconstruction, establishment of landmarks, measurement and analysis by Mimics 10.01.Results: There was significant forward movement of subspinale (A) in the RPE/C after the treatment with (3.06±1.29) mm, compared with RPE (2.16±1.27) mm, P<0.05. There were more symmetrical changes of the landmarks in the RPE/C and there was no statistic significance of the entire treatment time between the two groups. Moreover, the maxillary skeletal landmarks had the following 3D changes of a forward and downward movement during the expansion stages T2-T1, a forward and upward movement during the protraction stages T3-T2 and a forward and downward movement during the total treatments T3-T1 compared with the control group. And the width between the bilateral landmarks increased during the expansion stages T2-T1, narrowed down during the protraction stages T3-T2 and increased during the total treatments T3-T1.Conclusion: The maxillary protraction with alternating rapid palatal expansion and constriction provided clinical benefits on maxillary advancement and symme-trical changes in the orthopedic treatment of the patients with maxillary retrognathism and it required further study on the orthodontic analysis and measurements of CBCT.
骨性Ⅲ 类错牙合畸形在亚洲人群中患病率高达14%, 其中上颌后缩的表型所占比例较大 [1, 2, 3, 4, 5, 6]。为了尽早减轻骨性Ⅲ 类错牙合畸形对患者容貌、咀嚼、发音及心理健康的不良影响, 同时为了日后代偿性正畸治疗或正畸正颌联合治疗达到更佳矫治效果, 对于生长发育期患者及时进行早期治疗具有一定临床意义[7, 8, 9, 10, 11]。
针对上颌发育不足的青少年患者, 常用的矫形力早期治疗有前方牵引或者扩弓后前方牵引, 大量研究表明治疗有效, 凹面型改善, 反覆牙合、反覆盖解除, 鼻根点至上齿槽座点连线与前颅底平面所成的角(the angle of Nasion-point A plane and SN plane, SNA)、鼻根点至上齿槽座点连线与鼻根点至下齿槽座点连线所成的角(the angle of Nasion-point A plane and Nasion-point B plane, ANB)增大, 上齿槽座点(subspinale, A)作为主要疗效判断指标可矢状向前移约2.0~2.4 mm[12, 13, 14, 15, 16, 17, 18]。2005年, Liou对唇腭裂患者使用上颌双轴扩弓器反复快速扩弓回缩再前牵, 可使A点前移量明显增加[19, 20, 21, 22]。之后部分研究表明A点可前移约2.78~3.04 mm[23, 24, 25, 26, 27, 28]。
影像学方法是一种重要的研究生长发育的方法, 头颅侧位片因拍摄质量、放大率、解剖结构重叠及双侧解剖结构不对称等因素而有诸多局限性, 锥形束计算机体层摄影术(cone-beam computed tomography, CBCT)的应用可在三维方向进行研究分析, 具有信息可靠、图像清晰、射线量相对低等特点[29, 30, 31, 32], 目前CBCT在正畸测量分析的应用还十分局限。
本研究选取符合条件的上颌发育不足青少年患者, 进行随机对照研究, 反复扩缩组(alternating ra-pid palatal expansion and constriction group, RPE/C)为上颌反复快速扩弓回缩再前牵, 对照组(rapid pa-latal expansion group, RPE)为上颌单次快速扩弓再前牵, 通过对CBCT影像进行三维测量, 研究上颌骨三维方向变化, 为今后研究以及临床应用提供参考。
本研究获得北京大学生物医学伦理委员会审查批准(批准号:IRB00001052-10092)。研究选取36例于北京大学口腔医院正畸科2010年8月至2012年11月就诊患者。纳入标准:(1)7~13岁生长发育高峰期前儿童; (2)上颌第一恒磨牙已萌出, 安氏Ⅲ 类错牙合, 前牙反牙合; (3)上颌后缩, 面中部软组织凹陷, 侧貌凹面型; (4)头影测量显示ANB角< 0° , Wits值< -2 mm, A点到鼻根点垂线的距离(the distance from point A to Nasion perpendicular, A-Np)< 0 mm, 下颌可后退至切牙对刃者, 需先对下颌后退位头颅侧位X线片校正后再测量[27, 33, 34]。排除标准:(1)有唇腭裂等其他颌面部畸形或有呼吸系统疾病或其他全身系统性疾病; (2)有正畸治疗史; (3)上颌牙列条件不适合安装扩弓器。
1.2.1 分组方法 使用随机化区组设计进行分组, 患者按就诊顺序编号, 从随机数字表中取随机数字与患者匹配, 以就诊时间相邻的6名患者为一个区组, 区组内患者按随机数字从小到大编号后依次纳入RPE/C和RPE, 每组18例。
1.2.2 治疗方法 扩弓装置均采用带环粘接式Hyrax螺旋扩弓器, 分别粘接于上颌第一恒磨牙和第一或第二乳磨牙或第一前磨牙, 扩弓装置位于腭侧, 牵引钩力臂焊接在后牙带环颊侧, 水平伸出, 于尖牙颊侧前方露出, 由北京大学口腔医院正畸科同一技师制作。RPE/C快速扩弓2周, 0.5 mm/d, 回缩2周, 0.5 mm/d; 重复再扩弓2周, 0.5 mm / d, 回缩2周, 0.5 mm / d; 再重复扩弓2周, 0.5 mm/d, 不回缩。10周后上颌处于扩弓后状态, 锁住扩弓器螺旋。RPE单次快速扩弓2周, 0.5 mm/d, 结束后锁住扩弓器螺旋。两组扩弓结束后立即安装面罩前方牵引装置, 方向向前下方, 与牙合平面呈15° ~30° , 每侧牵引力400~500 g, 医嘱牵引时间至少14 h / d。待前牙反牙合解除, 磨牙关系调整为中性关系或远中关系后结束治疗, 拆除前牵装置及扩弓器。记录治疗前(T1)、扩弓后(T2)及前牵后(T3)时间。
1.2.3 拍摄方法 所有患者分别于T1、T2、T3拍摄头颅CBCT。使用北京大学口腔医院放射科配备的DCTPRO口腔颌面CBCT系统(VATECH公司, 韩国), 扫描参数:90 kV、7 mA, 曝光时间15 s, 体素0.4 mm3, 窗口大小20 cm× 19 cm。拍摄时嘱患者端坐, 目视前方, 使眶耳平面及两瞳孔连线与地面平行, 正中矢状面与机器正中参考面重合, 牙列保持牙尖交错位, 平静呼吸, 勿吞咽。
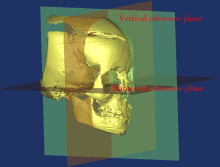
1.2.4 测量方法 将患者CBCT编号后打乱顺序, 将所得CBCT的Dicom格式数据导入Mimics 10.01软件, 三维重建, 生成多个以眶耳平面为水平面、正中矢状面与机器正中参考面重合的互相平行的CBCT影像。本研究设定参考原点为双侧耳点中点, 水平参考平面(horizontal reference plane, HRP)为眶耳平面, 垂直参考平面(vertical reference plane, VRP)为正中矢状面(图1)。确定并测量上颌标志点:右侧眶点(right orbitale, Or-R), 左侧眶点(left orbitale, Or-L), 右侧眶下孔最下点(right infraorbital foramen, InfraO-R), 左侧眶下孔最下点(left infraorbital foramen, InfraO-L), 梨状孔外缘最右点(right point of inner nasal contour, INC-R), 梨状孔外缘最左点(left point of inner nasal contour, INC-L), 右侧上颌第一磨牙腭根根尖点(right maxillary first molar, Mx6-R), 左侧上颌第一磨牙腭根根尖点(left maxillary first molar, Mx6-L)[35, 36, 37, 38]。由本文第一作者定点及测量, 将标志点数值减去对应参考原点数值得到新标志点数值, 再计算变化值比较分析左右对称性、矢状向、冠状向和水平向变化。矢状向变化为垂直于VRP变化, 正值为向前; 冠状向变化为垂直于HRP变化, 正值为向上; 水平向变化为双侧标志点间距变化, 正值为增宽。使用相同的方法由同一名医生对所有CBCT测量两次, 两次间隔一个月。使用组内相关系数(intraclass correlation coefficients, ICC)来评价测量一致性, ICC大于或等于0.75, 计算两次均值作为最终测量值; ICC小于0.75则重新测量。
使用SPSS 17.0软件进行数据统计分析, 数据结果以均数± 标准差表示。对两组患者T1资料进行组间独立样本t检验, 比较两组基线资料的一致性; 对两组患者T1双侧标志点进行组内配对t检验, 比较每组左右对称性; 对两组患者扩弓T2-T1阶段、前牵T3-T2阶段、总治疗T3-T1阶段双侧标志点进行组内配对t检验, 比较左右对称性变化; 对两组患者治疗各阶段测量项目进行组间独立样本t检验, 比较两种治疗方法的差异。检验水准α = 0.05, 双侧检验。
 | 图1 影像测量的水平和垂直参考平面Figure 1 Horizontal and vertical reference planes |
除RPE/C 2例患者失访, 余34例均完成全部治疗。表1可见两组患者男女比例相似, 年龄差异无统计学意义(P > 0.05), RPE/C女性10名, 男性6名, 平均年龄(10.27± 1.56)岁。两组患者前牵时间及治疗总时间组间差异无统计学意义(P > 0.05)。RPE/C前牵时间平均(8.45 ± 2.76)个月, 治疗总时间平均(10.95 ± 2.82)个月。
| 表1 两组患者基本情况和治疗时间比较 Table 1 Comparison of the fundamental condition and the treatment time of two groups |
两组患者T1各测量项目组间差异均无统计学意义(P> 0.05, 表2)。
| 表2 两组患者T1标志点一致性比较 Table 2 Comparison of T1 measurements of two groups |
T1标志点基本对称, 少数标志点个别方向不对称, 差异具有统计学意义, 包括RPE矢状向Mx6和RPE/C冠状向Or; 两组患者均出现明显不对称的结构为矢状向INC 和冠状向InfraO (P< 0.05), 见表3。
| 表3 两组患者T1标志点对称性比较 Table 3 Comparison of T1 symmetry of two groups |
RPE/C标志点治疗各阶段变化均对称(P> 0.05)。RPE标志点T2-T1阶段变化均对称(P> 0.05); T3-T2阶段变化基本对称, 少数点个别方向不对称变化, 差异具有统计学意义, 包括矢状向InfraO、Mx6, 冠状向Or(P< 0.05); T3-T1阶段变化基本对称, 少数点个别方向变化不对称, 差异具有统计学意义, 包括矢状向INC、Mx6(P< 0.05), 见表4。
| 表4 两组患者治疗各阶段标志点变化对称性比较 Table 4 Comparison of symmetry of two groups in different stages |
表5可见矢状向, RPE/C较RPE T3-T1阶段A点前移变化, 差异具有统计学意义, RPE/C(3.06± 1.29) mm, RPE(2.16± 1.27) mm, P< 0.05; 其余标志点治疗各阶段变化组间差异无统计学意义(P > 0.05)。标志点治疗各阶段变化趋势均为向前, RPE/C较RPE T3-T2阶段、T3-T1阶段向前变化大。
| 表5 两组患者治疗各阶段标志点的三维变化 Table 5 Comparison of three-dimensional changes of two groups in different stages |
冠状向, 两组患者多数标志点变化组间差异无统计学意义(P> 0.05), 变化趋势相似, T2-T1阶段向下, T3-T2阶段向上, T3-T1阶段向下或向上; Mx6除外, 治疗各阶段均向下变化, T3-T2、T3- T1阶段组间差异具有统计学意义, RPE/C向下变化显著, P< 0.05。
水平向变化, 两组患者多数标志点变化组间差异无统计学意义(P> 0.05), 变化趋势相似, T2-T1阶段增宽, T3-T2阶段缩窄或略增宽, T3-T1阶段增宽; RPE/C较RPE T2-T1阶段Mx6增宽, 差异具有统计学意义, RPE/C(3.71 ± 2.30) mm, RPE(2.20 ± 1.13) mm, P< 0.05; RPE/C较RPE T3-T2阶段Mx6、INC缩窄, 差异具有统计学意义, P< 0.05。
与传统二维头影测量相比, CBCT具有成像精确的特点, 对于不对称颅面部结构, 图像信息更可靠, 避免了结构重叠、放大率等误差, 同时可利用软件进行三维重建及各类测量, 较以往研究多采用角度等头影测量分析项目更加直观立体[29, 30, 31, 32, 39]。
阈值的界定以及标志点的选择是三维测量的难点, 本研究对于所有患者均选择同一阈值, 尽量选择上颌不同区域骨性标志点, 以保证测量的准确性以及可重复性[39, 40]。
虽然双侧结构标志点变化数值不同, 但既往文献没有比较扩弓前牵各治疗阶段标志点对称性变化及差异是否具有统计学意义, 且CBCT研究多针对扩弓阶段[35, 37]。本研究T1标志点基本对称, 少数标志点个别方向左右不对称, 差异具有统计学意义, 另外, 矢状向INC和冠状向InfraO在两组患者中均出现左右不对称, 差异具有统计学意义, 原因可能为InfraO和INC在骨性Ⅲ 类上颌后缩患者中不对称比例大, 此外, InfraO和INC结构精细, 变异较大, 受放射剂量限制, 影像不够清晰不易定位, 容易造成测量误差。
治疗各阶段各标志点变化基本对称, 变化不对称的不是T1不对称的标志点, 说明治疗前天然的不对称结构不影响变化的对称性。
RPE/C标志点各阶段变化均对称, 而RPE尽管T2-T1阶段均对称, 但T3-T2阶段及T3 -T1阶段有少数点个别方向变化不对称, 差异具有统计学意义。RPE/C较RPE提高了变化的对称性, 原因可能为重力反复快速牵张压缩腭中缝及周围骨缝使其均匀激活, 进而促使双侧变化更加对称。
国内外既往运用CBCT观察扩缩前牵疗效的研究较少, 刘伟涛等[27]将24位患者平分两组, 反复扩缩前牵组治疗后上颌骨前移量[(2.5± 1.0) mm]显著大于对照组[(1.6± 0.8) mm], P< 0.05。本研究采用36位患者的临床随机对照样本, 矢状向观察到相似变化, RPE/C较RPE T3-T1阶段A前移变化差异具有统计学意义, RPE/C(3.06± 1.29) mm, RPE(2.16± 1.27) mm, P< 0.05, 猜测机制为骨缝经过上颌扩缩充分激活, 促使上颌较多地向前变化。
本研究同时还观察到治疗各阶段标志点三维方向变化, 大部分上颌骨性标志点变化趋势为: T2-T1阶段前下、增宽, T3-T2阶段前上、缩窄或略增宽, T3 -T1阶段前下或略向上、增宽, 反映了上颌骨前下、增宽的生长趋势。水平向, RPE/C较RPE T2-T1阶段Mx6增宽变化、T3-T2阶段Mx6和INC缩窄变化差异具有统计学意义, 原因可能为扩缩式扩弓对牙齿及鼻部结构变化影响更大, 此外, RPE/C在T3-T2阶段较多地矢状向向前变化干扰水平向增宽变化。上颌牙性标志点Mx6变化幅度较大且趋势不同于其他标志点, 可能因为扩弓装置带环固定于上颌第一磨牙, Mx6更接近施力核心, 且牙性变化不同于骨性变化, 需要增加更多上颌牙性标志点进行测量分析。
本研究的不足是部分结构精细的上颌骨标志点, 如InfraO和INC, 受放射剂量限制, 颌面部三维重建后影像不够清晰不易定位, 对结果的准确性有一定影响。另外, 虽然本研究要求拍摄CBCT时患者头位保持一致, 并尽量选择骨性标记点, 仍无法保证患者均处于同一状态, 无法完全排除测量的主观因素。
综上所述, 本研究中上颌反复扩缩前方牵引可有效地早期治疗上颌后缩畸形; 与上颌单次快速扩弓前方牵引的方法相比, 上颌反复扩缩前方牵引对治疗中的上颌骨前移和对称性变化有利; CBCT在正畸测量分析中的应用需要进一步探讨。
(本文编辑:刘淑萍)
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|