
{kind=link}
{kind=link}
1例复杂染色体易位伴男性不育患者的家系核型分析及文献复习
[吴桂杰, 马帅, 郑连文, 徐影, 孟繁鹤, 代晓微△  ]
]
]
|
|


SUMMARY One case of family chromosomal karyotype with complex chromosomal translocation and male infertility was reported. This case is a male, 30 years old, Han nationality, who did not receive contraception for 3 years after marriage. The phenotype and intelligence of the patients were normal, and there were no abnormalities in the external genitalia. No abnormalities were found in the prostate and spermatic vein. There was no history of parotitis or testicular trauma, no history of smoking, drinking history, denial of harmful substances and history of radioactive contact. There were no similar patients in the family, and the secondary sex was normal. The routine semen examination suggested that the active sperm was seldom seen. There were no obvious abnormalities in the serum endocrine examination of the patient. Cytogenetic examination: the patient’s karyotype 46XY, t (10; 18; 21) (q22; p11.2; q11.2). There was no deletion in locus sY84, sY86, sY127, sY134, sY143, sY254 and sY255. His wife’s examination showed no obvious abnormality, and her karyotype was normal. The parents of the patients were not close relatives. Their father’s chromosome karyotype analysis was 46, XY, and Y chromosome microdeletion was normal. The chromosome karyotype of the parent was 46XX, t (10; 18; 21), and the parents of the patient also had a daughter, whose phenotype and intellectual development were normal, chromosome karyotype 46XX, t (10; 18; 21). In this case, the patient’s balance translocation should be inherited by the mother. Because of the normal phenotype of the patient, there was no loss of genetic material, but the abnormal chromosomes might be passed to the offspring, and the proportion of the unbalanced gametes was very high. Through systematic review and review of the cases, it was concluded that the balanced translocation carriers only changed the relative position of the translocation segments on the chromosomes, retained the total number of the original genes, only changed the relative position of the genes on the chromosomes, and had no serious effect on the role of the gene and the development of the individual. The phenotype was normal. The patients were given symptomatic treatment to improve semen quality. It is recommended that pre-implantation genetic screening/diagnosis(PGS/PGD) be performed if necessary. It is to guide married men and women to choose the appropriate childbearing age, avoid unhealthy environmental contacts, and strengthen genetic screening before and after pregnancy, so as to achieve the goal of eugenics.
染色体复杂易位是累及3条以上染色体, 有3个以上断裂点的染色体结构异常, 这种异常非常罕见。染色体畸变携带者一般个体表型正常, 但是在减数分裂时发生平衡易位的染色体及其同源染色体发生联会交换, 生成配子时发生遗传物质变化, 这类配子受精后形成的胚胎遗传物质严重不平衡, 往往表现出不育、不孕、流产、死胎或者胎儿畸形等不良后果的发生, 本文就1例复杂染色体易位伴男性不育患者进行病例分析。
患者, 男, 30岁, 汉族, 因婚后未避孕未育3年来吉林大学第二医院生殖中心就诊。患者身高178 cm, 体重74 kg, 表型及智力均正常, 外生殖器无异常, 前列腺及精索静脉超声检查均未见异常; 否认腮腺炎或睾丸外伤史, 无吸烟史、酗酒史, 否认有害物质及放射性接触史, 家族中无类似患者, 第二性征正常。精液常规检查显示精子密度0.1× 106/mL, 前向运动精子率0%、非前向运动精子率0%、不活动精子率100%。患者血清内分泌检查结果如下(括号内为正常参考值):卵泡刺激素 6.98 IU/L(1.50~12.40 IU/L)、促黄体激素 6.31 IU/L(1.70~8.60 IU/L)、睾酮8.99 nmol/L(9.90~27.80 nmol/L)、催乳素334.84 mIU/L(86.0~324.0 mIU/L)、雌二醇17.6 ng/L(25.8~60.7 ng/L)。细胞遗传学检查:在获得患者知情同意后, 抽取其外周静脉血进行淋巴细胞培养, 常规制备染色体, G显带分析计数30个中期分裂相, 镜下分析10个核型, 患者核型为46, XY, t(10; 18; 21)(10pter→ 10q22∷ 18p11.2→ 18qter; 18pter→ 18p11.2∷ 21q11.2→ 21qter; 21pter→ 21q11.2∷ 10q22→ 10qter)(图1)。无精子基因检测 报告示位点sY84、sY86、sY127、sY134、sY143、sY254、sY255未见缺失。其妻各项检查未见明显异常, 染色体核型正常。
 | 图1 患者核型图[46, XY, t (10; 18; 21)]Figure 1 Karyogram of the patient [46, XY, t (10; 18; 21)]Arrowheads show abnormal chromosomes. |
染色体平衡易位是一种常见的染色体结构异常, 一般人群发生率约0.2%[1], 反复流产人群中发生率为5%~10%[2], 其来源可由父或母一方携带而遗传, 也可以在配子形成过程中或受精前受某种因素影响而形成。平衡易位是常见的染色体结构畸变之一, 携带者通常无遗传物质丢失或增加, 故其表型及智力发育均正常。本例患者为3条染色体易位, 经查询Cytogenets Database、Borgaonkar online Database和中国人类染色体异常核型数据库, 截止到2017年12月尚未见相关文献报道。
本例患者的原发不育可能与染色体易位导致的基因断裂或缺失有关, 故建议其接受进一步的遗传学检查。据相关文献报道, 与男性不育相关的染色体异常大多发生在性染色体上, 但近年来不少学者认为常染色体的异常也可以导致精子的发生障碍[3]。男性染色体平衡易位可干扰配子减数分裂, 导致细胞周期阻滞和精子生成障碍, 表现为重度少精症[4, 5], 在生殖细胞的发育过程中, 常染色体的畸变可导致减数分裂阻断或部分阻断, 初级精母细胞第一次减数分裂时同源染色体互换率降低, 中变期不对称的双价体、多价体和单价体增多, 使精子生成阻滞在精母细胞水平而不能继续分化成精子, 影响生精功能。据Moretti等[6]报道, 在染色体平衡易位患者中检测到磷脂酰丝氨酸DNA碎片明显增多, 它是一种细胞凋亡标志物, 使精子细胞凋亡增多。此外, 常染色体上存在与睾丸发育及其功能相关的基因, 某些常染色体易位时染色体断裂造成这些基因的缺失或失活, 也会导致无精、少精。
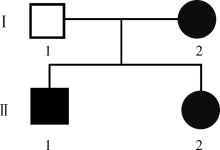
本例患者的父母非近亲结婚, 其父染色体核型为46, XY, Y染色体微缺失检测正常, 其母染色体核型为46, XX, t(10; 18; 21), 父母生育时不存在不良孕产史, 患者的父母另育有1女, 体健, 且其表型及智力发育均正常, 染色体核型与其母亲一致, 家系图谱见图2。
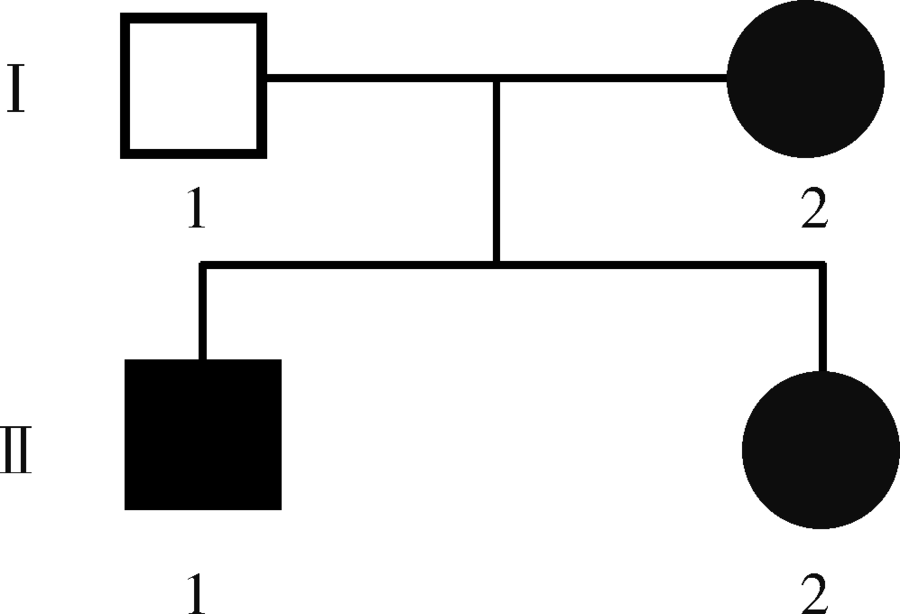 | 图2 患者家系图谱Figure 2 Family map of the patient |
本例患者的染色体平衡易位应是遗传自母亲, 由于母亲表型正常所以判断没有遗传物质丢失, 但可能把异常的染色体传给后代, 形成不平衡配子的比例极高。染色体平衡易位携带者仅改变易位节段在染色体上的相对位置, 保留了原有基因的总数, 只发生了基因在染色体上相对位置的变化, 对基因的作用和个体发育一般无严重影响, 表型正常。染色体平衡易位断裂点处基因结构的破坏导致基因功能的丧失, 染色体断裂后重排改变了基因的位置, 由此所产生的位置效应破坏或改变了基因的表达。染色体平衡易位断裂点处实际上发生了微小基因的缺失或重复, 这些缺失用常规细胞遗传学方法很难与真正的平衡易位区分, 可以通过非放射性荧光原位杂交方法检出[7]。染色体畸变携带者一般个体表型正常, 但是在减数分裂时平衡易位的染色体及其同源染色体联会交换, 生成配子时发生遗传物质变化, 该患者复杂易位所涉及的3条染色体及3个断裂点均未出现在同源染色体间, 因此, 这种突变应该发生在其父母的精子或卵子形成以后且受精以前。对于非同源染色体平衡易位, 理论上相互易位可形成1/18正常配子, 罗氏易位可形成1/6正常配子, 复杂易位获得平衡配子概率更小, 3条染色体的复杂易位在减数分裂过程中至少会形成32种不同类型的配子, 而其中仅有1种正常配子和1种平衡易位的配子, 其余都是单体型或三体型不平衡配子, 这些异常配子容易导致不孕、不育、自然流产、死产、新生儿死亡等情况发生[8]。由于患者拒绝进一步行家系调查, 故仅给予患者对症治疗以改善精液质量, 建议行辅助生殖, 且在必要时行胚胎植入前遗传学诊断和胚胎植入前非整倍体筛查。
平衡易位携带者的变异新核型的来源主要有两种, 一种是由父或母方传递而来, 另一种是配子形成过程中或受精卵分裂时发生。因染色体病多数是遗传而来, 遗传学工作者在遗传咨询中应详细进行家系调查, 如家系中有1例染色体异常, 其他成员也有可能携带有相同染色体异常的情况。此外, 遗传以外的因素, 如电子辐射、环境污染、化学毒物、病原体感染等也应被予以重视。因此, 应指导已婚男女选择合适的生育年龄, 避免不良环境接触, 加强育前、孕前的遗传学筛查, 以真正达到优生优育的目的。
(本文编辑:赵 波)
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|