{kind=link}
{kind=link}
肠代膀胱内原发肠源性腺癌1例
引用本文
覃子健, 毕海, 马潞林, 黄毅, 张帆. 肠代膀胱内原发肠源性腺癌1例. 北京大学学报(医学版), 2018,50(4): 737-739.
QIN Zi-jian, BI Hai, MA Lu-lin, HUANG Yi, ZHANG Fan. A primary intestinal-derived adenocarcinoma in intestine bladder substitutes:a case report. Journal of Peking University(Health Sciences), 2018,50(4): 737-739.
Doi: 10.3969/j.issn.1671-167X.2018.04.029
QIN Zi-jian, BI Hai, MA Lu-lin, HUANG Yi, ZHANG Fan. A primary intestinal-derived adenocarcinoma in intestine bladder substitutes:a case report. Journal of Peking University(Health Sciences), 2018,50(4): 737-739.
Permissions
Copyright©2018, 北京大学
© 2018《北京大学学报(医学版)》编辑部
肠代膀胱内原发肠源性腺癌1例
关键词:
膀胱癌; 肠道; 腺癌
中图分类号:R694
文献标志码:A
文章编号:1671-167X(2018)04-0737-03
A primary intestinal-derived adenocarcinoma in intestine bladder substitutes:a case report
Abstract
SUMMARY Intestinal primary intestine-derived adenocarcinoma of the bladder substituted by the intestine is a very rare long-term complication after complete urethral reconstruction of the bladder. The probability of its occurrence is low. However, in recent years, it has been proved to be objective, but there is rare literature about its diagnosis and treatment methods. This article describes a case of cystectomy and Studer ileal conduit in Peking University Third Hospital due to bladder cancer. After 9 years, he was discovered with a primary intestinal-derived adenocarcinoma in the bladder substitutes by the intestine. A male patient, 64 years old, with persistent abdominal pain in the lower abdomen for two weeks. There was carrion-like material in the urine, no gross hematuria, no urinary frequency, urgency, dysuria, and no abnormalities in the examination. Urinary CT showed intestinal metaplasia in the bladder. There was 5.7 cm×2.4 cm×4.8 cm irregular tissue shadow, and ureteroscopy found, on the right side, the bladder tumor whose diameter was 4-5 cm. We performed open lumpectomy and repaired the bladder, and postoperative pathology showed middle-high differentiated adenocarcinoma. The patient recovered well after the surgery. This article reviewed the similar intestinal primary intestine-derived adenocarcinoma of the bladder substituted by the intestine and found that it had the highest incidence in the elderly male population. The pathogenetic factor was most closely related to the smoking. If the patients developed hematuria, carrion-like substances in the urine, and bladder irritation, the possibility of tumor development should be suspected. Then the patients should promptly take the tests, such as urine exfoliation cytology, urine FISH, urinary system B-ultrasound, cystoscopy, etc. The microscope was the most direct observation of the lesion site examination. If the pathological tumor occurred ,and then the tumor should be immediately removed, and a new urinary diversion was needed to avoid further progress of the tumor. And postoperative smoking was strictly prohibited, also the patients should strictly control their eating habits and regularly adhere to the follow-up at least 4 years or more, but the lifelong follow-up and review was a must. The mechanism of intestinal primary intestine-derived adenocarcinoma of the bladder substituted by the intestine is still unclear. Studies suggest that it may be related to N-nitroso compounds, smoking, and postoperative inflammatory reactions.
Key words:
Bladder neoplasm; Intestine; Adenocarcinoma
膀胱癌是指发生在膀胱黏膜上皮的恶性肿瘤, 是泌尿系统最常见的肿瘤。膀胱癌按浸润深度可分为非肌层浸润性膀胱癌和肌层浸润性膀胱癌, 非肌层浸润性膀胱癌患者多采用经尿道膀胱肿瘤电切术, 术后辅以膀胱内灌注治疗, 预防肿瘤的复发; 肌层浸润性膀胱癌由于浸润深度深, 易发生转移, 故多采用膀胱全切[1]。膀胱全切后肠代膀胱被认为是膀胱全切后下尿路重建的金标准[2], 但是由于肠代膀胱后尿液经由肠管排泄, 肠管不能完全替代膀胱, 可产生电解质紊乱、尿路感染、积水等诸多并发症[3], 其中已经证实肠代膀胱后可能再发生肿瘤, 其发生概率虽低但已成为不争的事实, 本文介绍1例北京大学第三医院Studer肠代膀胱内新发肠源性腺癌的病例。
1 病例资料
患者, 男, 64岁, 因下腹持续性胀痛两周就诊, 尿中有腐肉样物质, 无肉眼血尿, 无尿频、尿急、尿痛等症状, 既往高血压25年, 膀胱切除、Studer回肠原位膀胱术后9年, 糖尿病9年。
体格检查:体温36.6 ℃, 脉搏76次/min, 呼吸20次/min, 血压118/76 mmHg, 腹平坦, 无静脉曲张, 中下腹可见一长约15 cm手术瘢痕, 腹部柔软, 无压痛、反跳痛, 腹部无包块, 肝未触及, 脾未触及, Murphy氏征阴性, 肾无叩痛, 无移动性浊音。肠鸣音正常, 4次/min。
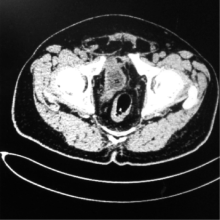
泌尿CT示膀胱未见显示, 回肠代膀胱。双肾盂扩张, 左侧显著, 左右肾盂宽径分别为 4.7 cm和2.0 cm。双肾肾盏内见点状高密度影。双侧输尿管迂曲、扩张。左输尿管中段结石, 代膀胱回肠充盈可, 腔内可见附壁不规则软组织影, 大小约 5.7 cm× 2.4 cm× 4.8 cm(图1)。诊断为“ 膀胱切除、回肠代膀胱术后, 腔内附壁肿物, 性质待定, 左输尿管结石, 双侧肾盂肾盏、输尿管扩张积水, 双肾小结石” 。
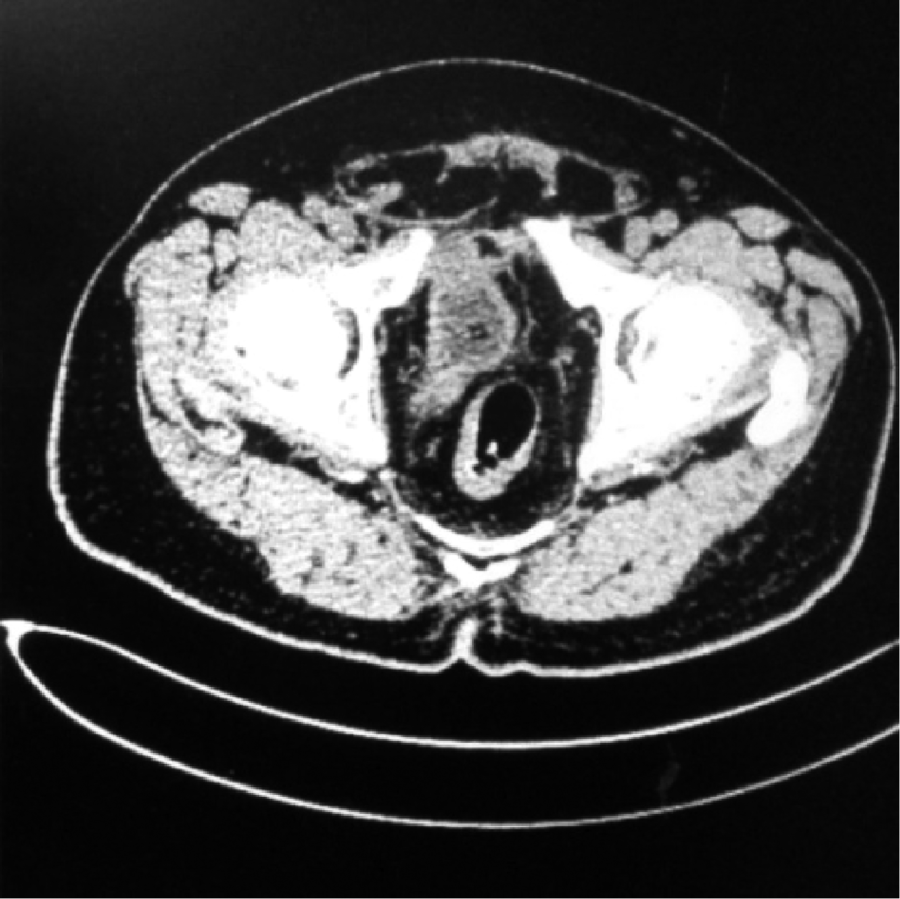 | 图1 肠代膀胱CT扫描结果Figure 1 Computed tomography scans of the bladder substituted by intestinalCT shows that the bladder filling is still acceptable, there is irregular soft tissue attached to the lumen, the size of tissue is about 5.7 cm× 2.4 cm× 4.8 cm. |
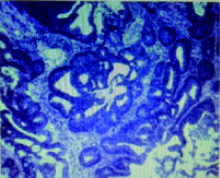
行膀胱镜探查, 观察膀胱黏膜为肠黏膜, 膀胱右侧壁偏输入襻侧似可见肿瘤, 膀胱镜无法接近肿瘤, 换用输尿管镜观察肿瘤, 可见膀胱右侧壁肿瘤, 直径4~5 cm, 呈隆起状生长, 不带蒂, 取活体组织5块进行病理分析, 留置尿管。送检黏膜组织的形态和免疫标记显示为肠源性上皮, 呈高级别上皮内瘤变(图2), 局灶形成黏膜内癌, 由于取材表浅, 无法判断浸润情况。
综上, 诊断为膀胱恶性肿瘤, 行开腹探查、肠粘连松解、新膀胱肿瘤切除术、膀胱修补术。采用腹部右侧旁正中切口, 长约10 cm, 逐层分离进入腹腔, 可见腹腔内明显粘连, 松解肠粘连, 向下腹部游离见新膀胱, 游离膀胱右侧壁, 打开膀胱, 距肿瘤1 cm完整切除, 缝合膀胱伤口并包埋。切下的肿块肉眼见灰褐色, 大小为6.5 cm× 5.0 cm× 3.0 cm, 实性质软糟脆, 切面呈灰白和灰褐色, 解剖结构不清。病理诊断为隆起型中-高分化腺癌, 癌穿过肌层达周围纤维组织, 周围可见正常结肠黏膜, 切缘未见癌。
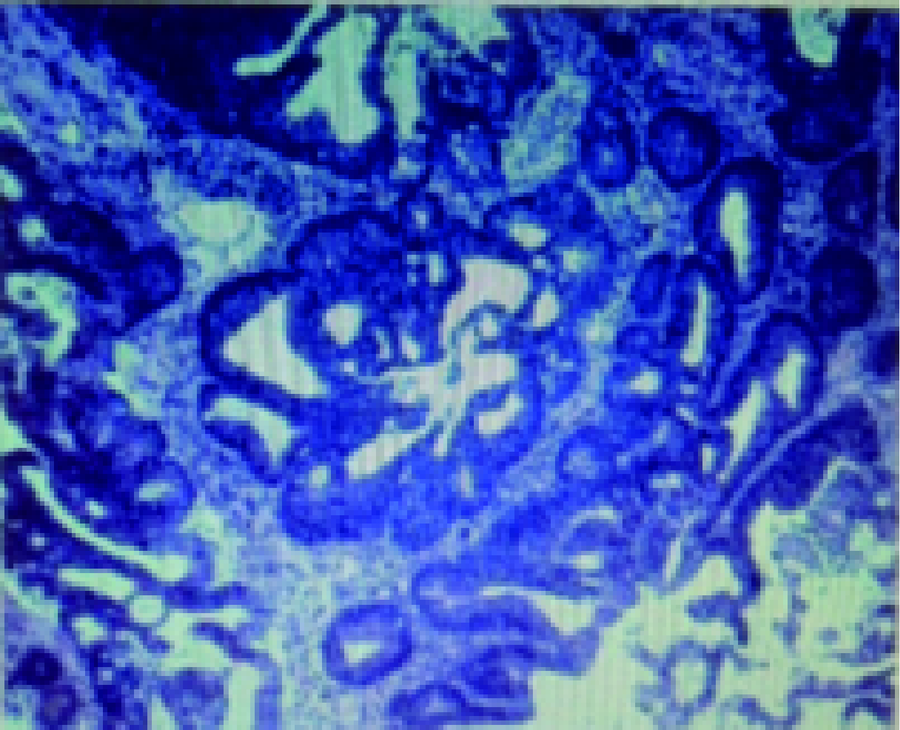 | 图2 肿物组织学特点(HE × 100)Figure 2 Histological feature of the tumor(HE × 100)Mucosal tissue’ s morphology and immunolabeling showed intestinal epithelium with high grade intraepithelial neoplasia. |
术后一年半复查CT, 回肠代膀胱, 内见导管影, 双侧输尿管下段前行与膀胱小肠吻合, 吻合区未见明显异常, 局部肠管、双侧肾盂及输尿管未见明显扩张。患者术后恢复良好。
2 讨论
肠代膀胱内新发腺癌报道较少, 国内外文献均有过报道, 北京大学第三医院多年仅见1例。国内一项266例原位肠代膀胱术患者远期疗效跟踪显示术后4年和术后6年发生肠代膀胱内肿瘤的患者各为1例[4], 国外的相关研究对新膀胱进行了长期的取样随访, 其中在一项对24例接受回肠原位新膀胱术的患者随访5年的研究中, 观察到回肠黏膜变薄, 杯状细胞增多, 绒毛萎缩, 但没有产生肿瘤[5], 另有一项在对30例患者进行的类似的4年随访研究中, 也观察到黏膜变薄和绒毛萎缩, 未观察到细胞发育不良或癌变, 研究人员认为是肠黏膜适应新环境的结果[6]。还有对90例接受原位回肠新膀胱术的患者随访了7年的研究中, 也发现了肠道黏膜发生了类似的渐进性变化[7]。
虽然肠代膀胱后新发肿瘤的发生概率低, 病例数少, 但是通过总结国内外报道的相关病例, 仍可理清此类病例的诊治思路。在发病人群上, 偏向于老年人群, 男性人群居多, 这虽然与膀胱癌发病的流行病学息息相关, 但也是肠代膀胱内肠源性腺癌本身的特点, 在诊治时应首先考虑, 特别是吸烟的人群, 应在既往病史及个人史中详细询问。术后应对随访予以重视, 每3个月复查膀胱镜, 2年后可每半年复查1次膀胱镜, 5年后可每年复查1次膀胱镜, 另还需术后的尿脱落细胞学检查、尿液荧光原位杂交检查、泌尿系统B超检查等, 但是这些检查不能代替膀胱镜检, 膀胱镜检可直接看出术后尿路重建的状况, 出现可疑变化不能确定时, 辅以CT或最可靠方法为组织学活检, 以确定是否是肿瘤及肿瘤的浸润深度。一旦出现血尿、膀胱刺激征时应及时行膀胱镜检查。如若确定新膀胱中出现肿瘤可行手术者应立即行膀胱全切或部分切除, 并行新的尿流改道, 术后应严格进行饮食及吸烟控制, 避免接触过多芳香胺及亚硝胺物质, 并进行规律随访, 患者可以恢复良好。
肠代膀胱后新发肿瘤的机制目前还不明确, 目前有几种可普遍接受的假说。一是N-亚硝基化合物的作用, N-亚硝基化合物是一种强烈的致癌物质, 正常人尿液和粪便中亚硝胺含量极少, 但在输尿管乙状结肠吻合术患者直肠黏液中却发现了较高浓度的亚硝酸盐和亚硝胺, 并证明这些物质与膀胱癌变有关[8]。二是与吸烟相关, 众所周知, 香烟中存在着几十种致癌物质, 其中许多是须在尿液中溶解并经过尿道排泄的, 长期的香烟物质刺激对膀胱癌的产生有一定的作用, 其中以芳香胺的作用最为显著。在膀胱癌膀胱切除术后, 尿液中存在的致癌物质同样对新膀胱有刺激作用, 而且其中的致癌物质浓度与再发肿瘤的风险呈正相关, 仍不能戒烟的患者, 再发肿瘤的概率明显高于戒烟患者[9]。三是炎性反应, 在输尿管乙状结肠吻合模型中发现, 尿流改道术后模型内的生长因子和细胞因子增加, 环氧化酶含量增加, 用于改道的肠道中淋巴细胞及嗜酸性粒细胞增多, 存在着慢性炎症的表现, 由炎性细胞释放的各种炎性因子可以作为致癌物质的启动子[10, 11]。
综上所述, 类似本文肠代膀胱内新发原发性腺癌在膀胱全切后的远期并发症中概率虽低, 但确实客观存在。术后对老年男性患者应予以格外关注, 严禁吸烟, 定期坚持随访至少4年以上, 终身随访与复查是必须的, 一经发现新发腺癌, 应立即行手术治疗, 手术可取得良好疗效, 但是更深入的机制研究和规范的诊疗, 需要进一步的研究与探索。
(本文编辑:刘淑萍)
The authors have declared that no competing interests exist.
参考文献
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|