



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
黄色肉芽肿性肾盂肾炎5例
[崔晨1, * , 蒋洁1, △, *  , 陈文, 崔立刚, 王金锐]
, 陈文, 崔立刚, 王金锐]
, 陈文, 崔立刚, 王金锐]
|
|


SUMMARY Xanthogranulomatous pyelonephritis (XGP) is an unusual form of chronic pyelonephritis in which the renal parenchyma is destroyed and replaced by lipid-laden foamy macrophages. It usually affects middle-aged women with a history of recurrent urinary tract infection, diabetes, or kidney stones. The inflammatory process is usually diffuse and can extend beyond the kidney. The rare focal forms may simulate primary renal tumours. The preoperative imaging diagnosis may be difficult.We reported five cases of XGP, The findings of ours were recorded including kidney size,shape,contour,the echogenecity of the renal parenchyma,the internal echoes of the dilate collecting system,the presence of perinephric fluid accumulation and obstruction.One of the 5 cases was a male patient,and the other four were female,with a mean age of 53 years. He affected kidneys of the 5 cases swelled in different degrees, and one of them was found with line-like anechoic fluid. Among the 5 cases, one kidney appeared as diffusely reducing of the parenchyma echogenicity, multiple hypoechoic areas,disappearance of corticomedullary differentiation and multiple hyperecho with shadow. A round cystic anechoic lesion was found in one kidney,with internal punctate echo and peripheral fluid. Ultrasonographic finding of 1 case was extremely hypoechoic lesion on the left kidney, protruding from the outline of the kidney, with the partial renal capsule discontinuous, the less clear boundary, and a little blood flow in it. Ultrasonographic demonstration of 2 cases was mild dilatation of the collecting system with irregular wall thickening and internal hypoechogenicity,and 1 case was solid lesion with less clear boundary to the pelvic wall and a small amount of blood flow signal, the another 1 case was showed floccule without internal blood flow. Three cases were caused by chronic obstruction verified by operation, of which one was staghorn calculi,one was poorly differentiated squamous cell carcinoma in the middle part of the ureter, and one was inflammatory stricture of upper ureteral. Through analysis of the above five cases and review of related literature, we explored diagnoses and management of the patients with XGP.Xanthogranulomatous pyelonephritis (XGP) is a rare chronic variant of pyelonephritis characterized by destruction of the renal parenchyma. Combining ultrasonographic features of XGP with clinical recurrent urinary infection and chronic obstruction, XGP can be included in the differentiation. The diagnosis of XGP suspected by ultrasound can be clarified by CT, MRI, contrast-enhanced ultrasound.
黄色肉芽肿性肾盂肾炎(xanthogranulomatous pyelonephritis, XGP)是一种少见的由细菌感染引起的肾实质及肾周组织慢性非特异性炎性病变, 约占所有肾感染的0.6%~1.4%, 由于发病率不高, 缺乏特异的影像学表现, 常常被误诊为恶性病变。本文回顾性分析了北京大学第三医院经手术病理诊断证实的5例XGP, 结合文献复习总结其临床表现及声像图特点, 以期提高对该病的声像图认识。
患者男, 69岁, 主因“ 发现血尿一月伴腰部酸痛” 就诊。查体:体温36.5 ℃, 无肾区叩击痛。血常规示:血红蛋白114.6 g/L, 略低于正常值。尿常规示:尿潜血阳性。超声示:右肾形态饱满, 大小约10.6 cm× 5.4 cm, 皮质变薄, 右肾盂及输尿管上段扩张, 内可见低回声填充, 彩色多普勒示低回声内未见明显血流信号(图1), 右肾静脉及下腔静脉未见明显异常回声。超声诊断:右肾盂实性占位— — 恶性可能性大, 建议超声造影。超声造影示:病变在动脉期呈周边结节状增强, 提示肾盂癌。肾动态显像示:右肾血流灌注减低, 肾功能受损。术中可见右肾盂至输尿管连接处膨大, 其内充满黄色、纤维脂肪样肿物, 伴大量灰白色黏稠液体。病理诊断:右肾黄色肉芽肿性肾盂肾炎。
患者女, 78岁, 主因“ 发现左侧腹包块一月余, 近期增大” 就诊。查体:体温36.4 ℃, 左侧腹可触及一大小约5.0 cm× 6.0 cm包块, 质硬, 活动度较大, 伴胀痛, 轻压痛。血常规示:血红蛋白77 g/L, 低于正常水平。尿常规示:尿潜血阳性。超声示:左肾体积偏小, 皮质变薄, 肾内结构尚清晰; 左肾盂扩张, 宽约2.5 cm, 左输尿管上段扩张约1.1 cm, 其下方左侧腹腔内可见一大小约9.1 cm× 7.0 cm× 8.3 cm的低回声包块, 边界清, 内部回声欠均匀, 彩色多普勒示内部血流丰富(图2)。超声诊断:左侧腹实性包块伴左肾积水。肾动态显像示:左肾无功能, 左下腹肿物血流灌注丰富, 提示恶性可能。术后病理诊断:左输尿管中段低分化鳞状细胞癌, 左肾黄色肉芽肿性肾盂肾炎, 伴肾间质及部分肾小球纤维化。
 | 图1 病例1, 右肾形态饱满, 肾盂及输尿管内充满低回声(A), 低回声内未见血流信号(B)Figure 1 Case 1, right kinday enlarge, renal pelvis and ureter full with hypoechoic lesion (A), and the hypoechoic lesion without blood flow signal (B) |
 | 图2 病例2, 右肾盂肾盏扩张(A), 同侧腹部见一低回声包块, 术后证实为输尿管鳞癌(B)Figure 2 Case 2, the right renal pelvis and calyces expansion (A), and the mass confirmed squamous cell carcinoma in the ureter (B) |
患者女, 60岁, 主因“ 发现右肾鹿角形结石” 就诊。查体:体温36 ℃, 右肾区未及明显叩击痛。血常规示:血红蛋白58 g/L, 明显低于正常水平, 尿常规检查未见明显异常。超声示:右肾皮髓质结构消失, 实质内可见多发低回声区, 肾盂内可见多个斑块状强回声伴声影(图3)。超声诊断:右肾结石伴右肾内积脓。肾动态显像提示:右肾未显影, 无功能。经皮肾镜可见右肾盂内多发鹿角形结石及大量白色脓性分泌物。术后病理诊断:右肾黄色肉芽肿性肾盂肾炎伴坏死及钙化。
 | 图3 病例3, 肾内多发结石(A), 肾内可见多发低回声(箭头所示)(B)Figure 3 Case 3, multiple stones in kidney(A), and multiple hypoechoic lesion in kidney(arrow)(B)RK, right kidney; ST, stone. |
患者女, 25岁, 主因“ 间断左下腹痛一月余” 就诊。查体:体温36.3 ℃, 无肾区叩击痛及血尿。血常规示:血红蛋白107 g/L, 略低于正常水平。尿常规未见明显异常。 超声示:左肾上极可见低回声, 大小约3.4 cm× 2.7 cm, 边界欠清, 向肾轮廓外突出, 内见少量血流信号, 局部肾包膜不连续(图4)。超声诊断:左肾实性占位— — 不除外恶性肿瘤。术中可见肾筋膜与脂肪囊分界不清, 粘连严重。术后病理诊断:左肾黄色肉芽肿性肾盂肾炎。
 | 图4 病例4, 肾内见一低回声结节(测量键)(A), 其内未见明显血流信号(B)Figure 4 Case 4, hypoechoic nodules in kidney (measure)(A), without blood flow signal (B) |
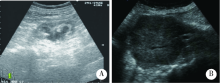
患者女, 31岁, 因右侧腰痛伴肉眼血尿就诊。查体:体温36 ℃, 右侧肾区无叩击痛。尿检结果:外观为暗红色脓液, 镜下所见视野布满红细胞及白细胞。超声示:右肾内可见类圆形无回声区, 大小约 5.4 cm× 5.0 cm, 边界清楚, 内部可见细点状回声, 右肾周线样无回声区(图5)。术中同样发现肾筋膜与肾脂肪囊粘连严重。超声诊断:右肾囊肿伴感染。术后病理诊断:右肾黄色肉芽肿性肾盂肾炎。
 | 图5 病例5, 肾内囊肿无回声, 囊肿内沉积物为细点样回声(A), 肾周可见游离积液(箭头)(B)Figure 5 Case 5, a cystic anechoic lesion in kidney, with internal punctate echo (A) and peripheral fluid (arrow)(B)RK, right kidney. |
XGP是一种少见的特殊类型肾实质及肾周组织慢性非特异性炎症, 由Schlagenhaufe在1916年首次提出, 致病菌多为大肠杆菌及变形杆菌[1], 一般累及单侧肾, 亦有双侧发病者, 双侧XGP 预后较单侧差, 可能和双侧肾功能受损有关[2]。本研究5例患者均为单侧受累。XGP好发于中年女性, 尤其多见于肥胖及患有糖尿病的女性, XGP的临床表现并无特异性, 可表现为腰痛、发热, 其中腰痛为最常见症状, 实验室检查包括:脓尿、贫血、尿路刺激症状及尿路梗阻症状[3], 因其发病诱因多与泌尿系反复感染及泌尿系结石引起的梗阻有关, 这两种人群患有泌尿系统感染及泌尿系结石的风险更大。本组病例也以女性多见。近年来有儿童发病的报道[4], 多见于8岁以下的男孩, 发病原因不同于成年人, 多是因为泌尿系统先天发育异常所致[5]。本组病例中, 有4例表现为不同程度的贫血, 两例尿潜血阳性, 1例表现为脓血尿, 并有1例因输尿管癌导致尿路梗阻。XGP的病理表现为肾实质进行性破坏, 逐渐被黄色肉芽肿结节所替代, 最终导致肾功能受损, 严重者可导致肾衰竭[6]。本组病例中有3例病人术前肾动态显像提示患侧肾功能严重受损, 其病程进展可分为3个阶段[7]:第一阶段仅有肾实质受累; 第二阶段肾实质和肾周脂肪间隙同时受累; 第三阶段病变侵及腹膜后及周围脏器。本组病例中, 有两例患者术中可见肾筋膜与脂肪囊粘连, 1例患者出现肾周积液, 提示病程进展到第二阶段。当病变发展到第三阶段时, 脾、胰腺、十二指肠可出现肉芽肿性病变[8], 严重者可导致肾十二指肠瘘[9]。
Chou等[10]回顾27例经病理证实的黄色肉芽肿性肾盂肾炎的声像图表现, 将其分为4种类型:(1)肾盂积水型(44%):声像图表现为患侧肾体积增大, 伴不同程度的肾盂扩张, 扩张的肾盂肾盏内充满低回声, 此类型患者多伴有输尿管结石、膀胱肿瘤或其他原因引起的尿路梗阻, 本组病例的病例1即表现为扩张的肾盂内充满低回声, 结合病理特点分析扩张肾盂内的低回声实际上为坏死组织碎片及脓液, 超声造影检查表现为扩张肾盂内低回声周边结节状增强, 故而给出肾盂癌的诊断, 其强化区域可能与肾盂壁的局灶性炎性病变有关, 不易与肾盂癌区分。(2)实质弥漫病变型(33%):声像图表现为患侧肾弥漫性增大而无明显肾盂肾盏扩张, 皮髓质分界不清, 实质内见多发低回声区, 此类型患者多伴有鹿角型结石或肾盂输尿管移行处结石, 比对病理特点, 低回声区域内多为坏死的肾组织、炎性细胞和肉芽肿结节, 有文献报道此种类型病变在CT图像上有特征性的表现, 称为“ 熊爪” 征[11], 本组病例的病例3超声诊断提示肾结石合并肾内积脓, 回顾性分析肾声像图, 发现实质回声弥漫性减低, 其内部可见局灶性极低回声, 超声表现符合实质弥漫病变型XGP。(3)肾实质萎缩型(15%):声像图表现为患侧肾体积缩小, 实质回声增强, 皮髓质分界不清, 形成该声像图可能和慢性炎症及肾实质严重受损有关, 发现时多处于病程晚期, 在本组病例2(输尿管中段占位病例)中, 因扩张肾盂内低回声无血流信号显示, 故而只提示肾盂扩张伴沉积物而忽略了肾本身病变。(4)局限型XGP(7%): 较为少见, 声像图表现为肾内局灶性低回声区, 经常伴有结石及局灶性肾周积液, 本组的病例4较符合局限型XGP, 声像图上表现为肾上极不规则低回声区, 向肾轮廓外突起, 局部肾包膜不连续, 边界欠清, 未见血流信号, 值得注意的是局限型XGP可能因为局部炎性刺激, 肾体积可同时增大, 局限型XGP与肾肿瘤在声像图上并不容易区别。
本组病例中除了上述的几种分类情况, 还有1例(病例5)表现为单纯肾囊肿合并感染, 病理提示为黄色肉芽肿性肾盂肾炎, 同时伴有肾周积液。本组病例中没有发现明确的梗阻原因, 结合文献分析可能为肾盏的炎性狭窄[12]。
虽然文献报道及本研究入组病例可以观察到黄色肉芽肿性肾盂肾炎的形态学改变, 然而这些征象缺乏特异性, 因此难以单纯通过超声来明确诊断肉芽肿性肾盂肾炎, 但是, 超声作为泌尿系疾病的首站检查方式, 在遇到相关病例时能够结合超声表现和临床资料考虑到XGP的诊断, 对于疾病的诊断和治疗将有一定的指导意义。
XGP的超声表现不具有特异性, 需要与肾其他疾病相鉴别。弥漫型XGP与肾结核鉴别比较困难, 近年来也有将合并结石的XGP误诊为肾结核的报道[13], 对于肾结核而言, 因其病程进展不同, 所表现出来的声像图也多种多样, 有一部分肾结核晚期可表现为肾体积缩小, 皮髓质分界不清, 形成“ 自截肾” [14], 而XGP的后期病程进展则是向周围组织浸润, 再结合临床表现可以提示为XGP或者肾结核, 但最终确诊还需病理诊断。CT对弥漫型XGP的诊断比较敏感, 除了典型的“ 熊爪印” 征, 还可有以下特点:(1)患侧肾体积增大; (2)肾实质被多个低密度替代, 其增强后出现囊壁环形强化, 这些低密度病灶实际上是被脓液及坏死组织填充的肾盏; (3)肾周筋膜增厚, 肾外组织如脾、胰腺、腰大肌受累, 当出现以上表现时, CT可高度怀疑XGP[15]。
局灶型XGP则需要与肾肿瘤鉴别, 肾肿瘤尤其是透明细胞癌往往边界较清, 同时有因挤压周边肾组织而形成的假包膜[16], 而XGP是炎性反应, 边界较为模糊, 通常没有假包膜形成, 并可能因为炎性刺激而导致肾体积增大, 肾周可出现积液, 同时可合并泌尿系梗阻。超声造影也可以将两者进行区分, 肾肿瘤尤其是透明细胞癌在造影时会在肿瘤与正常肾组织之间有一环形增强带, 呈环状包绕在瘤体周边, 即在灰阶超声观察到“ 假包膜” [17], 而XGP是良性炎性反应, 周边无假包膜形成, 故不出现周边环形强化的特点, 这一点可以帮助两者进行鉴别。
综上所述, 虽然既往观点认为黄色肉芽肿性肾盂肾炎的灰阶声像图表现并无特征性, 有时与肾肿瘤、结核以及其他肾炎症鉴别困难。但本文经病例分析并结合文献阅读发现其临床病史和超声表现具有一定的提示性。当患者出现发热、腰疼、血尿、脓尿、尿路刺激症状以及合并慢性泌尿系梗阻症状时, 结合以下声像图改变, 包括肾形态饱满、肾盂扩张积水, 扩张集合系统内具有低回声, 尤其发现病人有泌尿系梗阻原因及肾结石时, 可以考虑到XGP的可能性。CT和超声造影可能有助于进一步明确疾病的诊断, 最终确诊仍需依靠超声引导下穿刺或手术的病理报告。
(本文编辑:王 蕾)
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|