{kind=link}
{kind=link}
{kind=link}
{kind=link}
颈动脉斑块成分和体积的多排螺旋计算机断层扫描血管成像技术评价
[李金勇1 , 孙宏亮2 , 叶志东1 , 樊雪强1 , 刘鹏1, △  ]
]
]
|
|


目的: 通过多排螺旋计算机断层扫描血管成像技术 (multi-detector computed tomography angiography,MDCTA)评价无症状性与症状性颈动脉狭窄患者斑块的成分和体积的差异。方法: 回顾性分析2011年7月至2015年12月在北京大学中日友好临床医学院连续行血管造影确诊的颈内动脉狭窄≥70%患者的临床资料。症状性患者定义为6个月内出现一过性黑朦、短暂性脑缺血发作及非致残性脑卒中者,否则定义为无症状性患者。共有78例患者符合条件,其中无症状性患者35例(44.9%),症状性患者43例(55.1%)。所有患者造影前一个月内行MDCTA检查。通过MDCTA利用后处理工作站斑块分析软件并根据不同的HU值将颈动脉斑块分为脂质斑块(富含脂质坏死核心,≤60 HU)、纤维斑块(60~130 HU)和钙化斑块(≥130 HU),计算斑块的总体积,各种斑块的体积及所占的比例,并比较两组之间的差异。结果: 无症状性患者的钙化斑块比例明显高于症状性患者( t=2.760, P=0.007),而脂质斑块比例低于症状性患者( Z=-2.009, P=0.044),差异有统计学意义。多因素分析表明钙化斑块比例与无症状性颈动脉狭窄呈正相关( OR=0.949,95% CI:0.915~0.985, P=0.005),脂质斑块比例与无症状性颈动脉狭窄呈负相关( OR=1.068,95% CI:1.021~1.117, P=0.004)。对于症状性患者,当脂质斑块比例大于30.3%时,其特异度为94.3%,而敏感度仅为37.2%。两组斑块体积及纤维斑块比例差异无统计学意义。结论: 与症状性颈动脉狭窄斑块相比,无症状斑块钙化比例增加、脂质比例减少,脂质斑块比例大于30.3%在临床上可以作为预测症状性斑块一个有用的截点,对于颈动脉狭窄患者,可以应用MDCTA斑块分析进行风险评估。
Objective: To evaluate the differences of plaquecomposition and volume between symptomatic and asymptomatic patients with carotid artery stenosis by multi-detector computed tomography angiography (MDCTA).Methods: The consecutive patients with internal carotid artery stenosis≥70% diagnosed by digital subtraction angiography (DSA) were retrospectively analyzed from July 2011 to December 2015 in Peking University China-Japan Friendship School of Clinical Medicine. The symptomatic patients were defined as those who experienced nondisabling ischemic stroke or transient cerebralis chemic symptoms, including hemispheric events oramaurosis fugaxin the last 6 months. Otherwise, the patients were considered as a symptomatic. A total of 78 patients were enrolled in the study. Of these patients, there were 35 asymptomatic patients (44.9%) and 43 symptomatic patients (55.1%). All the patients received MDCTA before DSA. According to the plaque analysis of post processing work station, carotid plaques were divided into lipid-rich necrotic coreplaques (HU≤60), fibrous plaques (60 to 130 HU) and calcified plaques (HU≥130) through the different value sthreshold of HU. The plaque volume and proportion were all calculated. The differences between the two groups were compared by statistical methods.Results: The proportion of calcified plaques in asymptomatic patients was significantly higher than in symptomatic patients ( t=2.760, P=0.007).And the proportion of LRNC plaqueswas lower than that in symptomatic patients ( Z=2.009, P=0.044).There was statistical significance between the asymptomatic and symptomatic patients. Multivariate analysis showed that there was a positive correlation between the proportion of calcified plaques and asymptomatic carotid artery stenosis ( OR=0.949; 95% CI: 0.915 to 0.985; P=0.005). The proportion of LRNC plaques showed a negative correlation with asymptomatic carotid artery stenosis ( OR=1.068; 95% CI: 1.021 to 1.117; P=0.004). For the symptomatic patients, when the LRNC plaque proportion was greater than 30.3%, the specificity was 94.3%, and the sensitivity was 37.2%. There was no significant difference in plaque volume and fibrous plaque proportion in both groups.Conclusion: Compared with symptomatic carotid plaques, the proportion of asymptomatic calcified plaques increased but the proportion of LRNC plaques decreased. Plaque LRNC 30.3% of the total volume may represent a clinically useful cutoff. For the patients with carotid artery stenosis, MDCTA may help noninvasively risk-stratify patients.
在发达国家, 脑卒中是继心脏疾病和癌症之后引起死亡的主要原因。 一项来自美国心脏病协会的数据表明在美国每年卒中的发病为79.5万例, 其中61万例为新发卒中, 18.5万例为复发性卒中。大约20%~25%卒中是由颈动脉狭窄所致[1], 而在所有初次缺血性卒中事件中约有7%与颅外段颈动脉狭窄≥ 60%有关[2]。在北美症状性颈动脉内膜剥脱试验中[3], 75%~94%症状性颈动脉狭窄者的脑卒中风险为27%, 而无症状患者为18.5%, 表明无症状颈动脉狭窄患者的卒中风险低于症状性患者。
颈动脉内膜剥脱和支架置入术是两种治疗颈动脉狭窄有效的手术方式, 适用于狭窄大于50%(血管造影)的症状性患者。经过手术血管重建的症状性颈动脉狭窄患者, 每年卒中的发病率约为1.1%, 相应的5年无卒中生存率为93%[4]。最近, 较大型随机对照研究表明, 在预防卒中事件发生上, 症状性与无症状性颈动脉狭窄患者可以通过颈动脉内膜剥脱和支架置入术获益[5, 6, 7], 然而这些试验是通过颈内动脉狭窄的程度选择患者, 评估卒中风险。此外, 一些因素(如斑块的组织形态)也与卒中风险相关, 因而产生“ 不稳定斑块” 理论, 研究证实不稳定斑块可以作为缺血性卒中事件的一个独立危险因素[8]。
一些非创伤性影像学技术如彩色多普勒超声、多排螺旋计算机断层扫描血管成像(multi-detector computed tomography angiography, MDCTA)、磁共振血管成像可以鉴别不稳定斑块的特性, 其敏感度达83%~100%, 特异度为73%~89%[9], 其中MDCTA是一个可靠的方法, 可以将颈动脉斑块分为钙化、纤维、脂质(富含脂质坏死核心)斑块, 并对斑块体积和成分进行量化, 与组织病理学相比有较好的相关性[10]。研究发现钙化形成并不降低冠状动脉粥样斑块的机械稳定性[11], 而颅外段颈动脉非钙化斑块引起的狭窄与症状相关[12]。Nandalur等[13]通过多层螺旋CT对症状性和无症状性斑块的钙化成分及非钙化成分进行测定, 结果表明颈动脉狭窄患者钙化成分的比例(而非体积)与斑块稳定性相关, 但是该研究并没有对非钙化斑块中的纤维及脂质斑块分别进行评价。本研究旨在通过头颈部MDCTA斑块分析方法评价无症状性与症状性颈动脉狭窄患者斑块的成分和体积的差异。
回顾性分析2011年7月至2015年12月在中日友好医院连续行血管造影的颈动脉狭窄患者的临床资料。
纳入标准:(1)所有患者的颈内动脉起始处狭窄≥ 70%; (2)患者行造影手术前1个月内行头颈部MDCTA检查。
排除标准:(1)非动脉粥样硬化性颈动脉狭窄者, 如大动脉炎等; (2)慢性闭塞性病变或次全闭塞病变者; (3)MDCTA质量欠佳, 无法进行斑块分析者; (4)血管造影提示颅内动脉、椎动脉、对侧颈动脉明显狭窄(≥ 50%)者。
症状性患者定义为6个月内出现一过性黑朦、短暂性脑缺血发作及非致残性脑卒中, 否则定义为无症状患者。共有78例患者符合条件纳入本研究, 其中非症状性患者35例(44.9%), 症状性患者43例(55.1%)。记录患者的基本信息及相关危险因素, 如年龄、体重指数(body mass index , BMI)、性别、高血压、糖尿病、冠状动脉疾病(coronary artery disease, CAD)、高脂血症、既往脑卒中病史、吸烟史等。颈动脉狭窄程度依据《北美症状性颈动脉内膜切除试验标准》并通过全脑动脉造影来确定[14]。
所有患者均行320排头颈部MDCTA检查(Aquilion ONE; Toshiba Medical Systems, Otawara, Japan)。患者肘正中静脉预留20G套管针, 采用高压双筒注射器。增强扫描对比剂使用碘普罗胺佛醇(370 mg iodine/mL Iopromide 370; Bayer Schering Pharma AG, Berlin, Germany), 剂量60 mL, 流速 5.0 mL/s, 并以相同速率注射20 mL生理盐水。扫描参数:准直器宽度80× 0.5 mm; 管电压120 kV, 管电流150 mA, 螺距0.75, 层厚/层间距0.5 mm/0.5 mm。扫描范围为主动脉弓至颅顶, 采用对比剂失踪技术自动触发扫描 (SUREStart, Toshiba), 感兴趣区设在降主动脉, 阈值设定为120 HU。所有扫描图像传输到一个后处理工作站(Vitrea Workstation Vitrea 2, Toshiba Medical), 分别应用多平面重组、曲面重建和容积再现等技术对目标血管进行三维重建, 然后斑块体积和比例用特定的斑块分析软件进行计算。
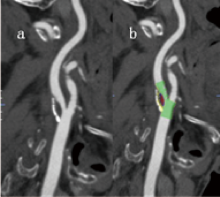
为了确定斑块的体积和比例, 首先通过分析软件自动选择颈内动脉狭窄的斑块范围; 然后在连续叠加的0.5 mm厚的轴位图像中, 相应手动调整颈内动脉斑块的边界以达到最佳范围(图1、图2)。手动调整需要两个经验丰富的影像科主治医师分别确定。斑块的成分通过设置不同的CT值来确定, 根据不同的CT值将斑块分为脂质斑块、纤维斑块、钙化斑块。区分纤维组织和脂质坏死核心的阈值为60 HU, 而区别钙化斑块与纤维组织的阈值为130 HU[10]。斑块的总体积和各成分的体积在感兴趣区内可以根据设定的HU值并通过三维空间容积相关参数由软件自动计算, 而斑块的比例通过各成分占斑块总体积的百分比获得, 选取25例患者进行斑块体积和比例的重复测量, 以检验重测信度。
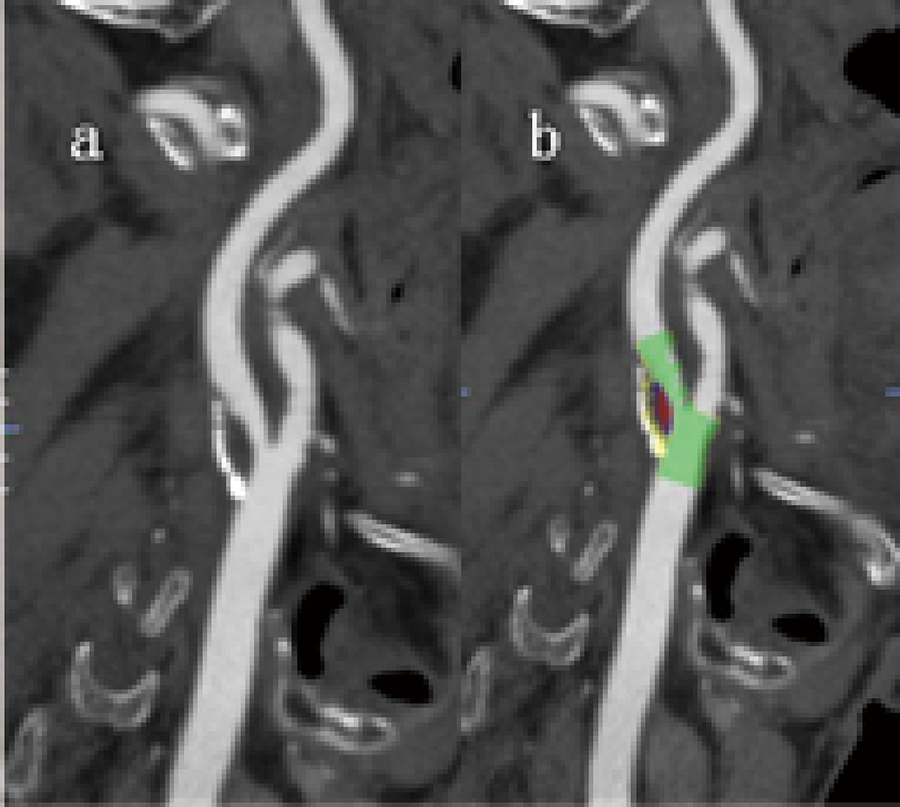 | 图1 MDCTA颈动脉斑块多平面重建矢状位图像Figure 1 Multi-planar reconstruction sagittal images of carotid plaque analyzed by MDCTAa, MDCTA image of carotid plaque lesion was illustrated in the sagittal plane; b, carotid plaque range was selected by MDCTA. The plaque composition is visible in the image, with lipid-rich necrotic core (red), fibrous tissue (blue) and calcification (yellow). |
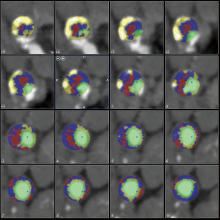
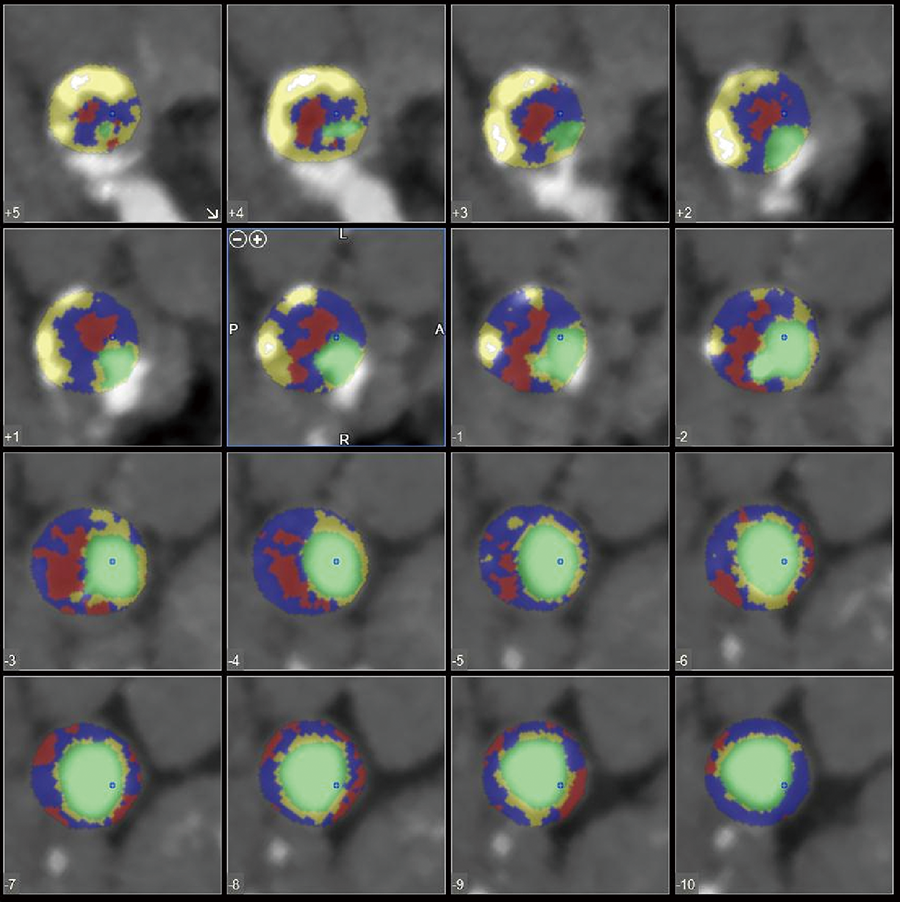 | 图2 MDCTA颈动脉斑块连续轴位分析图像Figure 2 Carotid plaque consecutive axial images analyzed by MDCTAConsecutive plaque images was illustrated by MDCTA in the carotid artery. The plaque composition is visible in the image overlay, with lipid-rich necrotic core (red), fibrous tissue (blue), calcification (yellow), and the contrast-filled lumen (green). |
高血压定义为有高血压病史或连续至少2次测量收缩压大于140 mmHg或舒张压大于90 mmHg。糖尿病定义为重复空腹血糖测量大于126 mg/dL 或者进食后大于200 mg/dL或正在应用降糖药物控制者。高脂血症定义为快速血清检查总胆固醇浓度大于200 mg/dL, 甘油三脂 大于150 mg/dL, 低密度脂蛋白大于140 mg/dL, 高密度脂蛋白小于40 mg/dL, 或正在服用降脂药物者。吸烟史定义为每天吸烟大于1支、至少持续6个月或戒烟少于2年的患者。
应用SPSS 19.0软件进行统计学分析, 计量资料采用均数± 标准差, 采用独立样本t检验或非参数检验进行比较; 计数资料用百分比表示, 组间比较采用卡方检验。分类变量的多因素分析应用二元逻辑回归进行评价, 并建立两个模型。模型Ⅰ 以症状为因变量, 以钙化斑块比例、年龄、高脂血症、吸烟史、糖尿病为自变量; 模型Ⅱ 仍以症状为因变量, 以脂质斑块比例、年龄、高脂血症、吸烟史、糖尿病为自变量, 二者应用向后步进(条件)方法进行回归分析, 结果以斑块比例、年龄、糖尿病、高脂血症表示。钙化或脂质斑块比例的特异度和敏感度通过受试者 工作特征曲线(receiver operating characteristic curve, ROC)计算。斑块体积或比例的重复测量结果应用重测信度检验通过组内相关系数(intra-class correlation coefficient, ICC)进行评价[15]。P< 0.05认为差异有统计学意义。
本研究共纳入了78例患者, 其中非症状性患者35例, 症状性患者43例(36例卒中, 6例TIA, 1例一过性黑朦, 表1)。症状性患者高脂血症病史明显高于无症状性患者(P=0.005), 并且二者的吸烟史差异也具有统计学意义(P=0.049)。症状性患者与无症状性患者动脉造影狭窄度分别为80.9%± 10.5%和81.7%± 7.7%, 二者差异无统计学意义(Z=-0.418, P=0.676)。两组的年龄、性别、BMI、高血压、糖尿病、冠心病、既往脑卒中病史差异无统计学意义。
| 表1 研究人群特征 Table 1 Clinical characteristics of the study population |
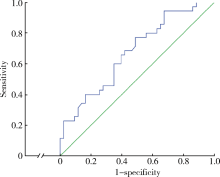
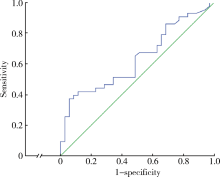
无症状性患者与症状性患者颈动脉斑块体积与比例见表2, 发现无症状患者的钙化斑块比例明显高于症状性患者(t=2.760, P=0.007), 而脂质斑块比例低于症状性患者(Z=-2.009, P=0.044)。两组的斑块体积与纤维斑块比例差异无统计学意义。无症状性斑块与症状性斑块的多因素分析见表3, 在模型Ⅰ 中, 仅高脂血症和钙化斑块比例与症状之间差异有统计学意义; 高脂血症患者与非高脂血症患者相比, 出现症状的危险是4.72倍(P=0.006), 而钙化斑块比例与无症状性颈动脉狭窄呈正相关(OR=0.949, 95%CI: 0.915~0.985, P=0.005); 在模型Ⅱ 中, 高脂血症和脂质斑块比例与症状之间差异有统计学意义; 高脂血症患者颈动脉斑块出现症状的危险是非高脂血症患者的4.26倍(P=0.01), 而脂质斑块比例与无症状性颈动脉狭窄呈负相关(OR=1.068; 95%CI:1.021~1.117, P=0.004)。钙化及脂质斑块ROC曲线表明(图3、4), 当钙化比例为40.6%时, 检测无症状的敏感度为 65.7%, 特异度为60.5%(ROC=0.674; 95%CI:0.555~0.793, P=0.009)。对于症状性患者, 当脂质斑块比例大于 30.3%时, 其特异度为 94.3%, 敏感度为 37.2%(ROC=0.633, 95%CI:0.510~0.756, P=0.045)。
| 表2 研究人群的斑块特征 Table 2 Plaque volume and proportion of the study population |
| 表3 斑块比例与临床特征的多因素分析 Table 3 Multivariable analysis for the associations between plaque proportions and clinical characteristics |
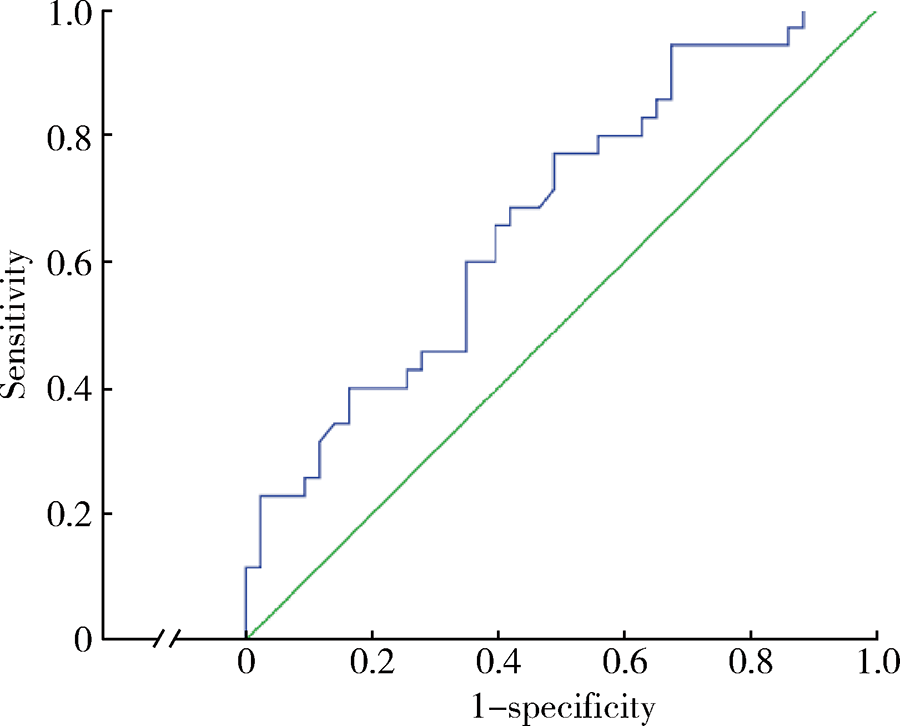 | 图3 钙化斑块的ROC曲线图Figure 3 The ROC curve for calcified plaque proportionThe area under the curve was 0.674. |
 | 图4 脂质斑块的ROC曲线图Figure 4 The ROC curve for LRNC plaque proportionThe area under thecurve was 0.633. |
通过其中25例斑块体积和比例进行重测信度检验, ICC结果表明, 脂质斑块体积 (ICC=0.996, P< 0.01)、纤维斑块体积(ICC=0.997, P< 0.01), 钙化斑块体积(ICC=0.996, P< 0.01)均显示具有良好重测信度。
本研究通过MDCTA斑块分析技术, 比较症状性和无症状性颈动脉狭窄患者的斑块成分和比例的差异, 结果表明颈动脉斑块中钙化的比例与症状呈负相关, 而脂质斑块的比例与症状呈正相关。在心血管危险因素中, 多因素分析表明高脂血症与症状性颈动脉狭窄呈正相关。两组的斑块体积和纤维斑块比例差异无统计学意义, 表明钙化比例增加及脂质比例减少(而非体积)与无症状性颈动脉狭窄斑块相关。
MDCTA可以对颈动脉在轴位、矢状位、冠状位等多平面进行重建。斑块钙化、纤维斑块厚度、脂质坏死核心可以通过不同的CT值来确定。某些斑块的肉眼改变, 如较大的出血及坏死核心, 可以通过MDCTA鉴别[16]。此外, MDCTA在发现溃疡斑块和血管生成方面也很有效, 其敏感度和特异度达90%[17]。De Weert等[10]对15例症状性颈动脉狭窄大于70%的患者进行研究, 结果表明区分脂质核心与纤维组织、纤维组织与钙化的截点值分别为60和130 HU, 与病理组织相比有较好的相关性(R2> 0.73)。综上, MDCTA作为一种无创的影像学方法, 可以对颈动脉斑块所致的狭窄以及成分进行有效的评价。
Nandalur等[13]对行MDCTA检查的102例颈动脉狭窄≥ 50%患者进行研究(症状性35例, 无症状性67例), 发现颈动脉狭窄钙化的比例与斑块稳定相关, 而钙化的比例大于45%可能代表一个有用的截点, 其特异度为97.1%, 敏感度为28.4%。本研究的结果也表明钙化比例增加与斑块稳定相关, 这与Nandalur 等[13]的结果类似。当钙化的比例大于45%, 其特异度为64.1%, 敏感度为54.3%, 与Nandalur 等[13]的研究结果不同, 可能是由于样本选择以及入组患者狭窄程度的不同而得出相异的结果。在Nandalur 等[12]另一项包含31例颈动脉狭窄≥ 60%的研究中, 症状性15例, 无症状性21例, 结果也证实了引起颈动脉狭窄的钙化斑块比非钙化斑块更稳定。
此外, Kwee[18]的一项系统回顾表明症状性斑块比无症状性斑块有较低程度的钙化比例, 另有研究发现[19], 炎症反应在颈动脉粥样硬化斑块的不稳定性和破裂中起着关键作用, 而非钙化斑块比钙化斑块更容易发生纤维帽炎症反应, 表明颈动脉粥样硬化斑块钙化是斑块稳定性的一个指标。同时Shaalan 等[20]研究表明, 与无症状性斑块相比, 症状性斑块钙化含量减少而炎症反应强烈。颈动脉斑块钙化的程度和斑块的纤维帽炎症的强度呈反相关, 表明颈动脉斑块钙化与斑块稳定性密切相关。
除钙化斑块之外, 脂质斑块也与管腔狭窄、临床症状相关, 并且在颈动脉粥样硬化斑块进展中起着重要的作用[21]。脂质斑块的大小与颈动脉支架植入术时产生残核的数量有关, 而这些残核可导致临床缺血事件[22]。Wong等[23]通过一个颈动脉钙化斑块的三维模型发现钙含量的增加与脂质核心含量的降低可以使斑块结构保持稳定。本研究也表明症状性颈动脉狭窄患者脂质斑块的比例高于无症状性患者, 当脂质斑块比例大于30.3%时, 其特异度为94.3% 。
在动脉粥样硬化斑块发生发展过程中, 当脂质坏死核心形成时, 斑块发展成为纤维粥样斑块, 斑块的稳定与表面的薄纤维帽有关。在一个包含44例颈动脉内膜剥脱术标本研究中[24], 其中19例为症状性患者, 发现纤维帽变薄与症状性斑块有关。在英国牛津大学进行的斑块研究表明, 纤维帽在病理组织上小于200 μ m考虑斑块易于破裂[25]。本研究发现脂质斑块比例增高与斑块不稳定性有关, 但是脂质斑块比例与薄纤维帽是否相关及机制还需要进一步证实。
此外, 斑块表面多态性如斑块溃疡也在颈动脉狭窄表现症状上起着重要的作用[26], 斑块溃疡形成与斑块破裂、斑块内出血、大脂质核心、较少纤维组织及斑块不稳定增加有关。斑块表面多态性可以作为斑块不稳定的一个敏感标记物[27], Homburg等[28]通过MDCTA研究发现斑块体积、狭窄程度、脂质斑块比例与斑块溃疡形成有关, 从而能间接表明脂质斑块比例与斑块稳定性之间的相关性。
除了斑块成分比例之外, 本研究结果还显示高脂血症与症状性颈动脉狭窄斑块明显相关。在美国的一项前瞻性队列研究中[29], 纳入了27 937 位年龄≥ 45岁女性患者, 结果发现总胆固醇与低密度脂蛋白-胆固醇水平与缺血性脑卒中风险增加明显相关。脂质在血管壁上的沉积是动脉粥样硬化斑块形成的特性之一, 并参与斑块的发展[30], 而斑块的稳定与表面的薄纤维帽有关。这些薄纤维帽纤维粥样斑块通常见于总胆固醇水平升高、总胆固醇与高密度脂蛋白-胆固醇的比值升高及年龄大于50岁的女性患者[31], 并且应用他汀类药物降脂治疗可减少动脉粥样硬化患者脑卒中发生的风险[32], 说明高脂血症患者与非高脂血症患者相比, 颈动脉斑块出现症状的风险增加。
本研究尚存在不足之处:首先, 本项研究为回顾性队列研究, 没有对溃疡斑块等斑块多态性进行精确影像学评价; 其次, 由于钙化与高浓度对比剂边界欠清晰, 可能导致斑块体积或比例测量结果出现偏差; 第三, 通过CT值区分纤维斑块与脂质斑块可能出现部分容积效应, 导致结果产生测量误差; 第四, 非钙化斑块如斑块内新生血管生成, 在应用对比剂后可能出现斑块CT值增加; 第五, 症状与颈动脉狭窄程度存在一定的相关性, 使本研究有一定的偏倚, 但是两组之间的狭窄程度差异无统计学意义, 可以基本排除两组间的混杂因素。此外, 本研究选取狭窄程度≥ 70%者, 范围过大, 没有进行亚组分析, 考虑各亚组人群数量较少, 且不同斑块在人群中分布存在差异, 对统计学分析有一定影响, 需要后续大样本量的研究进一步论证。
综上所述, 应用MDCTA可以无创测量颈动脉狭窄斑块的成分体积和比例, 钙化斑块比例增加及脂质斑块比例减少(而非体积)与无症状性颈动脉狭窄相关, 脂质斑块比例大于30.3%在临床上可以作为预测症状性斑块一个有用的节点, 对于颈动脉狭窄患者, 可以应用多层螺旋CTA斑块分析进行风险评估。
(本文编辑:王 蕾)
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|