{kind=link}
释氟高流动树脂在儿童早期釉质龋窝沟封闭中的应用
[闫文娟, 郑佳佳, 陈小贤△  ]
]
]
|
|


目的: 评价释氟高流动性树脂对儿童恒牙早期釉质龋进行窝沟封闭的临床应用效果,并与传统窝沟封闭剂做对比。方法: 临床纳入76名儿童,共52对第一恒磨牙和30对恒前磨牙,双侧同名牙均根据国际龋齿检测与评估系统(International Caries Detection and Assessment System,ICDAS)龋齿诊断标准诊断为早期釉质龋,采取自身双侧对照研究方法,随机选择一侧恒牙作为实验组,使用释氟高流动性树脂进行窝沟封闭,对侧同名牙作为对照组,使用传统窝沟封闭剂,在3、6、12、24个月进行临床观察比较,评价窝沟封闭剂的保存率和龋齿的进展情况。结果: 使用释氟高流动树脂及传统窝沟封闭剂对恒前磨牙进行窝沟封闭后3个月和6个月均无封闭剂脱落和龋齿进展,12个月和24个月对照组各有1例发生封闭剂脱落,差异无统计学意义。第一恒磨牙实验组在封闭后3、6、12和24个月封闭剂完全保存率分别为100%、98.08%、90.38%和88.46%,而传统窝沟封闭组分别为96.15%、92.31%、76.92%和73.08%, 封闭后24个月实验组封闭剂完全保存率明显高于对照组,差异有统计学意义( P<0.05)。封闭后6、12和24个月实验组龋齿进展率分别为1.92%、5.77%和7.69%,对照组分别为5.77%、19.23%和25.00%,12个月及24个月时实验组龋齿进展率明显低于对照组( P<0.05)。结论: 与传统窝沟封闭剂相比,采用释氟高流动性树脂对儿童恒磨牙早期釉质龋窝沟封闭可以提高窝沟封闭剂保存率,且能有效阻止龋齿发展。
Objective: To evaluate the clinical effect of fluoride releasing flowable resin used in treatment of early enamel caries of children compared with conventional sealant.Methods: Seventy-six patients, including fifty-two couples of permanent first molars and thirty couples of premolars were selected for this trial. Both sides of all the molars and premolars were diagnosed as early enamel caries based on International Caries Detection and Assessment System (ICDAS) dental caries diagnostic criteria. Using the contralateral control, the teeth were randomly divided into two groups. Molars/premolars in the expe-rimental group were sealed with a fluoride releasing flowable resin; the contralateral molars/premolars were sealed with a conventional fissure sealant as a control group. The retention rate and progress of caries were evaluated at the end of 3, 6, 12 and 24 months.Results: There was no fissure sealant loss or caries progression in both groups 3 and 6 months after sealing the premolars by fluoride releasing flowable resin or conventional fissure sealants. At the end of 12 and 24 months, only one case of fissure sealant loss was observed in conventional fissure sealant group. There was no statistical significance between the two premolar groups. In the first molar group, fluoride releasing flowable resin showed 100%, 98.08%, 90.38% and 88.46% complete retention at the end of 3, 6, 12 and 24 months, respectively. The conventional fissure sealant retention rates were 96.15%, 92.31%, 76.92% and 73.08% at the corresponding time points. The data at the end of 24 months showed that fluoride releasing flowable resin had significantly higher retention rate than the conventional fissure sealant group ( P<0.05). The incidence of caries progression at the end of 6, 12 and 24 months were 1.92%, 5.77% and 7.69%, respectively, in the fluoride releasing flowable resin group. In the conventional fissure sealant group, the incidence was 5.77%, 19.23% and 25.00%, respectively. At the end of 12 and 24 months, more significant decrease of caries progress incidence was observed in the fluoride releasing flowable resin group than in the control group, and there was statistical difference between the two groups ( P<0.05).Conclusion: Compared with conventional fissure sealant, using fluoride releasing flowable resin as a fissure sealant in children enamel caries of permanent molars can improve the sealant preservation rate and effectively prevent enamel caries progress.
儿童的年轻恒磨牙由于釉质表面结构疏松、多孔, 窝沟点隙多而复杂, 细菌容易在其表面聚集, 加之儿童喜食软质食物且口腔清洁能力较差, 因而在初萌出时极易患龋[1]。根据我国2015年第四次全国口腔健康流行病学调查结果显示, 12岁年龄组儿童恒牙患龋率为 34.5%。年轻恒牙的龋齿多发于点隙窝沟处, 因此, 窝沟龋的预防和治疗尤为重要。
流动性充填材料是20世纪90年代末开发出的材料, 由于其降低了填料比例, 具有一定的渗透性和流动性, 可以方便地封闭窝沟, 用于小面积龋损的充填[2]。研究发现, 释氟的树脂类材料进行窝沟封闭的保存率明显高于传统窝沟封闭剂[3, 4]。儿童恒牙由于釉质表面结构的特点, 容易受到环境因素的作用发生再矿化, 再矿化对于阻止龋病发展、预防龋病发生具有重要作用[5, 6]。释氟高流动性树脂一方面可以渗入窄而深的窝沟部位, 有一定的粘接力, 另一方面还可缓慢释放一定量的氟, 能够预防龋齿并促进早期釉质龋发生再矿化, 从原理上可用于窝沟封闭。本研究拟采用释氟高流动性树脂对年轻恒牙早期龋进行不备牙的窝沟封闭, 并观察其临床效果, 为早期龋的治疗寻求一种更符合微创理念的治疗方式。
本研究获得北京大学口腔医院生物医学伦理委员会审查批准。选择就诊于北京大学口腔医院门诊部儿童口腔科的6~13岁儿童76名, 共纳入82对牙齿, 包括第一恒磨牙52对(年龄6~9岁)和恒前磨牙30对(10~13岁)。纳入标准:(1)牙合面完全暴露, 无龈瓣覆盖; (2)双侧同名牙均根据国际龋齿检测与评估系统(International Caries Detection and Assessment System, ICDAS)龋齿诊断标准诊断为早期釉质龋(ICDAS code 2), 诊断方法:湿润状态下视诊检查窝沟, 龋损呈不透明状(白色斑点)和/或褐色, 龋损变色的范围超过正常的窝沟, 与临床上健康的釉质形态不一致, 吹干牙面后病损依然可见[7]。排除标准:(1)有邻面龋损者; (2)牙合面有充填体; (3)色素沉着、釉质发育不全、氟牙症及四环素牙。
采用自身同颌同名牙作为对照, 随机数字表简单随机分组。将双侧恒磨牙/恒前磨牙(同为上颌或下颌)分入对照组和实验组:一侧为实验组, 采用释氟高流动性树脂进行窝沟封闭; 另一侧为对照组, 采用传统窝沟封闭材料进行窝沟封闭。
临床操作由同一名医师完成。毛刷蘸清水清洁牙面, 压缩空气干燥牙齿表面。实验组:酸蚀牙面, 清水加压冲洗, 吹干牙面, 涂布粘接剂(Single Bond Universal Adhesive, 美国3M公司)并吹匀, 光固化后涂布释氟高流动树脂(Beautifil Flow F10, 日本Shofu公司), 探针去除气泡, 光固化, 检查确认所有窝沟完全封闭后进行调牙合、磨光。对照组:酸蚀牙面, 清水加压冲洗, 吹干牙面, 涂布传统窝沟封闭剂(ESPETM Concise, 美国3M公司), 探针去除气泡, 光固化, 检查确认所有窝沟完全封闭后进行调牙合、磨光。分别于窝沟封闭后3、6、12和24个月复查, 对封闭剂保存情况及龋齿是否发生进展进行记录。
(1)封闭剂保存率:包括完全保存率、部分保存率、完全脱落率。完全保存是指所有窝沟、点隙封闭剂固位好, 没有变色和脱落; 部分保存指窝沟封闭剂部分脱失; 完全脱落指窝沟封闭剂全部脱落。(2)龋齿进展率:发生龋齿进展的牙数/受检牙数× 100%。
采用 SPSS 17.0进行统计分析, 绘制Kaplan-Meier生存曲线, 采用时序检验(Log-rank)对两组间窝沟封闭保存率进行比较, 生存时间定义为牙齿进行窝沟封闭至封闭剂发生脱落之间的时间。龋齿进展情况比较采用配对卡方检验, P< 0.05为差异有统计学意义。
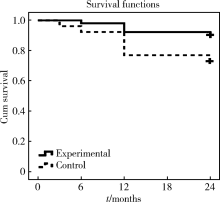
共76名儿童的52对第一恒磨牙和30对恒前磨牙完成本研究。恒前磨牙实验组和对照组在术后3个月、6个月均未发生封闭剂脱落和龋齿进展, 12个月和24个月时对照组各有1例发生封闭剂部分脱落, 但均未见龋齿进展, 两组间差异无统计学意义(P> 0.05)。第一恒磨牙实验组在术后3、6、12和24个月封闭剂完全保存率分别为100%、98.08%、90.38%和88.46%, 而传统窝沟封闭组保存率分别为96.15%、92.31%、76.92%和73.08%(表1), Kaplan-Meier生存分析提示, 窝沟封闭后24个月实验组封闭剂完全保存率明显高于对照组, 差异有统计学意义(P=0.044, 图1)。
| 表1 第一恒磨牙组窝沟封闭保存率(n=52) Table 1 Sealant preservation rate in the first molars group (n=52) |
 | 图1 第一恒磨牙组窝沟封闭保存率(Kaplan-Meier分析)Figure 1 Clinical survival probabilities of sealants in the first molars group (Kaplan-Meier analysis) |
窝沟封闭后3个月两组龋齿均无明显进展, 窝沟封闭后6、12和24个月两组均有龋齿发生, 实验组龋齿进展率分别为1.92%、5.77%和7.69%, 对照组分别为5.77%、19.23%和25.00%, 其中12及24个月时实验组龋齿进展率低于对照组, 差异有统计学意义(P< 0.05, 表2)。
| 表2 第一恒磨牙组龋齿进展发生率(n=52) Table 2 Caries progress incidence in the first molars group (n=52) |
年轻恒牙的窝沟点隙处是龋病的好发部位, 传统的龋齿治疗需除尽龋坏组织, 并需制备一定的固位洞型, 在一定程度上会造成健康牙体组织的损失。对于年轻恒牙的釉质龋, 临床上常采用预防性树脂充填或者窝沟封闭进行治疗。预防性树脂充填技术仅去除病变牙釉质或牙本质, 不进行预防性扩展, 对早期窝沟龋进行充填并在牙合面上涂一层封闭剂, 是一种窝沟封闭与窝沟龋充填相结合的方法, 适用于小的窝沟龋和窝沟可疑龋的治疗[8, 9]。预防性树脂充填能有效阻止龋病发展, 但需磨除一定量的健康牙体组织, 因此, 对于咬合面的未成洞龋损, 窝沟封闭术无需进行牙体预备, 是比较理想的修复方法[10]。
窝沟封闭是指在牙齿的咬合面、颊面或舌面的点隙裂沟涂布粘性树脂, 以隔绝细菌及代谢产物对点隙裂沟组织的侵蚀, 达到预防龋坏发生的作用[11]。窝沟封闭不仅可用于预防健康牙齿窝沟龋的发生, 还可用于局限于釉质的窝沟早期龋的修复治疗[12, 13]。研究证实, 对于未成洞的早期龋齿进行窝沟封闭, 龋损可停止进展[13]。封闭剂的保存率直接影响窝沟封闭的防龋效果[14], 因牙齿窝沟的形态复杂多样, 龋的诊断有一定的难度, 如果把无粘接性且不含氟的封闭剂直接涂抹在有活动龋的牙面上, 则封闭材料较易脱落, 且可能使龋坏在更隐蔽的环境里继续发展。研究证实, 对釉质龋进行预防性树脂充填后12个月, 完全保存率约为91.4%, 但如果在脱矿的釉质上进行窝沟封闭, 其封闭剂完全保存率仅为71.7%[15, 16]。
如何提高窝沟封闭剂保存率又尽可能不去除牙体组织是治疗早期龋的关键。释氟高流动树脂具有一定的渗透性和流动性, 可在临床上作为窝沟封闭材料使用。本研究结果显示, 对前磨牙早期釉质龋进行窝沟封闭, 无论是使用流动树脂还是传统窝沟封闭剂均取得了良好的效果, 这与前磨牙的窝沟形态较为简单且所处口腔位置较为靠前, 比较容易清洁有关。第一恒磨牙实验组和对照组的完全保存率在封闭后3和6个月时没有明显差异, 封闭后12和24个月时实验组完全保存率分别为90.38%和88.46%, 与以往文献报道的预防性树脂充填的保存率相近[16, 17], 24个月时完全保存率明显高于传统窝沟封闭剂组(73.08%)。
釉质龋的病损仅限于牙齿表层, 表现为组织脱矿, 微晶溶解, 晶体间孔隙增大。儿童恒牙由于釉质表面的结构特点, 容易受到环境因素的作用发生再矿化, 再矿化对于阻止龋病发展、预防龋病发生具有重要作用[18]。释氟高流动性树脂是利用表面预先反应玻璃离子(surface pre-reacted glass ionomer, S-PRG)技术研发而成的, S-PRG填料表面可由唾液形成一层保护膜, 有抑制菌斑聚集的效果, 且S-PRG填料具有玻璃离子稳定相, 能够根据口腔内的氟离子浓度释放和再充氟, 为促进早期釉质龋的再矿化创造了有利条件。本研究中, 窝沟封闭后12及24个月第一恒磨牙实验组龋齿进展率(5.77%, 7.69%)明显低于对照组(19.23%, 25.00%), 差异有统计学意义。
综上, 应用释氟性的流动树脂对恒磨牙早期釉质龋进行窝沟封闭, 既避免了传统充填治疗法磨除健康的牙体组织, 又可以有效的提高窝沟封闭剂保存率, 阻止龋齿发展, 更加符合临床治疗的微创原则, 具有较高的临床应用价值, 是治疗年轻恒牙窝沟早期龋的一种有效方法。
(本文编辑:赵 波)
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|