1. 吉林大学中日联谊医院 耳鼻咽喉头颈外科, 长春 130000
2. 吉林大学中日联谊医院 骨科, 长春 130000
收稿日期: 2016-11-02
基金资助: 吉林省科技发展计划项目(20150204062SF)
中图分类号:R653
文献标志码:A
文章编号:1671-167X(2018)05-0924-04
Analysis of 2 cases of dyspnea happening after tracheotomy and the clinical application of Mimics 10.01
1. Department of Otorhinolaryngology, China-Japan Union Hospital, Jilin University, Changchun 130000, China
1. Department of Otorhinolaryngology, China-Japan Union Hospital, Jilin University, Changchun 130000, China
△ Corresponding author’s e-mail,
wh15@163.com
Fund:Supported by Jilin Province Science and Technology Development Project (20150204062SF)
气管切开术是耳鼻咽喉头颈外科最常见的开放气道的手术之一, 而术后再次出现吸气性呼吸困难症状较为少见, 吉林大学中日联谊医院耳鼻咽喉头颈外科接诊2例气管切开术后再次出现喉梗阻的患者, 报道如下。
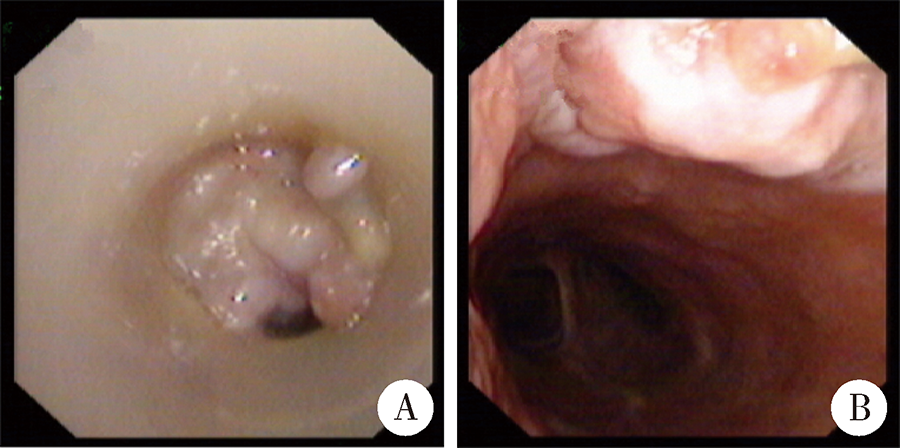
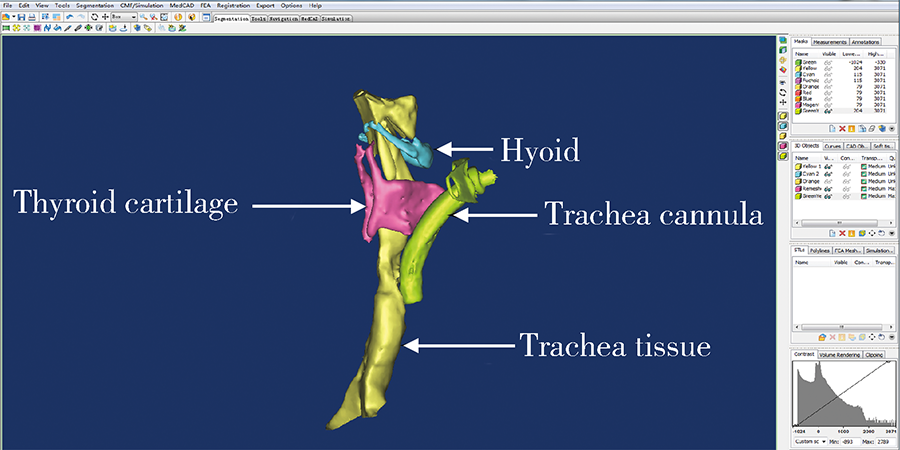
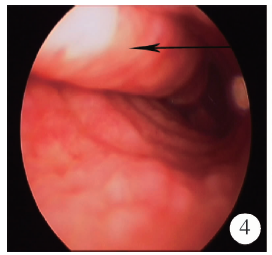
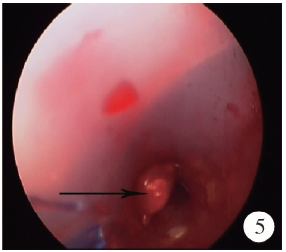
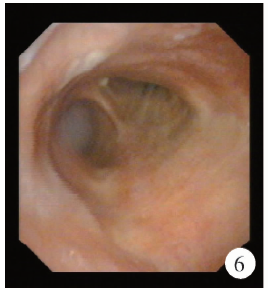
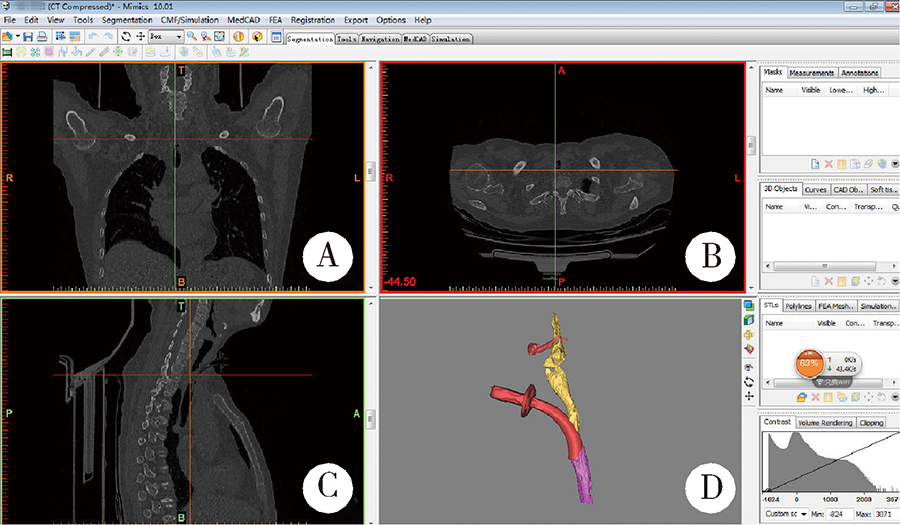
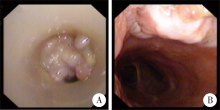
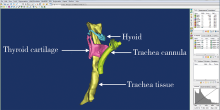
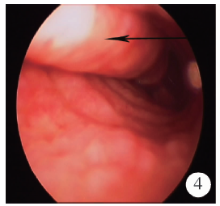
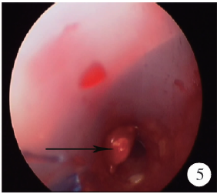
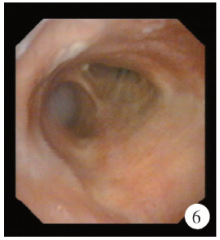
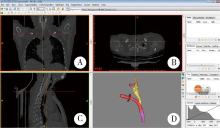
1 病例资料病例1, 患者男性, 86岁, 因气管切开术后2年、气道狭窄松解术后5个月、呼吸困难1周就诊于吉林大学中日联谊医院耳鼻咽喉头颈外科。该患者2年前因肺内感染并呼吸困难于当地医院行紧急气管切开术后置入铁质气管套管。既往因呼吸费力就诊于当地医院见气管套管内下端可见不规则新生物, 更换为聚氯乙烯 (polyvinylchloride, PVC) 气管套管并行激光手术后上述症状缓解, 1周前呼吸困难呈渐进性加重来吉林大学中日联谊医院耳鼻咽喉头颈外科就诊。患者既往强直性脊柱炎病史12年, 脑梗死、帕金森综合征病史10年。查体:患者侧卧位, 张口呼吸, 颈部活动受限, 三凹征阳性, 血氧饱和度在88%~98%之间。PVC气管套管外口平对环状软骨水平, 套管末端不通畅, 套管口及口鼻均有少许气流。电子喉镜示:双侧声带固定在旁正中位, 外展受限。声门下可见气管壁管状隆起, PVC气管套管套囊壁末端部分突出于气道内, 周围见大量肉芽组织(图1), 套管不通畅。CT仿真支气管镜示:气管内可见插管影, 插管与气管中段未见明显相通, 插管末端处气管管腔内壁局部向内突出(图2), 但上述CT仿真支气管镜对于PVC气管套管插入高度及与周围骨性标志的关系显示不佳, 应用Mimics 10.01 (比利时Materi-alise公司) 软件, 进行骨性结构三维重建后(图3), 发现PVC气管套管切口位置过高, 约位于环甲膜水平, 且部分PVC气管套管嵌入假腔(图4)。患者既往病史造成颈椎活动度差及声门外展受限, 实行麻醉插管及静脉吸入复合麻醉风险极高, 故于正压通气及局部麻醉下, 行硬质直达喉镜引导下PVC气管套管还纳术(图5), 将PVC气管套管沿原气管瘘口置入。同时于电子喉镜监视下应用半导体激光(波长 808 nm, 功率13 W, 连续脉冲)行肉芽组织切除术。术后, 患者血氧饱和度维持在98%~99%之间, 张口呼吸及三凹征消失。经抗感染及对症治疗, 术后2周再次于吉林大学中日联谊医院耳鼻咽喉头颈外科门诊局部麻醉下清除残余肉芽组织, 现患者随访1年, 未见以上症状复发, PVC气管套管在位、通畅(图6)。
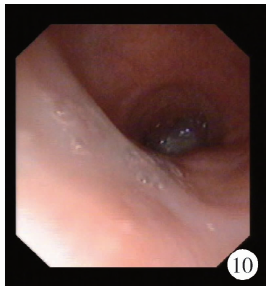
病例2, 患者女性, 57岁, 因气管切开术后1年, 再次出现呼吸困难就诊于吉林大学中日联谊医院耳鼻咽喉头颈外科。既往于吉林大学第四医院明确诊断为脑出血, 患者术前血氧饱和度不能维持于90%以上, 故于局部麻醉下行气管切开术, 应用呼吸机辅助呼吸, 再在静脉吸入复合麻醉下行血肿清除去骨瓣减压术。专科查体:PVC气管套管在位, 气管套管末端不通畅。电子喉镜检查示气管狭窄, 呈扁平状, 后壁可见肉芽样隆起, 表面光滑(图7)。行CT仿真支气管镜检查, 见气管狭窄, 狭窄部位以前后径为主, 但CT仿真支气管镜尚不能很好显示PVC气管套管与狭窄部位之间位置关系, 同时无法判断狭窄部位来源于气管塌陷还是软组织增生, 因而应用Mimics 10.01软件, 进行骨性结构三维重建后(图8)见PVC气管套管口局限性黏膜隆起, 气管软骨环完好, 呈扁平状(前后径/左右径< 0.93), 遂于1%(质量分数)丁卡因局部麻醉下, 经电子喉镜引导, 应用半导体激光(波长 808 nm, 功率13 W, 连续脉冲)行肉芽组织切除术(图9)。术后患者无明显不适主诉, 术后随访半年, 患者无呼吸困难, 术后复查电子喉镜, 可见气管壁黏膜光滑(图10)。
2 讨论紧急气管切开术是耳鼻咽喉头颈外科较为棘手的危机情况, 而气管切开术之后再次出现气道阻塞是该术式危险的晚期并发症之一。患者会因气管未能及时开放而造成窒息、乏氧, 严重时甚至死亡。
回顾以上病例, 发现上述两个病例存在一定共性:首先患者均合并系统性疾病, 需要长期带气管套管以开放气道, 排出分泌物, 带管时间超过1年; 其次患者均为紧急情况下行气管切开术, 操作与准备时间较短。Fiorini等[1]对300多例气管切开患者进行随访, 发现急诊气管切开与常规切开相比, 前者发生并发症如气管狭窄、气管黏膜阻塞气管口等比率明显增高, 这可能是由于急诊情况导致PVC气管套管放置位置错误或者置入PVC气管套管过程中损伤气道黏膜所致。Hillel等[2]对小鼠模拟进行气管切开术, 并对实验组小鼠在气管切开同时模拟PVC气管套管置入气道内可能发生的机械损伤, 发现存在气道机械损伤小鼠与无气道损伤小鼠相比, 气管切开术2周后, 前者的气管黏膜固有层明显增厚, 出现纤维化。本病例1 PVC气管套管长期置于气道内, 会与气管壁黏膜产生摩擦, 且行气管切开术位置过高, 使得PVC气管套管弧度与气管弧度不适应, 产生摩擦与压迫, 气道反复炎症刺激使气管黏膜及黏膜下组织出现了重塑, 损伤导致黏膜固有层增厚、肉芽增生。肉芽组织包裹PVC气管套管, 形成假腔, 由于套管部分通畅, 且套管未占据整个气管管腔, 患者早期可能不会产生呼吸困难等症状, 随着肉芽组织生长增大, 逐渐堵塞套管, 患者出现呼吸困难。另外, 长期气管套管的置入导致组织重塑, 进而出现气管狭窄。Lee等[3]对兔进行气管切开及置管, 发现气管切开后置管1周55%兔子出现气管狭窄, 置管2周84%兔子会出现气管狭窄。对这些兔子气管组织进行免疫组织化学分析发现:气管纤毛柱状上皮出现鳞状上皮化生以及肥厚, 固有层增厚及纤维化和不同程度新生血管, 因而对于长期置管患者, 不同程度的会出现气道狭窄, 导致气管切开后呼吸困难出现。本病例2气管切开1年以上, Mimics 10.01软件重建后可见气道狭窄, 以前后径减小为著, 考虑可能与长期置管后出现的气道重塑以及炎症刺激导致软骨环软化有关。以上原因导致的气道开放失败, 可能是早期即存在或是缓慢产生, 但患者早期均未出现呼吸困难, 未能引起足够重视, 当产生相应症状时, 往往保守方式已经很难达到治疗目的。
气管切开术中, 应尽量准确选择切开部位, 置入PVC气管套管应尽量轻柔, 避免暴力导致的气管黏膜损伤与撕脱, 选择合适直径与角度的套管, 避免套管与气管管壁长期接触而导致的气管黏膜损伤。Kirschbaum等[4]对气管切开并发症进行总结后提到:气管切开后, 损伤的气道黏膜可能造成气管硬化, 这是气管切开的晚期并发症之一。Gronhoj等[5]对气管切开的并发症进行统计, 结果发现气管切开后出现气道内肉芽生长的患者比例高达13%。行气管切开术后, 应常规复查电子喉镜, 可同时选取从声门及PVC气管套管口两个方向入路, 确认套管是否在位。对于一些声门无法正常张开的患者, 如脑梗死、甲状腺术后喉返神经损伤等患者, 可应用CT仿真支气管镜, 确认PVC气管套管是否在位, 腔内黏膜情况如何, 是否存在狭窄, 这是良好的无创、直观的确认PVC气管套管在气管内情况的方法, 但CT仿真支气管镜对于骨质的重建效果不佳, 这主要因为现有的影像学工作站, 仅能对图像进行表面重建, 而对于深层的组织情况无法重建, 没有骨性解剖标志对于定位PVC气管套管位置就变得尤为困难, 断层CT扫描虽然可以显示软组织与骨质之间的关系, 但显然不够直观。然而Mimics 10.01软件[6]处理后的CT图像, 可以对于整个气道进行三维重建, 并且通过后期处理(如反向阈值), 对软组织、骨质图像分别进行重建, 可以根据需要对两种组织进行拟合与拆分, 使得PVC气管套管与骨质、软组织的解剖关系都更为直观, 对于骨性标志的重建可以更准确地判断PVC气管套管的位置, 对于组织的重建可以判断出气管狭窄来源于气管黏膜还是骨质塌陷, 拟合的图像可以分析骨质与软组织间的解剖关系, 协助锁定狭窄的黏膜所在位置, 为手术方案的制定提供一定依据。Kirschbaum等[4]对1例患者行经皮气管切开术时由于选取位置过低, 导致术后患者脱管, 且还纳困难, 他们总结认为盲视下的操作容易造成气管瘘口的出现, 进一步加重气道与纵膈的损伤, 最终采取了胸腔镜监视下松解气管硬化部位以及PVC气管套管的还纳。本文中的病例采用硬质直达喉镜引导下的PVC气管套管还纳术, 精准地使PVC气管套管进入气道中, 避免再次误入肉芽形成的假性通道, 是一种值得借鉴和推广的方法。内窥镜下针对气道的硬化可以采取多种治疗方法, 比如球囊扩张、支架置入、二氧化碳激光切除、电切除、氩气刀凝固法、局部应用丝裂霉素以及冷冻疗法[7, 8]等。如果气管切开后气道出现网状的气道硬化, 激光切除是首选的方法, 因为激光的应用有助于保护气道黏膜[9]。应用半导体激光对肉芽进行灼烧, 术后效果明显, 术中可以根据肉芽组织的硬韧程度具体选择激光的功率, 可在11~14 W之间, 肉芽越硬韧, 使用激光的功率应相应增高。另外, 由于激光自身特性, 当遇到液体时会出现衰减[10], 使功率降低, 因而, 在急性烧灼之前, 务必将肉芽及气道内分泌物充分清理, 以保证激光的应用效果。本文2例患者应用激光烧灼肉芽组织, 对于长期带PVC气管套管出现气道肉芽生长的其他患者同样具有借鉴意义。
(本文编辑:刘淑萍)
The authors have declared that no competing interests exist.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 ]
]