
{kind=link}
{kind=link}
肾蒂旋转法辅助治疗后腹腔镜下腹侧肾肿瘤的肾部分切除术
[梁银华1 , 祖雄兵2 , 程序, 刘龙飞△  ]
]
]
|
|


目的:为降低后腹腔镜入路的腹侧肾部分切除术手术难度,减少手术风险,总结归纳并发展后腹腔镜入路肾部分切除术的肾蒂旋转法及相关技术。方法:总结归纳并发展一整套针对腹侧肾门区肾肿瘤的肾蒂旋转法操作技术,包括肾蒂旋转、双层缝合、早期开放动脉等。该技术有助于实施后腹腔入路的肾部分切除术,手术效果的评价由手术时间、热缺血时间、术中出血量、手术切缘、术后肾功能、手术并发症等组成。本研究回顾性分析中南大学湘雅医院28例腹侧肾肿瘤患者资料,其中15例为较复杂的肾门区肿瘤。结果:平均肿瘤大小为(3.8±0.5) cm,平均R.E.N.A.L评分为8(范围7~9)。手术中平均热缺血时间(23.8±4.7) min,缝合时间(26.2±6.5) min,估计失血量(139.1±54.0) mL,手术时间(124.1±12.1) min,中位住院天数为4 d。7例患者出现Clavien Dindo Ⅰ~Ⅱ级并发症,所有患者病理检查均示切缘阴性,中位随访7个月无局部复发或远处转移。结论:对于腹侧肾肿瘤,尤其是位于肾门区的肾肿瘤,利用肾蒂旋转法行后腹腔镜下肾部分切除术是安全有效的;短时间随访结果较乐观,但需长时间随访。
Objective:Retro-laparoscopic partial nephrectomy is a challenge for ventro-renal tumors, especially hilar tumors. The tumors are partial or entirely out of operative field and there is blind space for operation. To solve this problem, a set of techniques including renal pedicle rotation is developed.Methods:A set of techniques including renal pedicle rotation, double-layer suture, early artery unclamping for retro-laparoscopic nephrectomy for ventro-renal tumors, especially hilar tumors were developed. Hilar tumors were located anteriorly to the angle of the renal and renal arteries and in contact with the anterior surface of the renal artery. The evaluation of the outcomes included the operation time, warm ischemia time, estimated haemorrhage, surgical margin, renal function after operation, and complications. This study reviewed the data of 28 patients with ventro-renal tumor, including 15 patients with complex hilar tumors.Results:The average tumor size was (3.8±0.5) cm. The average R.E.N.A.L score was 8 (ranging from 7 to 9). The average warm ischemia time was (23.8±4.7) min, and suture time was (26.2±6.5) min, and operation time was (124.1±12.1) min. The median hospital stay was 4 days and the average estimated haemorrhage was (139.1±54.0) mL. All the surgeries were operated under laparoscope and no surgery switched to open surgery. Seven patients developed Clavien Dindo Ⅰ-Ⅱ complications after operation. Three patients (10.7%) developed collective system damage and received repair of collective system in time and three patients (10.7%) developed slightly gross hematuria (Clavien-DindoⅠ). Two patients developed wound infection (Clavien-DindⅡ). Three patients (10.7%) got renal vein clamped because of capillary hemorrhage from basilar part of tumors. There were 14 patients received early unclamping of renal artery, and no obvious renal vessel damage was found. There were statistically significant differences between the serum creatinine levels ( P<0.05) and the estimated glomerular filtration rates ( P=0.02) before and after surgery. All the patients’ serum creatinine levels were in normal range and no patient needed regular dialysis. There was no positive surgical margin and the median follow-up was 7 months without local recurrence or distant metastasis.Conclusion:It is safe and effective to apply renal pedicle rotation technique in retro-laparoscopic partial nephrectomy for ventro-renal tumors. The short-term follow-up results are optimistic, but long follow-up is required.
腹腔镜下肾部分切除术已经成为小肾癌的首选治疗方式, 它具有保护肾功能、创伤小、恢复快等优势[1]。对符合该手术指征的患者行腹腔镜下肾部分切除术, 能得到与开放手术同等的效果, 肾功能恢复[2, 3, 4]的程度及肿瘤复发或转移[5]概率的差异无统计学意义。
腹腔镜下肾部分切除术最初被用在单发、外生性、靠近肾一极的小肾癌上, 或是用于孤立肾肾肿瘤、肾功能不全的患者。最近国外有报道, 腹腔镜下肾部分切除术被用于更大(如大小在4~7 cm)、位置更为复杂(如肾门区)的肿瘤[6, 7, 8, 9, 10, 11, 12, 13], 也得到较好的效果。
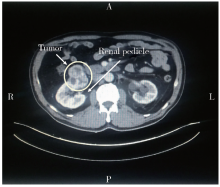
回顾性地选取中南大学湘雅医院2012年9月至2016年12月期间收治的28例腹侧肾肿瘤患者, 收集以肾蒂旋转法行后腹腔镜下肾部分切除术的病例资料。术前对所有患者均进行泌尿系彩超、泌尿系增强CT、肾血管增强及三维重建CT检查, 其中腹侧肾肿瘤即肿瘤位于肾腹侧、上极或下极或肾门区, 肾门区肾肿瘤的定义为术前CT及术中所见显示肿瘤位于肾门附近, 突出于肾表面且与肾血管或输尿管直接接触者(图1)。所有肾部分切除术均为非选择性阻断肾动脉, 术前行R.E.N.A.L评分[14]。研究方案符合人体试验伦理学标准, 并得到中南大学湘雅医院伦理委员会的批准, 所有受试者均签署知情同意书。
 | 图1 肾门区肿瘤, 白色箭头所指不均匀增强类圆形肿物即为肾肿瘤, 位于肾与肾动脉夹角前方, 与肾动脉前面相接触Figure 1 Hilar tumors, the white arrow directs an inhomogeneousen hancement of the round mass, which is a renal tumor, located anteriorly to the angle of the renal and renal arteries and in contact with the anterior surface of the renal artery |
所有患者采用三点法后腹腔镜下肾部分切除术, 麻醉后取健侧卧位, 切开皮肤, 制备后腹腔间隙, 置入穿刺套件, 建立二氧化碳气腹, 清除腹膜外脂肪, 切开肾筋膜。
肾蒂旋转:对于所有复杂的腹侧肾肿瘤行肾蒂旋转法(图2)。首先游离整个肾, 保留少部分肾周脂肪, 暴露肾蒂, 解剖清楚后游离肾动静脉及输尿管, 游离长度不可太短, 否则旋转后张力过大, 此时腹侧肿瘤并未进入术野。阻断肾动脉, 必要时同时阻断肾静脉, 记录夹闭时间。若肿瘤位于腹侧且更靠近上极, 则右手提起之前保留的上极肾周脂肪, 左手辅助推送肾下极, 轻柔地使下极绕肾蒂向腹侧旋转一定角度, 使腹侧肿瘤暴露在直视下。若肿瘤位置较高则旋转角度可稍小, 若肿瘤位于腹侧下极, 则可反向推送上极向腹侧, 使下极向背侧旋转, 从而将腹侧下极肿瘤暴露至背侧, 这样消除了手术视野的死角, 使肿瘤的切除及残肾的缝合更简单。
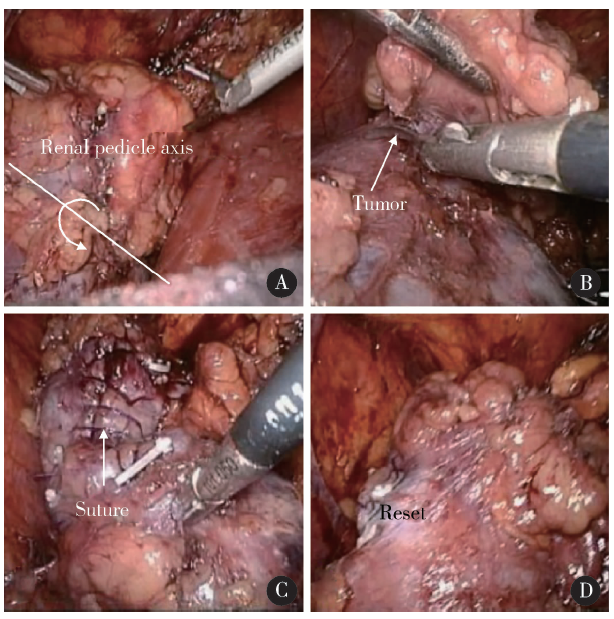 | 图2 肾蒂旋转法 A, the renal before rotation. The black line is renal pedicle direction as the rotation axis, and the arrow indicates the direction of rotation. Pick the upper mentioned kidney fat up gently around the renal pedicle rotation; B, the tumor was in the upper surgical field which originally located in ventral side after rotation, and can be cut easily; C, the tumor resection and suture after rotation; D, the reset ranal. The rotation direction is very important to avoid rotating in the same direction for a lap, resulting in unnecessary vascular injury.Figure 2 Renal-rotation technique |
肿瘤切除:暴露清楚后切除肿瘤, 提起肿瘤, 边缘留出0.5 cm进行裁剪。首先以锐性分离为主, 明确切除界限, 在肾皮质层内用剪刀锐性分离, 到达髓质层后处理肿瘤基底部时以剥离为主, 尽量保持术野清晰, 在锐性分离出的间隙内用抽吸器轻推肿瘤即可, 避免对肿瘤的破坏。肿瘤基底部较大的血管可以Hem-o-lok夹钳夹止血。
双层缝合:肿瘤切除完成后, 以可吸收免结线行双层连续缝合[15]。免结线应在术前准备好, 尾部夹Hem-o-lok夹以固定, 连续缝合中可继续用Hem-o-lok夹固定缝线, 一针一夹。首先内层缝合肾髓质, 旨在闭合肾实质深部的静脉以及修补可能的集合系统损伤。缝合不应过浅, 否则易导致止血不彻底, 引起术中或术后出血; 由于肿瘤基底部距离肾大动脉及集合系统较近, 亦不应缝合过深, 以避免损伤动脉及集合系统。
早期开放动脉:通常情况下, 由于较大静脉位于皮髓交界处, 内层缝合完毕后可尝试早期开放动脉, 若出血量不大, 术野清晰时, 可继续缝合外层, 若出血较多影响术野时, 则立即阻断动脉并于出血点补针, 必须待止血效果满意方可开放动脉。早期开放肾动脉不仅对肾功能恢复有帮助[16], 也有助于通过观察出血情况确认内层缝合效果。内层缝合完毕后外层用连续缝合加强内层缝合的效果。
完成后将肾复位, 将肾与邻近肌肉缝合固定, 并将标本快速病检。
术前统计患者性别、年龄、体重指数(body mass index, BMI)、肿瘤大小、R.E.N.A.L评分、血清肌酐、肾小球滤过率(estimated glomerular filtration rate, eGFR), 术中记录手术时间、热缺血时间、缝合时间、估计失血量、是否转开放手术, 术后随访3个月, 期间收集住院时间、有无输血、输血量、并发症、切缘状态、病理诊断、血清肌酐、肾小球率过滤等资料。
eGFR使用校正的肾病饮食改良(modification of diet in renal disease, MDRD)公式估算[17], 并发症分级采用Clavien-Dindo分级系统[18]。随访时由患者的临床表现结合最近一次影像学检查判断肿瘤是否复发。
应用SPSS 19.0处理统计数据。描述性数据用数字及百分比表示, 连续变量用均数± 标准差或均数和范围表示, 计数资料用例数和百分数表示。比较患者术前及术后的血肌酐、eGFR差异时用配对t检验和Wilcoxon符号秩和检验, 双侧P值< 0.05 则认为差异具有统计学意义。
28例患者均成功完成后腹腔镜下肾部分切除术, 男性18例, 女性10例, 年龄为(54.5± 10.5)岁。BMI为(25.3± 1.9) kg/m2, 肿瘤直径为(3.8± 0.5) cm, 所有患者均为单发肿瘤, 术前TNM分期为T1N0M0。R.E.N.A.L评分为7~9分, 平均8分。主要数据如表1。
| 表1 入选病例的一般资料 Table 1 General information of selected cases |
所有患者均行腹腔镜下肾部分切除术, 没有患者需要中转开放。平均估计出血量为(139.1± 54.0) mL, 没有患者术中或术后需要输血。热缺血时间为(23.8± 4.7) min, 缝合时间为(26.2± 6.5)min。3例患者由于肿瘤基底部渗血行肾静脉夹闭, 14例患者行早期肾动脉开放。平均手术时间为(124.1± 12.1) min, 未见明显肾蒂血管损伤。
3例(10.7%)患者出现术中的集合系统损伤并及时进行了修补。3例(10.7%)患者出现轻微的肉眼血尿(Clavien-DindoⅠ 级), 2例(7.1%)患者出现伤口感染(Clavien-DindⅡ 级)。患者术前和术后对比, 血清肌酐(P< 0.05)及eGFR(P=0.02)之间的差异有统计学意义, 术后所有患者血清肌酐均处于正常范围内, 没有需要规律透析的。中位术后住院时间为4 d(3~7 d), 术后病理检查报告所有标本均为肾细胞癌, 切缘都为阴性。术后中位随访时间为7个月, 最短达到3个月, 最长者为42个月。
后腹腔镜肾部分切除术与经腹腔途径相比, 国内应用更广泛, 两种方式在手术时间、失血量、并发症方面的差异无统计学意义, 但经腹腔途径在操作空间和解剖标志方面有明显优势, 而后腹腔途径则在对腹内脏器的影响和术后恢复方面有优势。欧美患者肥胖较多, 通常更为推荐经腹腔途径, 但是对于体型偏瘦小的中国患者来说, 通常后腹腔入路更有优势。后腹腔入路也有其缺点:操作空间相对狭窄, 没有明确的解剖标志, 对于腹侧、肾门区、肾下极的肾肿瘤难以得到较好的暴露和操作角度。肾蒂旋转法能够较好地解决经腹膜后途径暴露的问题, 保证肿瘤的切除和残肾的缝合能有较好的操作角度。
有研究者提出肾蒂旋转法的主要注意事项, 如术前血管CT成像、充分游离、术中B超定位、恰当的缝合深度[19], 有研究者扩大了研究数量, 同时提到对于腹侧尤其是肾门区复杂性肾肿瘤行肾部分切除术, 对术者的技术要求较高, 但进一步证实了该方法安全有效[20, 21, 22]。宋健等[23]在其对腹侧肾门区肾肿瘤的肾部分切除术中也应用到了肾蒂旋转技术, 并建议由远离肾血管方向切开肾实质以保证肿瘤安全、完整地切除, 而俞鸿凯等[24]建议由肾门前后唇肿瘤基底部及其周围肾窦组织与肾血管或集尿系统之间的层面开始解剖, 由于肾蒂血管及集合系统与肾窦脂肪之间的天然解剖层面的存在, 使这种入路能最大限度地减少对肾血管及集合系统的损伤。在实际应用中应根据具体情况进行选择, 若肿瘤与肾血管关系较紧密则优先选择近血管方向沿解剖层面切除肿瘤, 若肿瘤位于下极或靠外侧, 损伤血管及集合系统可能性较小, 则从远血管方向进行切开。缝合方面由最初的间断8字缝合到连续缝合加Hem-o-lok夹再发展到倒刺线缝合, 有研究者设计了新型钳夹缝线线夹, 避免松脱导致出血[25, 26]。26例中9例应用了后腹腔镜下旋转法辅助肾部分切除术, 切缘均为阴性, 平均热缺血时间为31 min, 进一步证实了该方法的安全性和有效性。门昌平等[27]对肾门旁肿瘤肾部分切除术的经腹途径及腹膜后途径进行了对比, 肾蒂旋转法在腹膜后途径可减少手术时间, 得到更好的切除和缝合角度, 同时在肠道恢复方面腹膜后途径有明显优势。
在腹侧肾肿瘤的肾部分切除术中该技术得到大量的应用, 并被总结和归纳, 在腹侧或肾下极的保留肾单位手术中, 将肾和肾蒂完全游离, 阻断肾动脉, 必要时阻断静脉。将肾旋转一定的角度, 使肾肿瘤暴露在术野内, 变操作死角为合适的位置。旋转的角度和方向并不固定, 应该按照肿瘤的位置进行调整。通常情况下, 对于腹侧肾下极的肿瘤应使下极向背侧、上极向腹侧旋转, 上极的肿瘤应使肾下极向腹侧、上极向背侧旋转, 肾门区的复杂肾肿瘤较肾下极肿瘤而言旋转角度更小。缝合完成后必须将肾复位, 避免同方向旋转导致血管损伤。复位后将肾与周围肌肉缝合以固定。
肾蒂旋转法能够减少后腹腔入路带来的操作死角, 使肿瘤的切除和残肾的缝合更为方便, 同时减少热缺血时间[28], 而减少热缺血时间对保护肾功能非常重要[28, 29, 30, 31, 32, 33]。通常肾门区肾肿瘤的肾部分切除术对外科医生来说难度较高, 将该研究结果与国内外相关研究进行比较[6, 7, 8, 9, 10, 11, 12, 13], 对于腹侧肾肿瘤的肾部分切除术, 国外经腹腔途径更多见, 而国内更常用经腹膜后途径; 本研究中手术患者平均肿瘤大小相对较大, 而耗费手术时间最短, 热缺血时间及估计出血量较少, 术后无一例切缘阳性, 并发症发生率居中; 在上述相关文献中, 肾蒂旋转法配合经腹膜后途径与经腹腔途径的手术对比中, 各指标未见明显劣势, 且在手术时间、估计出血量方面有明显优势, 可以认为肾蒂旋转法辅助治疗后腹腔镜下腹侧肾肿瘤的肾部分切除术是安全可靠的。
该研究有如下几点不足, 首先这项研究仅仅是单中心回顾性分析; 其次由于重点关注了腹侧肾肿瘤患者, 导致患者数量及随访时间都略有不足; 再次, 由于所有手术均由腹膜后入路完成, 未建立经腹腔途径的对照组, 在手术效果、并发症、手术时间、手术难度等方面无法与经腹腔途径的手术比较, 因此, 下一步需要进行大样本多中心的研究, 以及更长时间的随访。
该研究中28例患者手术效果提示, 对于腹侧肾肿瘤, 特别是肾门区、肾下极的肿瘤, 利用肾蒂旋转法行肾部分切除术是可行并有效的, 短期内肾功能及肿瘤切除均能达到满意疗效, 但长远效果仍有待继续随访。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|