Journal of Peking University(Health Sciences) ›› 2019, Vol. 51 ›› Issue (5): 977-980. doi: 10.19723/j.issn.1671-167X.2019.05.032
Previous Articles Next Articles
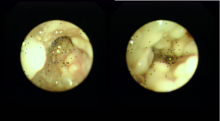
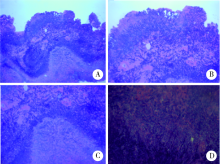
Drug-induced toxic epidermal necrolysis with secondary aspergillus fumigatus infection: a case report
Si ZHANG,Xiao-yang LIU,Jian-zhong ZHANG( ),Lin CAI,Cheng ZHOU()
),Lin CAI,Cheng ZHOU()
- Department of Dermatological, Peking University People’s Hospital, Beijing 100044, China
CLC Number:
- R758.25






| [1] | Mazokopakis EE, Tzortzinis AA, Dalieraki-Ott EI , et al. Coexistence of Hashimoto’s thyroiditis with papillary thyroid carcinoma.a retrospective study[J]. Hormones (Athens), 2010,9(5):312-317. |
| [2] | Pazos C, Ponton J, Del Palaeio A . Contribution of (1,3)-beta-D-glucanchromogenie assay to diagnosis and therapeutic monitoring of invasive aspergillosis in neutropenia adult patients:a comparison with serial screening for circulating galactomannan[J]. J Clin Microbiol, 2005,43:299-305. |
| [3] | 黄晓鸥, 刘霆 . 联合检测半乳甘露聚糖和(1,3)-β- D葡聚糖诊断侵袭性曲霉菌感染的研究进展[J]. 中国呼吸与危重监护杂志, 2011,10(6):610-612. |
| [4] | Bohme A, Ruhnke M, Buehheidt D , et al. Treatment of invasive fungal infections in cancer patients-recommendations of the infectious diseases working party (AGlHO) of the German Society of Hematology and Oncology (DGHO)[J]. Ann Hematol, 2009,88(2):97-110. |
| [5] | Herbrecht R, Denning DW, Patterson TF , et al. Voriconazole versus amphotericin B for invasive aspergillosis.[J]. New Engl J Med, 2002,347(25):2080-2081. |
| [6] | Paradisi A, Abeni D, Bergamo F , et al. Etanercept therapy for toxic epidermal necrolysis[J]. J Am Acad Dermatol, 2014,71(2):278-283. |
| [7] | Espinel-Ingroff A, Cuenca-Estreila M, Fothergill A , et al. Wild-type MIC distributions and epidemiological cutoff values for amphotericin B and Aspergillus spp.for the CLSI broth microdilution method (M38-A2 document)[J]. Antimicrob Agents Chemother, 2011,55(11):5150-5154. |
| [8] | Lockhart SR, Frade JP, Etienne KA , et al. Azole resistance in Aspergillus fumigatus isolates from the ARTEMIS global surveillance is primarily due to the TR/L98H mutation in the cyp51A gene[J]. Antimicrob Agents Chemother, 2011,55(9):4465-4468. |
| [9] | Harr T, French LE . Toxic epidermal necrolysis and Stevens-Johnson syndrome[J]. Arch Dermatol, 2000,136(3):323-327. |
| [1] | Yunling GENG, Chao LIU, Ping YANG, Jiajia ZHENG, Ning SHEN, Yipeng DU. Clinical features and virulence gene distribution of Klebsiella pneumoniae multi-site infection in patients with hospital-acquired pneumonia [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 201-207. |
| [2] | Ziwei WANG, Min LI, Hui GAO, Fang DENG. Correlation between streptococcal infection and renal damage in children with Henoch-Schönlein purpura nephritis [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 284-290. |
| [3] | Aichun LIU, Huiping ZHAO, Bei WU, Shuying ZHENG, Li ZUO, Mei WANG. Bacterial biofilm formation of peritoneal dialysis catheter in patients with peritonitis-associated catheter removal [J]. Journal of Peking University (Health Sciences), 2025, 57(1): 161-165. |
| [4] | Li-fang WANG,Lian-jie SHI,Wu NING,Nai-shu GAO,Kuan-ting WANG. Sjögren's syndrome combined with cold agglutinin disease: A case report [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1130-1134. |
| [5] | Jie QIAO,Li-xia LU,Yu-ting HE,Chun-cui MEN,Xin-xin CHU,Bei WU,Hui-ping ZHAO,Mei WANG. Fungal peritoneal dialysis catheter-related exit-site infection combined with tunnel infection: A case report [J]. Journal of Peking University (Health Sciences), 2023, 55(4): 748-754. |
| [6] | Hao LIN,Jing-hua LI,Xiao YANG,Xiao-ting CHEN,Yu-hui SHI,Chun CHANG,Yuan-tao HAO,Wang-nan CAO. Discrepancy between behavioral-indicated and perceived candidacy for HIV pre-exposure prophylaxis among men who have sex with men in Chengdu, China [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 511-520. |
| [7] | Zhe WANG,Wei SUN,Xue YANG,Ying SONG,Ai-ping JI,Jie BAI. Clinical analysis of patients with oral and maxillofacial infections in oral emergency [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 543-547. |
| [8] | Yi-lin YE,Heng LIU,Li-ping PAN,Wei-bing CHAI. Periprosthetic gout flare after total knee arthroplasty: A misdiagnostic case report [J]. Journal of Peking University (Health Sciences), 2023, 55(2): 362-365. |
| [9] | Fang CAO,Ming ZHONG,Cong-rong LIU. Uterine POLE mutant endometrioid carcinoma combined with human papilloma virus-associated cervical adenocarcinoma: A case report and literature review [J]. Journal of Peking University (Health Sciences), 2023, 55(2): 370-374. |
| [10] | Xiao-yan XING,Jun-xiao ZHANG,Feng-yun-zhi ZHU,Yi-fan WANG,Xin-yao ZHOU,Yu-hui LI. Clinical analysis of 5 cases of dermatomyositis complicated with macrophage activation syndrome [J]. Journal of Peking University (Health Sciences), 2022, 54(6): 1214-1218. |
| [11] | Zhi-yu KANG,Lei-lei WANG,Yong-zheng HAN,Xiang-yang GUO. Anesthesia management of athletes' operation in Beijing Olympic Winter Games [J]. Journal of Peking University (Health Sciences), 2022, 54(4): 770-773. |
| [12] | ZHANG Pu-li,YANG Hong-xia,ZHANG Li-ning,GE Yong-peng,PENG Qing-lin,WANG Guo-chun,LU Xin. Value of serum YKL-40 in the diagnosis of anti-MDA5-positive patients with dermatomyositis complicated with severe pulmonary injury [J]. Journal of Peking University (Health Sciences), 2021, 53(6): 1055-1060. |
| [13] | Hong MENG,Li-na JI,Jing HUANG,Shuang CHAO,Jia-wen ZHOU,Xue-jun LI,Xiao-mei YIN,Li-rong FAN. Analysis of the changes and characteristics of pediatric outpatient visits in a general hospital in Beijing before and after the COVID-19 pandemic [J]. Journal of Peking University (Health Sciences), 2021, 53(5): 952-956. |
| [14] | DU Qiang,HONG Kai,PAN Bo-chen. Comparison of two methods for detection of Chlamydia trachomatis and Ureaplasma urealyticum in male reproductive tract [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 785-788. |
| [15] | ZHOU Bo-lin,LI Wei-shi,SUN Chui-guo,QI Qiang,CHEN Zhong-qiang,ZENG Yan. Risk factors for multiple debridements of the patients with deep incisional surgical site infection after spinal surgery [J]. Journal of Peking University (Health Sciences), 2021, 53(2): 286-292. |
|
||