Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (6): 1088-1093. doi: 10.19723/j.issn.1671-167X.2021.06.014
Previous Articles Next Articles
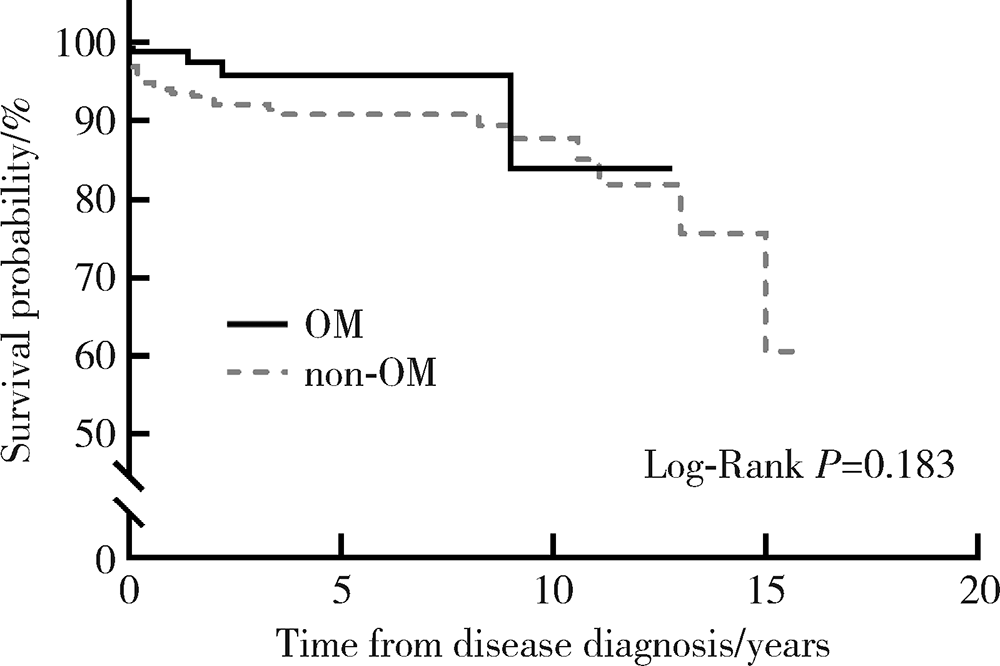
Clinical and immunological characteristics of 88 cases of overlap myositis
XIAO Yun-shu1,ZHU Feng-yun-zhi2,LUO Lan2,XING Xiao-yan2,LI Yu-hui2,△( ),ZHANG Xue-wu2,SHEN Dan-hua1
),ZHANG Xue-wu2,SHEN Dan-hua1
- 1. Department of Pathology, Peking University People’s Hospital, Beijing 100044, China
2. Department of Rheumatology and Immunology, Peking University People’s Hospital, Beijing 100044, China
CLC Number:
- R593.26

| [1] |
Lilleker JB, Vencovsky J, Wang G, et al. The EuroMyositis registry: an international collaborative tool to facilitate myositis research[J]. Ann Rheum Dis, 2018, 77(1):30-39.
doi: 10.1136/annrheumdis-2017-211868 pmid: 28855174 |
| [2] |
Aguila LA, Lopes MR, Pretti FZ, et al. Clinical and laboratory features of overlap syndromes of idiopathic inflammatory myopathies associated with systemic lupus erythematosus, systemic sclerosis, or rheumatoid arthritis[J]. Clin Rheumatol, 2014, 33(8):1093-1098.
doi: 10.1007/s10067-014-2730-z |
| [3] |
Nuño-Nuño L, Joven BE, Carreira PE, et al. Overlap myositis, a distinct entity beyond primary inflammatory myositis: a retrospective analysis of a large cohort from the REMICAM registry[J]. Int J Rheum Dis, 2019, 22(8):1393-1401.
doi: 10.1111/1756-185X.13559 pmid: 30968571 |
| [4] |
Lundberg IE, Tjärnlund A, Bottai M, et al. EULAR/ACR Classification Criteria for Adult and Juvenile Idiopathic Inflammatory Myopathies and their Major Subgroups[J]. Arthritis Rheumatol, 2017, 69(12):2271-2282.
doi: 10.1002/art.40320 |
| [5] | Dalakas MC. Polymyositis, dermatomyositis and inclusion-body myositis[J]. N Engl J Med, 1991, 325(21):1487-1498. |
| [6] |
van den Hoogen F, Khanna D, Fransen J, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League Against Rheumatism Collaborative Initiative[J]. Arthritis Rheum, 2013, 65(11):2737-2747.
doi: 10.1002/art.38098 |
| [7] |
Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism Collaborative Initiative[J]. Arthritis Rheum, 2010, 62(9):2569-2581.
doi: 10.1002/art.27584 |
| [8] |
VitaliC, Bombardiefi S, Josson R, et al. Classification criteria for Sjögren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group[J]. Ann Rheum Dis, 2002, 61(6):554-558.
pmid: 12006334 |
| [9] |
Aringer M, Costenbader K, Daikh D, et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus[J]. Arthritis Rheumatol, 2019, 71(9):1400-1412.
doi: 10.1002/art.40930 |
| [10] |
Solomon J, Swigris JJ, Brown KK. Myositis-related interstitial lung disease and antisynthetase syndrome[J]. J Bras Pneumol, 2011, 37(1):100-109.
doi: S1806-37132011000100015 pmid: 21390438 |
| [11] |
Chinniah KJ, Mody GM. The spectrum of idiopathic inflammatory myopathies in South Africa[J]. Clinical rheumatology, 2020, 40(4):1437-1446.
doi: 10.1007/s10067-020-05048-w |
| [12] |
Troyanov Y, Targoff IN, Tremblay JL, et al. Novel classification of idiopathic inflammatory myopathies based on overlap syndrome features and autoantibodies: analysis of 100 French Canadian patients[J]. Medicine (Baltimore), 2005, 84(4):231-249.
doi: 10.1097/01.md.0000173991.74008.b0 |
| [13] |
Cobo-Ibáñez T, López-Longo FJ, Joven B, et al. Long-term pulmonary outcomes and mortality in idiopathic inflammatory myopathies associated with interstitial lung disease[J]. Clinical Rheumatology, 2019, 38(3):803-815.
doi: 10.1007/s10067-018-4353-2 pmid: 30392161 |
| [14] |
Zhang L, Wu G, Gao D, et al. Factors associated with interstitial lung disease in patients with polymyositis and dermatomyositis: a systematic review and meta-analysis[J]. PLoS One, 2016, 11(5):e0155381.
doi: 10.1371/journal.pone.0155381 |
| [15] |
Keser G, Capar I, Aksu K, et al. Pulmonary hypertension in rheumatoid arthritis[J]. Scand J Rheumatol, 2004, 33(4):244-245.
pmid: 15370720 |
| [16] | Kobak S, Kalkan S, Bahadır Kirilmaz, et al. Pulmonary arterial hypertension in patients with primary Sjögren’s syndrome[J]. Autoimmune diseases, 2014, 2014:710401. |
| [17] |
Sanges S, Yelnik CM, Sitbon O, et al. Pulmonary arterial hypertension in idiopathic inflammatory myopathies: data from the French pulmonary hypertension registry and review of the literature[J]. Medicine (Baltimore), 2016, 95(39):e4911.
doi: 10.1097/MD.0000000000004911 |
| [18] |
Barba T, Mainbourg S, Nasser M, et al. Lung diseases in inflammatory myopathies[J]. Semin Respir Crit Care Med, 2019, 40(2):255-270.
doi: 10.1055/s-0039-1685187 |
| [19] |
Condliffe R, Howard L. Connective tissue disease-associated pulmonary arterial hypertension[J]. F1000Prime Reports, 2015, 7:6.
doi: 10.12703/P7-06 pmid: 25705389 |
| [20] |
Aithala R, Alex AG, Danda D. Pulmonary hypertension in connective tissue diseases: an update[J]. Int J Rheum Dis, 2017, 20(1):5-24.
doi: 10.1111/1756-185X.13001 pmid: 28205373 |
| [21] |
Albrecht K, Huscher D, Callhoff J, et al. Trends in idiopathic inflammatory myopathies: cross-sectional data from the German National Database[J]. Rheumatol Int, 2020, 40(10):1639-1647.
doi: 10.1007/s00296-020-04634-0 pmid: 32594219 |
| [22] |
Ruiz-Cano MJ, Escribano P, Alonso R, et al. Comparison of baseline characteristics and survival between patients with idiopathic and connective tissue disease-related pulmonary arterial hypertension[J]. J Heart Lung Transplant, 2009, 28(6):621-627.
doi: 10.1016/j.healun.2009.02.016 |
| [23] |
Jayakumar D, Zhang R, Wasserman A, et al. Cardiac manifestations in idiopathic inflammatory myopathies: an overview[J]. Cardiol Rev, 2019, 27(3):131-137.
doi: 10.1097/CRD.0000000000000241 pmid: 30585794 |
| [24] |
Gupta R, Wayangankar SA, Targoff IN, et al. Clinical cardiac involvement in idiopathic inflammatory myopathies: a systematic review[J]. Int J Cardiol, 2011, 148(3):261-270.
doi: 10.1016/j.ijcard.2010.08.013 |
| [25] |
Danieli MG, Gambini S, Pettinari L, et al. Impact of treatment on survival in polymyositis and dermatomyositis. A single-centre long-term follow-up study[J]. Autoimmun Rev, 2014, 13(10):1048-1054.
doi: 10.1016/j.autrev.2014.08.023 |
| [26] | Lundberg IE. The heart in dermatomyositis and polymyositis[J]. Rheumatology (Oxford), 2006, 45(Suppl 4):18-21. |
| [27] |
Lu Z, Guo-Chun W, Li M, et al. Cardiac involvement in adult polymyositis or dermatomyositis: a systematic review[J]. Clin Cardiol, 2012, 35(11):685-691.
doi: 10.1002/clc.v35.11 |
| [28] |
Iaccarino L, Gatto M, Bettio S, et al. Overlap connective tissue disease syndromes[J]. Autoimmun Rev, 2013, 12(3):363-373.
doi: 10.1016/j.autrev.2012.06.004 pmid: 22743033 |
| [29] |
Betteridge Z, Tansley S, Shaddick G, et al. Frequency, mutual exclusivity and clinical associations of myositis autoantibodies in a combined European cohort of idiopathic inflammatory myopathy patients[J]. J Autoimmun, 2019, 101:48-55.
doi: S0896-8411(19)30100-3 pmid: 30992170 |
| [30] |
Rigolet A, Musset L, Dubourg O, et al. Inflammatory myopathies with anti-Ku antibodies: a prognosis dependent on associated lung disease[J]. Medicine (Baltimore), 2012, 91(2):95-102.
doi: 10.1097/MD.0b013e31824d9cec |
| [31] |
Maundrell A, Proudman S, Limaye V. Prevalence of other connective tissue diseases in idiopathic inflammatory myopathies[J]. Rheumatol Int, 2019, 39(10):1777-1781.
doi: 10.1007/s00296-019-04411-8 pmid: 31385080 |
| [32] |
Ng KP, Ramos F, Sultan SM, et al. Concomitant diseases in a cohort of patients with idiopathic myositis during long-term follow-up[J]. Clin Rheumatol, 2009, 28(8):947-953.
doi: 10.1007/s10067-009-1181-4 pmid: 19387765 |
| [33] |
Torres C, Belmonte R, Carmona L, et al. Survival, mortality and causes of death in inflammatory myopathies[J]. Autoimmunity, 2006, 39(3):205-215.
doi: 10.1080/08916930600622603 |
| [34] |
Amaral Silva M, Cogollo E, Isenberg DA. Why do patients with myositis die? A retrospective analysis of a single-centre cohort[J]. Clin Exp Rheumatol, 2016, 34(5):820-826.
pmid: 27494511 |
| [1] | Zhengfang LI,Cainan LUO,Lijun WU,Xue WU,Xinyan MENG,Xiaomei CHEN,Yamei SHI,Yan ZHONG. Application value of anti-carbamylated protein antibody in the diagnosis of rheumatoid arthritis [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 729-734. |
| [2] | Zhanhong LAI,Jiachen LI,Zelin YUN,Yonggang ZHANG,Hao ZHANG,Xiaoyan XING,Miao SHAO,Yuebo JIN,Naidi WANG,Yimin LI,Yuhui LI,Zhanguo LI. A unicenter real-world study of the correlation factors for complete clinical response in idiopathic inflammatory myopathies [J]. Journal of Peking University (Health Sciences), 2024, 56(2): 284-292. |
| [3] | Yan-hong MENG,Yi-fan CHEN,Pei-ru ZHOU. Clinical and immunological features of primary Sjögren's syndrome patients with positive anti-centromere protein B antibody [J]. Journal of Peking University (Health Sciences), 2023, 55(6): 1088-1096. |
| [4] | Xiao-yan XING,Jun-xiao ZHANG,Feng-yun-zhi ZHU,Yi-fan WANG,Xin-yao ZHOU,Yu-hui LI. Clinical analysis of 5 cases of dermatomyositis complicated with macrophage activation syndrome [J]. Journal of Peking University (Health Sciences), 2022, 54(6): 1214-1218. |
| [5] | Lu ZHANG,Cheng CHEN,Mei-ting WENG,Ai-ping ZHENG,Mei-ling SU,Qing-wen WANG,Yue-ming CAI. Characteristics of serum autoantibodies in patients with lupus nephritis and tubulointerstitial damage [J]. Journal of Peking University (Health Sciences), 2022, 54(6): 1094-1098. |
| [6] | YI Wen-xia,WEI Cui-jie,WU Ye,BAO Xin-hua,XIONG Hui,CHANG Xing-zhi. Long-term rituximab treatment of refractory idiopathic inflammatory myopathy: A report of 3 cases [J]. Journal of Peking University (Health Sciences), 2021, 53(6): 1191-1195. |
| [7] | LUO Lan,XING Xiao-yan,XIAO Yun-shu,CHEN Ke-yan,ZHU Feng-yun-zhi,ZHANG Xue-wu,LI Yu-hui. Clinical and immunological characteristics of patients with anti-synthetase syndrome complicated with cardiac involvement [J]. Journal of Peking University (Health Sciences), 2021, 53(6): 1078-1082. |
| [8] | Feng-yun-zhi ZHU,Xiao-yan XING,Xiao-fei TANG,Yi-min LI,Miao SHAO,Xue-Wu ZHANG,Yu-hui LI,Xiao-lin SUN,Jing HE. Clinical and immunological characteristics of myositis complicated with thromboembolism [J]. Journal of Peking University (Health Sciences), 2020, 52(6): 995-1000. |
| [9] | Yi-ming ZHENG,Hong-jun HAO,Yi-lin LIU,Jing GUO,Ya-wen ZHAO,Wei ZHANG,Yun YUAN. Correlation study on anti-Ro52 antibodies frequently co-occur with other myositis-specific and myositis-associated autoantibodies [J]. Journal of Peking University (Health Sciences), 2020, 52(6): 1088-1092. |
| [10] | Jing ZHAO,Feng SUN,Yun LI,Xiao-zhen ZHAO,Dan XU,Ying-ni LI,Yu-hui LI,Xiao-lin SUN. Significance of anti-tubulin-α-1C autoantibody in systemic sclerosis [J]. Journal of Peking University (Health Sciences), 2020, 52(6): 1009-1013. |
| [11] | LIU Xue-qin, YAN Hui, QIU Jian-xing, ZHANG Chun-yu, QI Jian-guang, ZHANG Xin, XIAO Hui-jie, YANG Yan-ling, CHEN Yong-hong, DU Jun-bao. Pulmonary arterial hypertension as leading manifestation of methylmalonic aciduria: clinical characteristics and gene testing in 15 cases [J]. Journal of Peking University(Health Sciences), 2017, 49(5): 768-777. |
| [12] | XU Jing, LIU Jing,ZHU Lei, ZHANG Xue-wu, LI Zhan-guo. Significance of glucose-6-phosphate isomerase assay in early diagnosis of rheumatoid arthritis [J]. Journal of Peking University(Health Sciences), 2016, 48(6): 942-946. |
| [13] | WANG Lin-Lin, YANG Na, YUAN Yue, REN Ai-Guo. Establishment and evaluation of enzyme-linked immunosorbent assay for measuring human autoantibody IgG to folate receptor [J]. Journal of Peking University(Health Sciences), 2014, 46(3): 483-487. |
| [14] | LIU Yuan, WANG Yong-Fu, WANG Kai-Li, 吕Feng-Feng . Prevalence and significance of immunoglobulin G-anti-cyclic citrullinated peptide antibodies in primary Sjögren’s syndrome patients [J]. Journal of Peking University(Health Sciences), 2014, 46(3): 478-482. |
|
||