Journal of Peking University(Health Sciences) ›› 2019, Vol. 51 ›› Issue (6): 1169-1172. doi: 10.19723/j.issn.1671-167X.2019.06.034
Previous Articles Next Articles
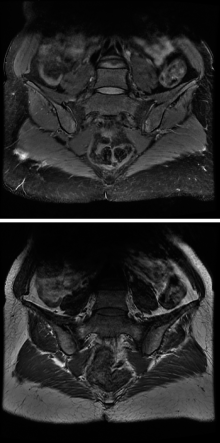
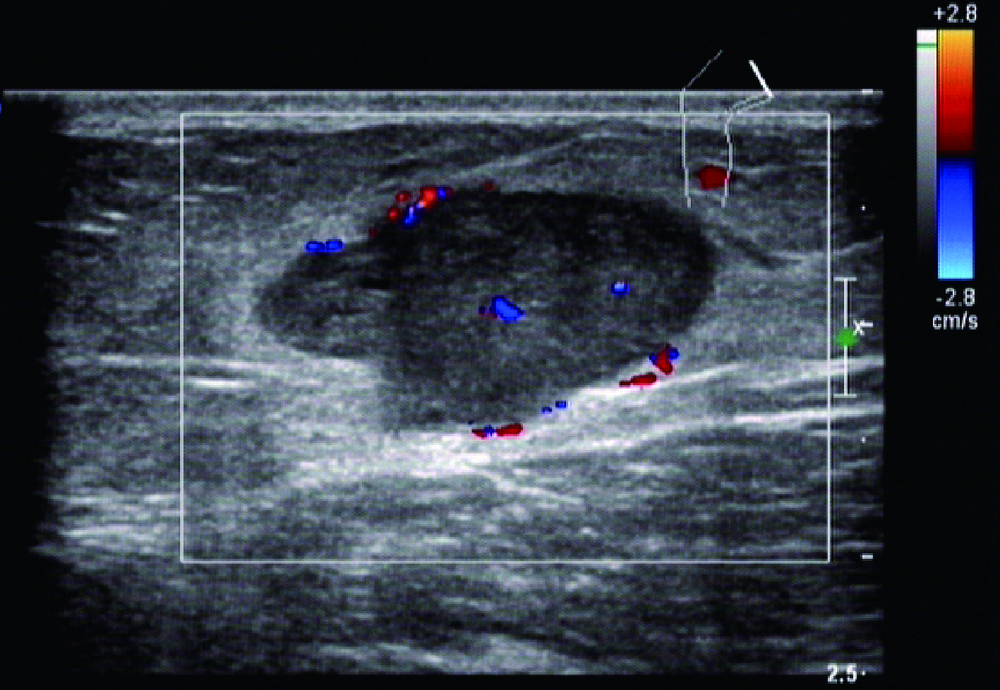
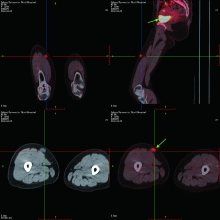
Hypophosphatemic osteomalacia caused by urinary mesenchymal tumor: A case
Hui WEI,Rui LIU( ),Zhan-hui WANG,Zhong-qiang YAO
),Zhan-hui WANG,Zhong-qiang YAO
- Department of Rheumatology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R591.44


| [1] | 唐宏宇, 王海彬, 何伟 , 等. 髋部磷酸盐尿性间叶瘤致全身低磷性骨软化症4例[J]. 中华关节外科杂志: 电子版, 2018,12(5):727-729. |
| [2] | Chong WH, Molinolo AA, Chen CC , et al. Tumor-induced osteomalacia[J]. Endocr Relat Cancer, 2011,18(3):R53-R77. |
| [3] | Bergwitz C, Collins MT, Kamth RS , et al. Case records of the Massachusetts General Hospital. Case 33-2011. A 56-year-old man with hypophosphatemia[J]. N Engl J Med, 2011,365(17):1625-1635. |
| [4] | 许志阳, 张文明 . 踝部肿瘤诱发低磷性骨软化症1例[J]. 中华骨质疏松和骨矿盐疾病杂志, 2018,11(6):584-587. |
| [5] | 李晔, 高鹏 . 距骨肿瘤相关性低磷抗D骨软化症1例报告[J]. 中国骨与关节外科, 2011,4(1):81-83. |
| [6] |
巴建明, 桑艳红, 陆菊明 , 等. 12例肿瘤性骨软化症的临床诊治及术后随访[J]. 中华内分泌代谢杂志, 2011,27(1):19-23.
doi: 10.3760/cma.j.issn.1000-6699.2011.01.007 |
| [7] | 张化冰, 潘慧, 李方 , 等. 奥曲肽显像诊断肿瘤性骨软化症一例[J]. 中华医学杂志, 2005,85(33):2375-2376. |
| [8] | Cliflon-Bligh RJ, Hofman MS, Duncan E , et al. Improving diagnosis of tumor-induced osteomalacia with Gallium-68 DATATATE PET/CT[J]. J Clin Endocrinol Metab, 2013,98(2):687-694. |
| [9] | Agrawal K, Bhadada S, Mittal BR , et al. Comparison of 18F-FDG and 68Ga DOTATATE PET/CT in localization of tumor causing oncogenic osteomalacia [J]. Clin Nucl Med, 2015,40(1):e6-e10. |
| [10] | 魏伟平, 刘海蔚, 全会标 , 等. 肿瘤性低磷骨软化症一例报道并文献复习[J]. 中国全科医学, 2018,21(13):1629-1632. |
| [11] | 金今, 邱贵兴, 陈宾 , 等. 肿瘤相关性低磷抗D骨软化症的外科干预治疗[J]. 中国骨质疏松杂志, 2005,8(3):346-348. |
| [12] | Areses-Trapote R, Lopez-Garcia JA, Ubetagoyena-Arrieta M , et al. Hereditary hypophosphatemic rickets with hypercalciuria: case reports[J]. Nefrologia, 2012,32(4):529-534. |
| [13] | Wang H, Zhang D, Liu Y , et al. Surgical treatments of tumor-induced osteomalacia lesions in long bones: seventeen cases with more than one year of follow-up[J]. J Bone Joint Surg Am, 2015,97(13):1084-1094. |
| [14] | Geller JL, Khoseavi A, Kelly MH , et al. Cinacalcet in the ma-nagement of tumor-induced osteomalacia[J]. Bone Miner Res, 2007,22(6):931-937. |
| [15] | Paglia F, Dionisi S, Minisola S . Octreotide for tumor-induced osteomalacia[J]. N Engl J Med, 2002,346(22):1748-1749. |
| [16] | Fukumoto S . Anti-fibroblast growth factor 23 antibody therapy[J]. Curr Opin Nephrol Hypertens, 2014,23(4):346-351. |
| [17] | Hesse E, Rosenthal H, Bastian L . Radiofrequency ablation of a tumor causing oncogenic osteomalacia[J]. N Engl J Med, 2007,357(4):422-424. |
| [1] | Wen SUN,Ang LI,Jun-qing ZHANG,Zhen-fang YUAN. Low-dose adefovir-induced Fanconi syndrome and hypophosphatemic osteomalacia: A case report and literature review [J]. Journal of Peking University (Health Sciences), 2020, 52(5): 975-979. |
|
||