Journal of Peking University(Health Sciences) ›› 2019, Vol. 51 ›› Issue (6): 1165-1168. doi: 10.19723/j.issn.1671-167X.2019.06.033
Previous Articles Next Articles
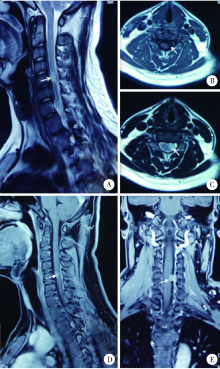
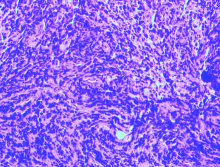
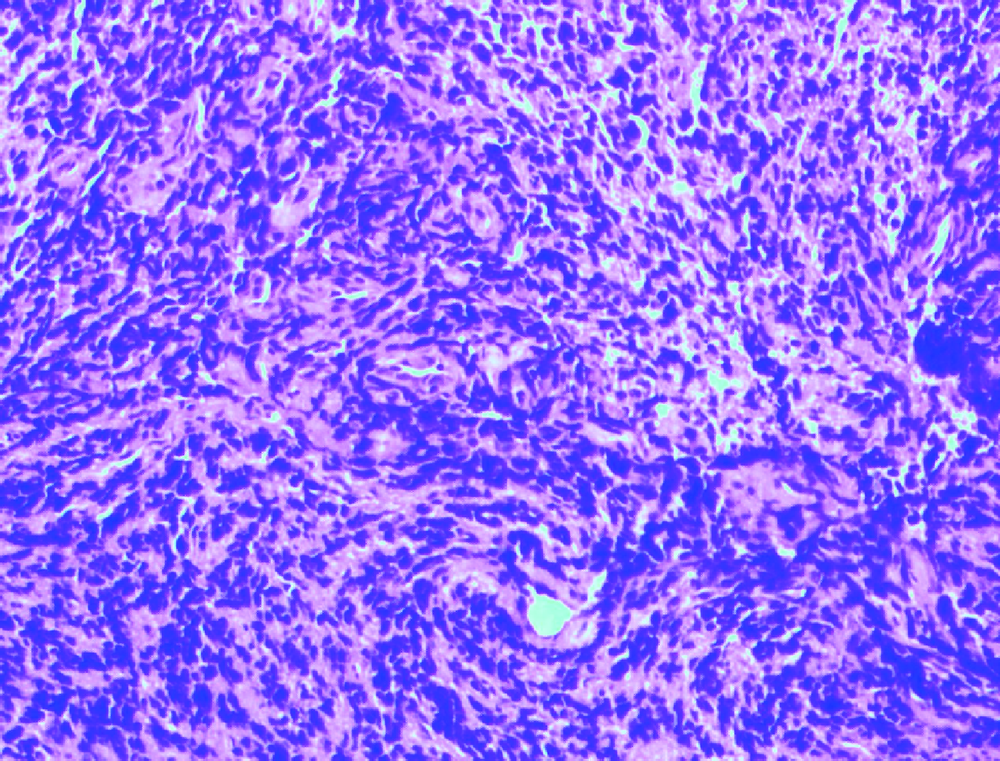
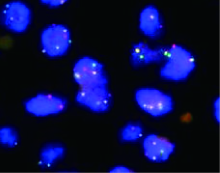
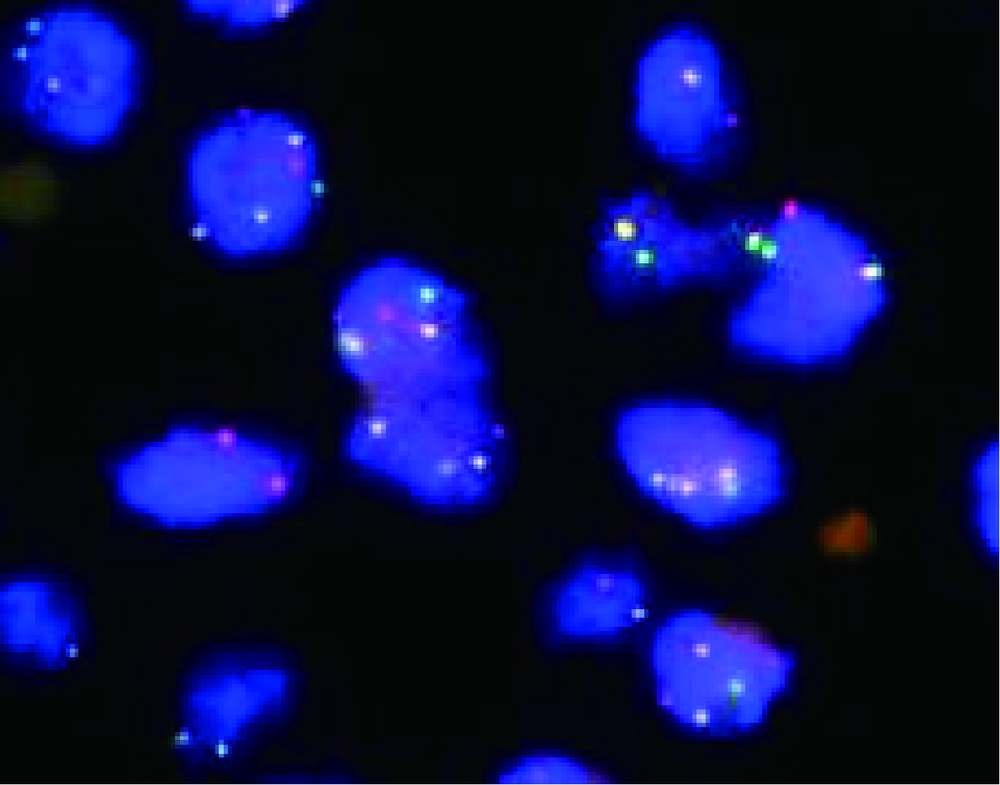
Intraspinal metastasis of alveolar rhabdomyosarcoma: A case report
Guo-zhong LIN,Zhen-yu WANG1,△( ),Bin LIU1,Shao-min YANG2
),Bin LIU1,Shao-min YANG2
- 1. Department of Neurosurgery, Peking University Third Hospital, Beijing 100191, China
2. Department of Pathology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R739.4







| [1] | Paulino AC, Okcu MF . Rhabdomyosarcoma[J]. Curr Probl Can-cer, 2008,32(1):7-34. |
| [2] | Egas-Bejar D, Huh WW . Rhabdomyosarcoma in adolescent and young adult patients: current perspectives[J]. Adolesc Health Med Ther, 2014,5:115-125. |
| [3] | Parham DM, Barr FG . Classification of rhabdomyosarcoma and its molecular basis[J]. Adv Anat Pathol, 2013,20(6):387-397. |
| [4] | Fletcher CD . The evolving classification of soft tissue tumours:an update based on the new 2013 WHO classification[J]. Histopathology, 2013,64(1):2-11. |
| [5] | Sarkar D, Ray S, Saha M , et al. Alveolar rhabdomyosarcoma with multiple distal metastases. A case report and review of literature[J]. BMJ Case Rep, 2012,2012(968):382. |
| [6] | Eftekhari K, Chambers CB, Goldstein SM , et al. Alveolar rhabdomyosarcoma masquerading as embryonal subtype: the value of modern molecular diagnostic testing[J]. Ophthal Plast Reconstr Surg, 2015,31(2):e43-e45. |
| [7] | La Starza R, Nofrini V, Pierini T , et al. Molecular cytogenetics detect an unbalanced t(2;13)(q36;q14) and PAX3-FOXO1 fusion in rhabdomyosarcoma with mixed embryonal/alveolar features[J]. Pediatr Blood Cancer, 2015,62(12):2238-2241. |
| [8] | Mercado GE, Barr FG . Fusions involving PAX and FOX genes in the molecular pathogenesis of alveolar rhabdomyosarcoma: recent advances[J]. Curr Mol Med, 2007,7(1):47-61. |
| [9] | Sullivan LM, Atkins KA, LeGallo RD . PAX immunoreactivity identifies alveolar rhabdomyosarcoma[J]. Am J Surg Pathol, 2009,33(5):775-780. |
| [1] | YE Jian-fei,ZHAO Lei,WANG Guo-liang,HONG Kai,MA Lu-lin. Clinical analysis of testicular rhabdomyosarcoma [J]. Journal of Peking University (Health Sciences), 2021, 53(6): 1178-1182. |
|
||