Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (6): 1178-1182. doi: 10.19723/j.issn.1671-167X.2021.06.028
Previous Articles Next Articles
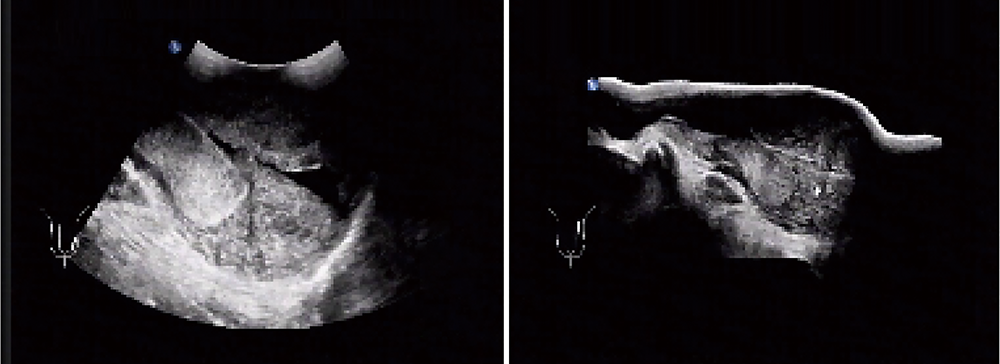
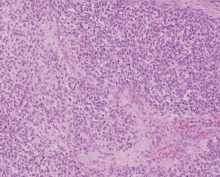
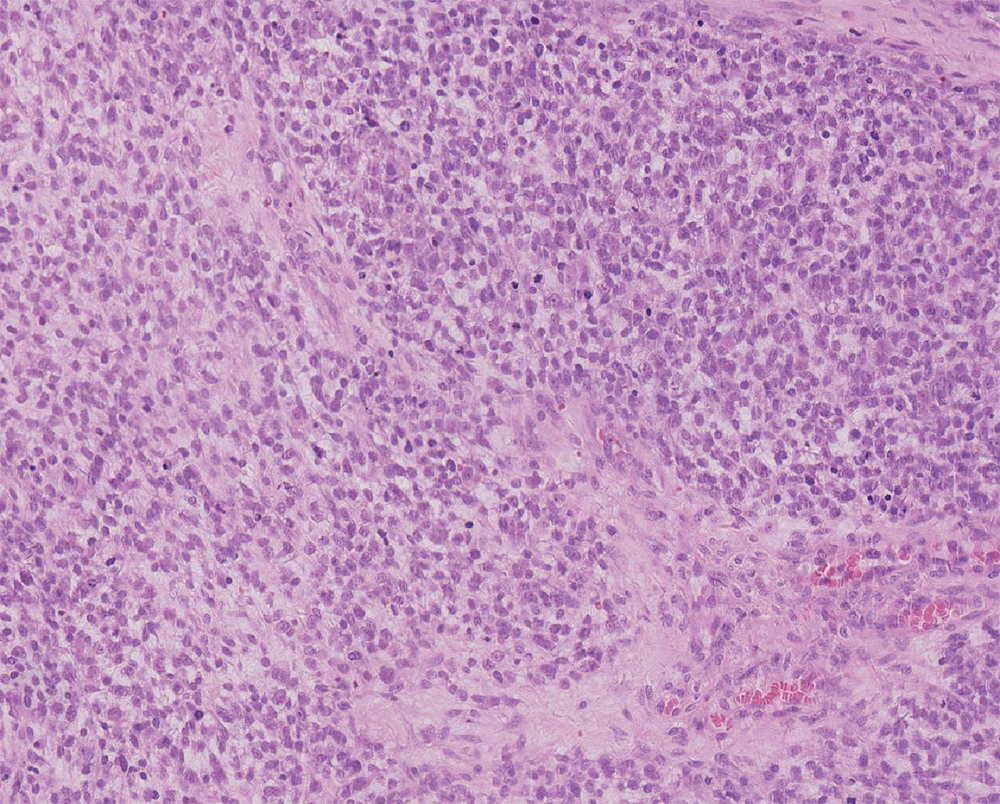
Clinical analysis of testicular rhabdomyosarcoma
YE Jian-fei,ZHAO Lei,WANG Guo-liang,HONG Kai,MA Lu-lin( )
)
- Department of Urology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R737.21

| [1] | 黄健, 王建业, 孔垂泽, 等. 中国泌尿外科和男科疾病诊断治疗指南[M]. 北京: 科学出版社, 2020: 145. |
| [2] |
Motzer RJ, Jonasch E, Agarwal N, et al. Testicular cancer, version 2.2015[J]. J Natl Compr Canc Netw, 2015, 13(6):772-799.
doi: 10.6004/jnccn.2015.0092 |
| [3] |
Albers P, Albrecht W, Algaba F, et al. Guidelines on testicular cancer: 2015 Update[J]. Eur Urol, 2015, 68(6):1054-1068.
doi: 10.1016/j.eururo.2015.07.044 pmid: 26297604 |
| [4] |
Yi J, Zhou DA, Huo JR, et al. Primary intratesticular rhabdomyosarcoma: A case report and literature review[J]. Oncol Lett, 2016, 11(2):1016-1020.
doi: 10.3892/ol.2015.3987 |
| [5] |
Lovric E, Hizak DB, Balja MP, et al. An unusual mixed germ cell tumor of the testis consisting of rhabdomyosarcoma, mature teratoma and yolk sac tumor[J]. Asian J Androl, 2010, 12(3):451-452.
doi: 10.1038/aja.2010.2 |
| [6] |
Korski K, Breborowicz D, Filas V, et al. A case of primary testi-cular germ cell tumor with rhabdomyosarcoma metastases as an example of applying the FISH method to diagnostic pathology[J]. APMIS, 2007, 115(11):1296-1301.
doi: 10.1111/apm.2007.115.issue-11 |
| [7] |
Erbay ME, Tarhan F, Barisik NO, et al. A case of testicular rhabdomyosarcoma[J]. Int Urol Nephrol, 2004, 36(1):73-75.
doi: 10.1023/B:UROL.0000032671.74121.d3 |
| [8] | Gow KW, Murphy JR, Wu JK, et al. Metastatic testicular rhabdomyosarcoma: A report of two cases[J]. J Pediatr Surg, 2003, 38(8):E1-E3. |
| [9] |
Liu ZW, Zhang XQ, Hou GL, et al. Primary adult intratesticular rhabdomyosarcoma: Results of the treatment of six cases[J]. Int J Urol, 2011, 18(2):171-174.
doi: 10.1111/iju.2011.18.issue-2 |
| [10] |
Banfield GK, Brookstein R. Rhabdomyosarcoma arising in teratoma of the testis[J]. J R Army Med Corps, 1995, 141(3):167-168.
doi: 10.1136/jramc-141-03-07 |
| [11] | Kelly B, Lundon D, Rowaiye B, et al. Embryonal rhabdomyosarcoma of the testis[J]. Can Urol Assoc J, 2011, 5(1):E7-E10. |
| [12] | Nakagawa R, Aoyama S, Urata S, et al. Testicular rhabdomyosarcoma after chemotherapy for metastatic germ cell tumors[J]. Int Cancer Conf J, 2019, 8(4):175-180. |
| [13] |
Ishiguro N, Motoi T, Osaki M, et al. Immunohistochemical analysis of a muscle ankyrin-repeat protein, Arpp, in paraffin-embedded tumors: Evaluation of Arpp as a tumor marker for rhabdomyosarcoma[J]. Hum Pathol, 2005, 36(6):620-625.
pmid: 16021567 |
| [14] |
Kumar S, Perlman E, Harris CA, et al. Myogenin is a specific marker for rhabdomyosarcoma: An immunohistochemical study in paraffin-embedded tissues[J]. Mod Pathol, 2000, 13(9):988-993.
doi: 10.1038/modpathol.3880179 |
| [15] |
Walterhouse D, Watson A. Optimal management strategies for rhabdomyosarcoma in children[J]. Paediatr Drugs, 2007, 9(6):391-400.
doi: 10.2165/00148581-200709060-00006 |
| [16] |
Breitfeld PP, Meyer WH. Rhabdomyosarcoma: New windows of opportunity[J]. Oncologist, 2005, 10(7):518-527.
pmid: 16079319 |
| [17] |
Wiener ES, Anderson JR, Ojimba JI, et al. Controversies in the management of paratesticular rhabdomyosarcoma: Is staging retroperitoneal lymph node dissection necessary for adolescents with resected paratesticular rhabdomyosarcoma?[J]. Semin Pediatr Surg, 2001, 10(3):146-152.
pmid: 11481652 |
| [18] |
Urgun DA, Bista B, Krishnam M. Unusual presentation of testicular rhabdomyosarcoma metastases to the right ventricle papillary muscle and tricuspid valve[J]. Radiol Case Rep, 2020, 15(9):1562-1565.
doi: 10.1016/j.radcr.2020.05.075 |
| [19] |
Ferrari A, Casanova M, Massimino M, et al. The management of paratesticular rhabdomyosarcoma: A single institutional experience with 44 consecutive children[J]. J Urol, 1998, 159(3):1031-1034.
doi: 10.1016/S0022-5347(01)63830-8 |
| [1] | Guo-zhong LIN,Zhen-yu WANG,Bin LIU,Shao-min YANG. Intraspinal metastasis of alveolar rhabdomyosarcoma: A case report [J]. Journal of Peking University(Health Sciences), 2019, 51(6): 1165-1168. |
| [2] | Jian-fei YE,Bing WANG,Lu-lin MA,Lei ZHAO,Guo-liang WANG,Kai HONG. Organ-sparing partial orchietectomy for testicular adenomatoid tumor [J]. Journal of Peking University(Health Sciences), 2019, 51(2): 365-368. |
| [3] | HUA Ke-han, YANG Lei, ZHANG Xiao-wei, BAI Wen-jun, LI Qing, XU Tao. Complete androgen insensitivity syndrome associated with vesical fistula: a case report and literature review [J]. Journal of Peking University(Health Sciences), 2017, 49(4): 724-729. |
| [4] | HAO Han, SU Xiao-hong, ZHENG Wei, GE Peng, HE Qun, SHEN Qi, YANG Xin-yu, ZHANG Zheng, LI Xue-song, LIN Jian, ZHOU Li-qun. Radical cystectomy in patients with pathological non-muscle invasive bladder cancer [J]. Journal of Peking University(Health Sciences), 2016, 48(4): 627-631. |
| [5] | ZHANG Yu-jie, LIU Bao-guo, ZHAO Zhi-yan, SHENG Jin-dong, FENG Dong-dong. Relationship and clinical significance between mutated BRAF with prophylactic central-neck nodal dissection in papillary thyroid carcinoma [J]. Journal of Peking University(Health Sciences), 2016, 48(3): 502-506. |
| [6] | MENG Yi-Sen, Su-Yang, Fan-Yu, Yu-Wei, Wang-Yu, Zheng-Wei, Chen-Cheng, Zhou-Li-Qun, Zhang-Qian, Li-Xue-Song, . Risk factors for the development of postoperative paralytic ileus after radical cystectomy: a report of 740 cases [J]. Journal of Peking University(Health Sciences), 2015, 47(4): 628-633. |
|
||