Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (6): 1183-1187. doi: 10.19723/j.issn.1671-167X.2021.06.029
Previous Articles Next Articles
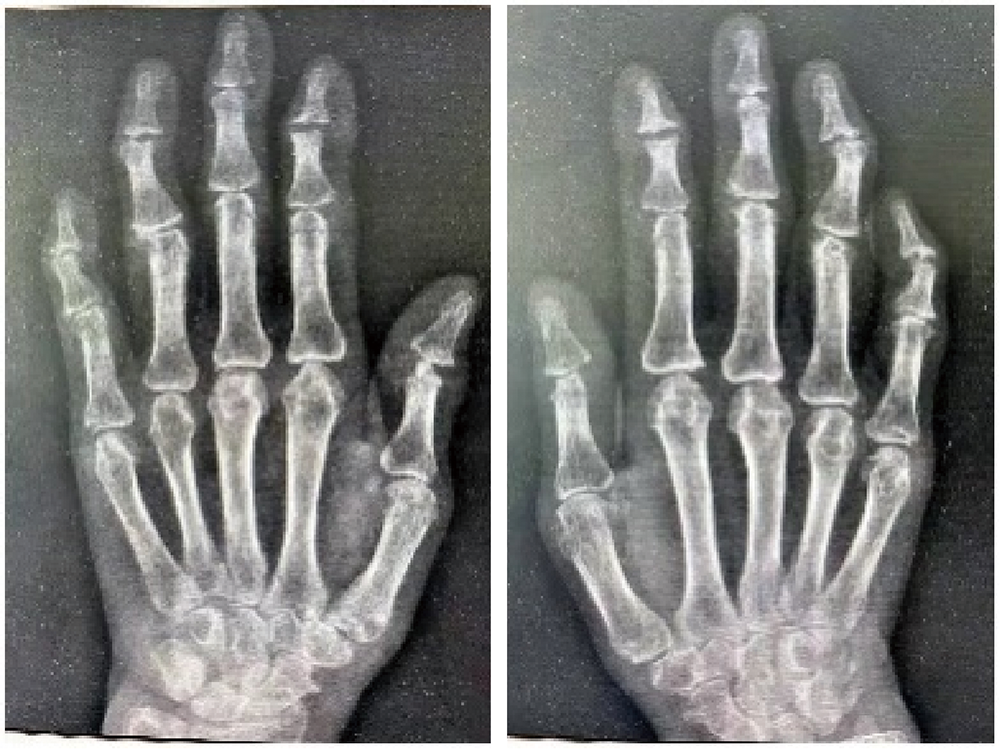
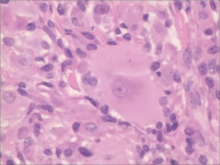
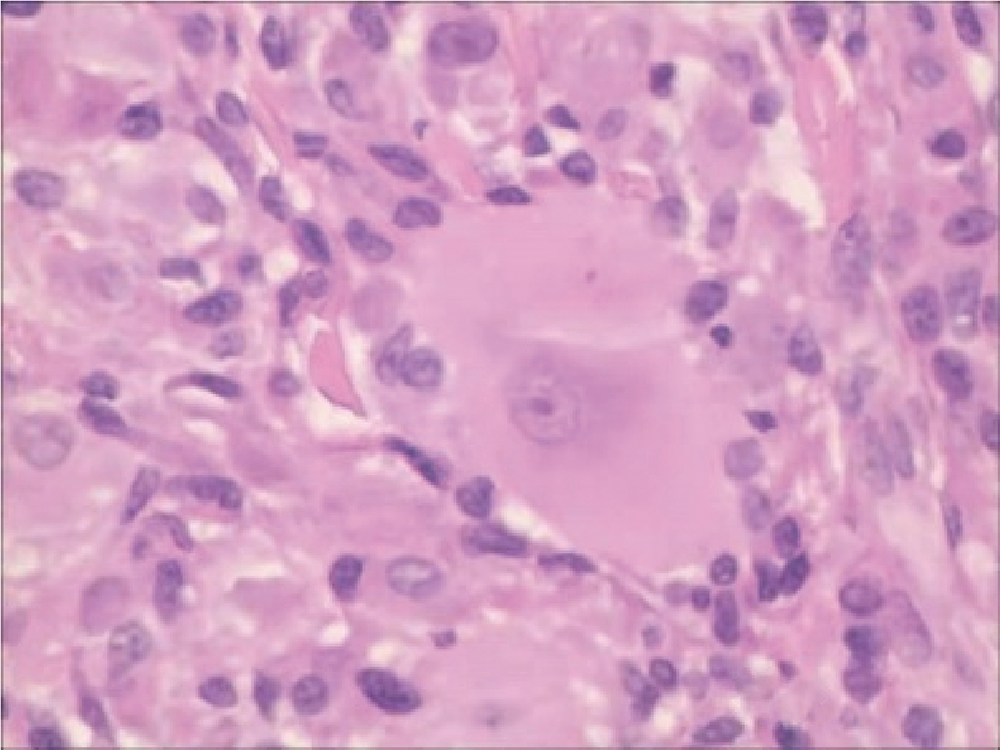
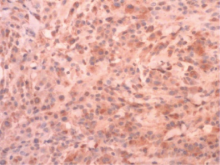
Multicentric reticulohistiocytosis: A case report
ZHAI Li1,QIU Nan1,SONG Hui2,△( )
)
- 1. Department of Rheumatology and Immunology, The 960th Hospital of the PLA Joint Logistics Support Force, Tai’an 271000, Shandong, China
2. Department of Traditional Chinese Medicine, Taian City Central Hospital, Tai’an 271000, Shandong, China
CLC Number:
- R59












| [1] | 王白鹤, 惠云, 苑春雨, 等. 多中心网状组织细胞增生症一例[J]. 中国麻风皮肤病杂志, 2018, 34(9):550-552. |
| [2] |
Luz FB, Gaspar TAP, Kalil-Gaspar N, et al. Multicentric reticulohistiocytosis[J]. J Eur Acad Dermatol Venereol, 2001, 15(6):524-531.
pmid: 11843211 |
| [3] |
Tajirian AL, Malik MK, Robinson-Bostom L, et al. Multicentric reticulohistiocytosis[J]. Clin Dermatol, 2006, 24(6):486-492.
pmid: 17113966 |
| [4] |
Tariq S, Hugenberg ST, Hirano-Ali SA, et al. Multicentric reticulohistiocytosis (MRH): Case report with review of literature between 1991 and 2014 with in depth analysis of various treatment regimens and outcomes[J]. Springerplus, 2016, 5(1):180.
doi: 10.1186/s40064-016-1874-5 |
| [5] |
Sanchez-Alvarez C, Sandhu AS, Crowson CS, et al. Multicentric reticulohistiocytosis: The Mayo clinic experience (1980-2017)[J]. Rheumatology(Oxford), 2020, 59(8):1898-1905.
doi: 10.1093/rheumatology/kez555 |
| [6] | 李慧娟, 王立, 侯勇, 等. 多中心网状组织细胞增生症8例临床特征[J]. 中华临床免疫和变态反应杂志, 2015, 9(3):213-217. |
| [7] |
Lu YY, Lu CC, Wu CH. Leonine facies in the cutaneous form of multicentric reticulohistiocytosis[J]. Intern Med, 2012, 51(15):2069-2070.
doi: 10.2169/internalmedicine.51.8119 |
| [8] |
Islam AD, Naguwa SM, Cheema GS, et al. Multicentric reticulohistiocytosis: A rare yet challenging disease[J]. Clin Rev Allergy Immunol, 2013, 45(2):281-289.
doi: 10.1007/s12016-013-8362-2 |
| [9] |
Gorman JD, Danning C, Schumacher HR, et al. Multicentric reticulohistiocytosis: Case report with immunohistochemical analysis and literature review[J]. Arthritis Rheum, 2000, 43(4):930-938.
doi: 10.1002/1529-0131(200004)43:4<930::AID-ANR27>3.0.CO;2-A |
| [10] | Yamamoto T. Skin manifestation associated with multicentric reticulohistiocytosis[J/OL]. J Clin Rheumatol, 2020(2020-12-15)[2021-08-01]. https://pubmed.ncbi.nlm.nih.gov/33337805/. |
| [11] |
El-Haddad B, Hammoud D, Shaver T, et al. Malignancy-associated multicentric reticulohistiocytosis[J]. Rheumatol Int, 2011, 31(9):1235-1238.
doi: 10.1007/s00296-009-1287-7 pmid: 20012625 |
| [12] | 白丽杰, 李鸿斌, 徐晓艳. 多中心网状组织细胞增多症1例并文献复习[J]. 临床荟萃, 2015, 30(7):831-832. |
| [13] |
Zhao H, Wu C, Wu M, et al. Tumor necrosis factor antagonists in the treatment of multicentric reticulohistiocytosis: Current clinical evidence[J]. Mol Med Rep, 2016, 14(1):209-217.
doi: 10.3892/mmr.2016.5253 |
| [14] | Lim K, D’Souza J, Vasquez JB, et al. Looks can be deceiving: A case report on multicentric reticulohistiocytosis successfully treated with rituximab[J]. Cureus, 2017, 9(5):e1220. |
| [15] |
Pacheco-Tena C, Reyes-Cordero G, Ochoa-Albíztegui R, et al. Treatment of multicentric reticulohistiocytosis with tocilizumab[J]. J Clin Rheumatol, 2013, 19(5):272-276.
doi: 10.1097/RHU.0b013e31829cf32b pmid: 23872542 |
| [16] |
Aouba A, Leclerc-Mercier S, Fraitag S, et al. Assessment and effective targeting of Interleukin-1 in multicentric reticulohistyo-cytosis[J]. Joint Bone Spine, 2015, 82(4):280-283.
doi: 10.1016/j.jbspin.2015.02.003 |
| [1] | Doudou MA, Xiaocai MA, Tianjing CHANG, Lifang WANG, Yan DING, Lianjie SHI. Bone marrow infiltration of large B-cell lymphoma with clinical manifestations similar to systemic lupus erythematosus: A case report [J]. Journal of Peking University (Health Sciences), 2026, 58(3): 666-669. |
| [2] | Youdong LIU, Yajun LYU, Jie CHEN, Mingde ZANG, Hongda PAN, Xiaowen LIU, Jun LU, Fenglin LIU. Clinical efficacy and safety of totally laparoscopic subtotal gastrectomy with cardia-gastric fundus preservation in middle-upper gastric cancer [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 301-306. |
| [3] | Weihao LI, Xuemin ZHANG, Wei LI, Tao ZHANG, Xiaoming ZHANG. Outcomes of suture-mediated vascular closure device in the closure of left brachial artery access site after thoracic endovascular aortic repair [J]. Journal of Peking University (Health Sciences), 2026, 58(2): 388-392. |
| [4] | Ebrahimi Farin, Zhiqiang FENG, Ebrahimi Faraz, Weihua HAN, Ziyang YU, Kuankuan JIA, Jingang AN. Surgical treatment outcomes of different stages of maxillary medication-related osteonecrosis of the jaw [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 107-114. |
| [5] | Ye ZHAO, Xiaoli DIAO, Yan XIONG. Application of cell transfer technology in pathological diagnosis of micro-volume cell fluid [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 208-213. |
| [6] | Hailing ZANG, Yuhong LIANG. Endodontic retreatment of a maxillary second molar with chronic apical periodontitis and separated instrument: A case report [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 214-219. |
| [7] | Yue WANG, Yuhong LIANG. Florid cemento-osseous dysplasia: A case report [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 220-224. |
| [8] | Lianfei PAN, Wenjing LI, Ruiyang WANG, Jian JIAO, Zhanqiang CAO, Li GAO, Dong SHI. Short-term efficacy and influencing factors of systemic antibiotics as an adjunct to mechanical periodontal therapy for stages Ⅲ/Ⅳ periodontitis [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 30-36. |
| [9] | Yanting CHI, Hongjie JIANG, Yan CHEN, Zhixiu XU, Binbin LI. Value of direct immunofluorescence in the diagnosis of oral mucosal pemphigus vulgaris: A retrospective study based on multi-index combined analysis [J]. Journal of Peking University (Health Sciences), 2026, 58(1): 68-73. |
| [10] | Jingyan GU, Xinyi LI, Jinxia ZHAO, Rong MU. Diabetic Charcot neuroarthropathy initially misdiagnosed as rheumatoid arthritis and gout: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1193-1197. |
| [11] | Xiaodi XIAO, Youchen XIA, Jianying LIU, Peng FU. Left sided sternocleidomastoid interosseous intravascular papillary endothelial hyperplasia: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 1002-1004. |
| [12] | Shang XIE, Luming WANG, Xinyuan ZHANG, Qiushi FENG, Yangyang XIA, Ziwei DAI, Xiaofeng SHAN, Zhigang CAI. Construction and application of oral squamous cell carcinoma organoid bank [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 847-851. |
| [13] | Xiangyu SUN, Chao YUAN, Xinzhu ZHOU, Jing DIAO, Shuguo ZHENG. Application of salivary micro-ecosystem in early prevention and control of oral and systemic diseases [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 859-863. |
| [14] | Yuanyuan YANG, Shanshan ZHANG, Guangyan YU, Huijun YANG, Hongyu YANG. Clinical outcomes of partial sialoadenectomy for the treatment of benign tumors in the submandibular gland [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 334-339. |
| [15] | Zhao CHEN, Yongkang QIU, Lei KANG. Classical Sweet syndrome with multiple organ lesions by 18F-FDG PET/CT: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(2): 403-407. |
|
||