
桥本甲状腺炎(Hashimoto thyroiditis,HT)和格雷夫斯病(Graves disease,GD)是自身免疫性甲状腺病中最常见的两种类型,是由于免疫系统失常导致甲状腺组织受到攻击所致的疾病[1-3]。HT以甲状腺功能减退为主要特征,患者常伴有甲状腺肿大,可能导致发声困难、吞咽困难和呼吸困难等颈部压迫症状,以及涉及多器官和组织的甲状腺功能减退症状;而GD则以甲状腺功能亢进为典型表现,约有一半的GD患者会出现眼球突出、眼睑肿胀等眼部症状,以及心悸、失眠、焦虑等甲状腺功能亢进症状[4-5]。近年来,随着生活方式变化和环境因素影响,自身免疫性甲状腺病的流行趋势显著上升,且女性患病率明显高于男性[6],这种性别差异可能是由于女性的雌激素刺激免疫反应而导致的[1],因此,女性人群的HT和GD的患病情况需要重点关注。
1 资料与方法
1.1 数据来源
本研究基于平台的电子病历数据,提取青岛市2022—2024年确诊的HT和GD病例信息。根据2020年山东省第七次人口普查数据,获取青岛市性别、年龄(5岁一组)和区域的分层人口数据[12]。
本研究使用的数据已通过北京大学生物医学伦理委员会的批准(批准号:IRB00001052-24067)。
1.2 研究对象
纳入标准:(1)2022年1月1日至2024年12月31日在平台有记录的所有常住居民,常住居民定义为在青岛市居住6个月及以上并在平台上建立健康档案的人群;(2)在平台的记录大于1年;(3)年龄为10~59岁的女性。排除标准:个人唯一标识缺失。
1.3 资料提取与整理
本研究通过平台的电子病历系统提取HT和GD的诊断信息,查询表单包括门诊和住院的就诊记录表、诊断明细表、出院小结表,提取变量包括出生日期、地区、保险类型、诊断时间、《疾病和有关健康问题的国际统计分类(第10次修订版)》[International Statistical Classification of Diseases and Related Health Problems (10th revision),ICD-10]编码和诊断名称等。
本研究运用模糊匹配的检索手段,疾病的识别算法由诊断编码和名称组成。HT的病例识别:采用ICD-10编码E06.3,结合临床诊断名称“桥本甲状腺炎”“桥本病”“慢性淋巴细胞性甲状腺炎”等关键词进行判定。GD的病例识别:采用ICD-10编码为E05.0,结合临床诊断名称“Graves病”“格雷夫斯甲状腺功能亢进症” “格雷夫斯甲亢” “毒性弥漫性甲状腺肿”等关键词进行判定。
数据脱敏:为确保参与研究的个体隐私不被泄露,本研究采用了严格的数据脱敏处理方法。所有患者的个人识别信息(如姓名、身份证号码、地址等)在收集后即被替换为唯一的匿名标识符,仅允许研究者跟踪病例进展,而不暴露任何可以追溯到具体个人的信息,以保证患者数据安全。
1.4 统计学分析
本研究使用R 4.2.2软件进行数据分析。对HT和GD病例数据进行描述性统计,采用频数和百分比描述年龄组、区县等分类变量。三年患病率(/10万)以2020年山东省第七次人口普查数据的青岛市10~59岁女性人口数为分母,2022—2024年累计确诊的HT或GD病例数为分子进行计算,并报告95%置信区间(confidence interval,CI);年度患病率(/10万)以2020年山东省第七次人口普查数据的青岛市10~59岁女性人口数为分母,各年新发HT或GD病例数和既往已确诊且存活病例数为分子进行计算,并报告95%CI,采用Cochran-Armitage趋势检验分析时间趋势。按年龄分组(10~14岁、15~19岁、…、55~59岁)计算年龄别三年患病率,按各区县分组(市南区、市北区、李沧区、崂山区、城阳区、黄岛区、即墨区、胶州市、平度市、莱西市)计算地区别三年患病率。采用卡方检验比较HT和GD患病率在不同年龄、地区间的分布差异。P < 0.05为差异有统计学意义,所有检验均为双侧检验。
2 结果
2.1 HT和GD患者的一般人口学特征
本研究共提取了40 362例HT患者和2 095例GD患者(表 1)。HT患者中,30~34岁年龄组构成比最高(19.83%),其次为35~39岁组(18.69%),10~14岁的HT患者构成比最低(0.72%);在地区分布上,黄岛区的HT患者构成比最高(17.72%),其次是市北区(12.13%),而莱西市构成比最低(3.75%);保险类型为基本医疗保险的HT患者占65.05%,全自费占27.65%。GD患者中,35~39岁年龄组构成比最高(15.42%),其次为30~34岁组(15.27%),10~14岁的患者占比最低(1.53%);即墨区的GD患者构成比最高(12.27%),其次是李沧区(11.46%),而莱西市构成比最低(4.11%);保险类型为基本医疗保险的GD患者占58.19%,全自费占34.61%。
表1 2022—2024年青岛市10~59岁女性桥本甲状腺炎和格雷夫斯病患者的人口学特征Table 1 Demographic characteristics of Hashimoto thyroiditis and Graves disease in females aged 10-59 years in Qingdao, 2022-2024 |
| Items | HT (n=40 362) | GD (n=2 095) |
| Age group/years, n(%) | ||
| 10-14 | 290 (0.72) | 32 (1.53) |
| 15-19 | 632 (1.57) | 90 (4.30) |
| 20-24 | 2 056 (5.09) | 153 (7.30) |
| 25-29 | 6 298 (15.60) | 259 (12.36) |
| 30-34 | 8 003 (19.83) | 320 (15.27) |
| 35-39 | 7 543 (18.69) | 323 (15.42) |
| 40-44 | 5 530 (13.70) | 249 (11.89) |
| 45-49 | 3 508 (8.69) | 211 (10.07) |
| 50-54 | 3 648 (9.04) | 260 (12.41) |
| 55-59 | 2 854 (7.07) | 198 (9.45) |
| Districts, n(%) | ||
| Shinan District | 3 840 (9.51) | 157 (7.49) |
| Shibei District | 4 895 (12.13) | 233 (11.12) |
| Huangdao District | 7 154 (17.72) | 183 (8.74) |
| Licang District | 3 875 (9.60) | 240 (11.46) |
| Laoshan District | 2 168 (5.37) | 189 (9.02) |
| Chengyang District | 4 031 (9.99) | 214 (10.21) |
| Jimo District | 3 586 (8.88) | 257 (12.27) |
| Jiaozhou City | 2 565 (6.35) | 130 (6.21) |
| Pingdu City | 3 328 (8.25) | 149 (7.11) |
| Laixi City | 1 513 (3.75) | 86 (4.11) |
| Unknown | 3 407 (8.44) | 257 (12.27) |
| Insurance types, n(%) | ||
| Basic medical insurance | 26 257 (65.05) | 1 219 (58.19) |
| Supplementary medical insurance | 142 (0.35) | 7 (0.33) |
| Special relief or grant | 244 (0.60) | 9 (0.43) |
| All expenses paid | 11 160 (27.65) | 725 (34.61) |
| Unknown | 2 559 (6.34) | 135 (6.44) |
HT, Hashimoto thyroiditis; GD, Graves disease. |
2.2 HT和GD的患病率
2.2.1 总人群的患病率
表2 2022—2024年青岛市10~59岁女性桥本甲状腺炎和格雷夫斯病患病率Table 2 Prevalence of Hashimoto thyroiditis and Graves disease in females aged 10-59 years in Qingdao, 2022-2024 |
| Items | HT | GD | |||||
| n | Prevalence rate (95%CI) (per 100 000) | P value | n | Prevalence rate (95%CI) (per 100 000) | P value | ||
| Three-year | |||||||
| (2022-2024) | 40 362 | 1 206.53 (1 194.79, 1 218.36) | 2 095 | 62.63 (59.97, 65.37) | |||
| Annual | < 0.001 | < 0.001 | |||||
| 2022 | 12 890 | 385.32 (378.69, 392.03) | 680 | 20.33 (18.83, 21.91) | |||
| 2023 | 26 292 | 785.94 (776.47, 795.50) | 1 405 | 42.00 (39.83, 44.25) | |||
| 2024 | 40 355 | 1 206.32 (1 194.58, 1 218.15) | 2 095 | 62.63 (59.97, 65.37) | |||
HT, Hashimoto thyroiditis; GD, Graves disease. Three-year prevalence rate (2022-2024) = Total cases during study period / Census population× 100 000; Annual prevalence rate = Cumulative cases by year-end / Census population ×100 000. |
2.2.2 患病率的年龄分布
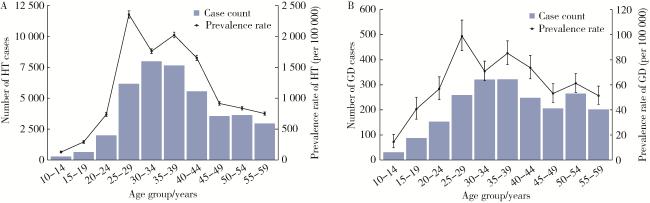
2022—2024年,HT三年患病率在不同的年龄组中差异存在统计学意义(χ2=12 164,P < 0.001);其中,2 5~29岁年龄组最高,为2 354.44/10万,其次为35~39岁组(2 022.20/ 10万)、30~34岁组(1 760.20/10万),10~14岁年龄组的HT三年患病率最低,为127.05 /10万(图 1A)。GD三年患病率在年龄分布上差异也存在统计学意义(χ2 =208.79,P < 0.001);其中,25~29岁组最高(98.90/10万),其次是35~39岁组(85.21/10万)、30~34岁组(63.25/10万),10~14岁组的GD三年患病率最低,为14.43/10万(图 1B)。
2.2.3 患病率的地区分布
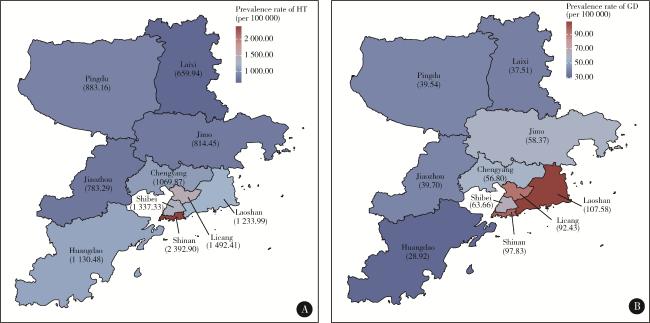
2022—2024年,青岛市各区县的HT三年患病率差异存在统计学意义(χ2 = 4 197.74,P < 0.001):市南区最高,为2 392.90/ 10万,其次为李沧区(1 492.41/10万)和市北区(1 337.33/10万);莱西市的HT三年患病率最低,为659.94/10万,其次为胶州市(783.29/10万,图 2A)。各区县GD的三年患病率差异亦具有统计学意义(χ2=335.79,P < 0.001):崂山区最高,为107.58/10万,其次是市南区(97.83/10万)和李沧区(92.43/10万);黄岛区的GD三年患病率最低,为28.92/10万,其次为莱西市(37.51/10万,图 2B)。
{kind=link}
{kind=link}
{kind=link}
{kind=link}
3 讨论
本研究基于青岛市全民健康信息平台,分析了2022—2024年青岛市10~59岁女性居民HT和GD的患病率及其年龄和地区分布特征。结果提示,2022—2024年青岛市10~59岁女性HT三年患病率为1 206.53/10万,年度患病率呈现逐年上升趋势(P < 0.001);年龄分布特征显示,25~29岁组和35~39岁组的HT三年患病率呈双峰分布;地区分布方面,市南区的HT三年患病率最高,莱西市最低。同期GD三年患病率为62.63/10万,年度患病率亦呈现显著上升趋势(P < 0.001);年龄分布显示25~29岁组和35~39岁组GD三年患病率较高;地区分布中,崂山区的GD三年患病率最高,黄岛区最低。
HT是一种甲状腺组织的慢性自身免疫性炎症,是原发性甲状腺功能减退的最常见病因,其流行情况在不同国家和地区因诊疗技术、生活环境和经济水平而异。本研究显示, 2022—2024年青岛市10~59岁女性居民的HT三年患病率为1 206.53/10万,与2000年山东省沿海地区7~74岁自然人群的抽样调查结果类似[13],但低于最新的荟萃分析数据[14-15]。Mohamed-Ahmed等[14]的荟萃分析显示,中国成人的HT汇总患病率为2 322(95%CI:2 057~ 2 620)/10万;Hu等[15]的荟萃分析显示中国成人的HT患病率为6 000/10万。本研究的HT患病率较低可能是由于研究所使用的数据来源于青岛市的电子病历数据,尽管青岛市全民健康信息平台覆盖了大多数医疗机构,但仍可能遗漏部分未就诊或未被诊断的患者,尤其是无症状或轻度症状的患者。且本研究通过ICD-10编码和诊断名称识别HT患者,可能导致甲状腺过氧化物酶抗体(thyroid peroxidase antibody,TPOAb)和/或甲状腺球蛋白抗体(thyroglobulin antibody,TgAb)阳性但未达到临床诊断标准的亚临床病例未被纳入[16]。此外,研究数据起始于2022年1月1日,既往确诊患者若在观察期内未因HT相关症状就诊,平台无法捕获此类病例,可能导致患病率被低估。
与欧美发达国家相比,我国的HT患病率处于较低水平[15, 17-18],可能是由于遗传与种族的差异性,以及发达国家更早地普及筛查,HT的早期诊断率更高所导致[14]。此外,由于HT通常表现为慢性病程,早期症状不明显,许多患者在疾病初期可能仅表现为TPOAb或TgAb阳性而无明显甲状腺功能异常,可能存在未及时就医或未被准确诊断的情况,导致HT诊断率偏低[5, 19]。在年龄分布上,本研究发现HT患病率在25~29岁和35~39岁呈现双峰分布,45岁以上的HT患病率逐渐下降,这与浙江、上海的研究结果类似[20-21]。女性在生育期、妊娠期和更年期等激素波动较大的阶段,HT的发病率显著增加,这可能是因为雌激素能够增强B细胞的活性,促进自身抗体的产生,从而导致HT的发生[1],提示应该重点关注该年龄段女性的甲状腺健康状况,加强HT相关的早期筛查、科普教育与健康管理。在地区分布上,本研究显示青岛市女性HT患病率最高的地区为市南区和李沧区,这可能与这些地区的经济水平较高、医疗资源丰富、诊断能力较强有关[14]。此外,青岛市全民健康信息平台的数据质量在各区之间可能存在差异,部分地区可能存在数据缺漏或患者跨区就诊导致的信息捕获不全问题,从而造成地区分布差异较大。
GD是甲状腺功能亢进症最常见的原因,也称为毒性弥漫性甲状腺肿[4]。本研究显示青岛市10~59岁女性居民中GD三年患病率为62.63/10万,低于荟萃分析报告的中国成人GD患病率(450/10万)[14],以及全国性流行病学抽样调查的结果(成人:0.53%;18~49岁育龄妇女:0.76%)[18, 22-23]。这种差异可能是由于部分私立医院及基层诊所的漏报导致病例低估,尤其是轻度或初发GD患者。此外,不同研究对GD的定义不一致,既往研究采用促甲状腺素受体抗体(thyrotropin receptor antibody,TRAb)阳性和甲状腺超声异常的综合诊断标准,而本研究依赖电子病历中的ICD-10编码及诊断名称,可能导致TRAb阴性或不典型病例未被纳入,导致研究结果存在差异[15]。此外,由于GD具有甲状腺功能亢进症状,需要进行鉴别诊断,实际可能存在漏诊和误诊的情况,导致患病率被低估,因而需要进一步提升医疗机构的诊断水平[3, 24]。在年龄分布上,本研究发现女性居民GD的患病率在25~29岁达到最大值,其次是35~39岁,与雌激素对免疫系统的调节作用密切相关[7-9]。与国际研究相比,本研究中的GD患者较为年轻,英国CPRD(Clinical Practice Research Datalink)人群研究显示,GD平均诊断年龄为59岁(43~75岁)[6];其原因可能是GD在女性中的患病率显著高于男性(女性与男性的患病率比约为10 ∶ 1),且女性发病年龄可能较男性更早[25],CPRD研究关注的是全人群,而本研究仅针对女性人群,因此可能放大了年轻化趋势。在地区分布上,GD的患病率没有呈现明显的特征,可能是由于GD的流行病学特征与碘摄入量的关系与HT相比较弱[26]。然而,一些研究表明,碘摄入量的增加可能会加重GD的病情,尤其是在碘缺乏地区补碘后,GD的发病率可能会暂时性升高[18, 21]。
本研究基于青岛市的电子病历数据,涵盖三级甲等医院至基层医疗机构,样本量较大,能够较全面地反映HT和GD的患病情况,填补了青岛市女性人群HT和GD的流行病学数据空白,为自身免疫性甲状腺病的预防控制提供了参考依据。但本研究也存在一定局限性:首先,尽管青岛市全民健康信息平台整合了全市二级及以上公立医疗机构的数据,但基层和私立医疗机构的数据采集尚不完善,可能遗漏轻症患者或未就诊人群,导致患病率的低估。其次,尽管本研究系统收集了临床诊断数据,但由于电子病历系统中社会人口学信息存在显著缺失,未能深入分析社会经济因素(如收入水平、婚姻状况、教育程度等)对疾病分布的影响,未来需要从多源数据获取尽可能多的相关变量,对自身免疫性甲状腺病的流行病学特征进行更加深入的分析;在人口数据上,本研究采用2020年第七次全国人口普查数据作为分母计算2022—2024年患病率,存在2~4年的人口结构滞后偏差,未来需要结合户籍登记系统,建立实时人口数据库以提高疾病负担评估的准确性。再次,病例识别方法还有待完善,研究通过ICD-10编码和临床诊断名称识别病例,可能遗漏早期病例,未来需结合实验室检查和甲状腺超声检查提升病例识别准确性。最后,由于研究可获取的数据时间范围较短,仅分析了2022—2024年这三年的HT和GD患病特征,无法全面反映疾病的长期变化趋势和规律。未来可考虑进一步扩大样本量,延长观察时间,并纳入更多的影响因素进行分析,以更全面地揭示HT和GD的流行病学特征。
综上所述,2022—2024年青岛市10~59岁女性居民HT和GD三年患病率为1 206.53/10万和62.63/10万,低于既往研究报告的HT和GD患病水平。年龄分布显示,25~39岁女性的HT和GD患病率明显高于其他年龄组,需重点关注该人群的甲状腺健康管理及早期筛查;HT和GD的流行病学特征存在地区差异,可能与各地区的经济条件、医疗水平以及电子病历数据的质量相关。未来需进一步延长观察时间对自身免疫性甲状腺病的流行病学特征进行更全面的描述。