
由于长期缺牙或其他疾病的影响,需要种植修复的患者常存在软硬组织缺乏的情况,给种植治疗带来了挑战。随着生物材料和组织工程的发展,各类骨替代材料(如自体骨、异体骨、合成骨等)和膜材料(如胶原膜、不可吸收膜、钛网等)在骨增量临床操作中获得了广泛应用;在软组织再生方面,自体游离龈移植与结缔组织移植仍是金标准,同时也出现了一些胶原基质、脱细胞真皮基质等生物材料的临床应用[6]。
在现有的软硬组织再生材料中,血浆基质作为来源于自体血液的生物材料,具有富含血小板等活细胞与生长因子的三维纤维蛋白网络,兼具优异的组织相容性与血管生成能力,同时可协同调节炎症微环境,促进成骨细胞与成纤维细胞的增殖与分化[7],因此,它可替代或部分增强传统生物材料的效果,特别是在牙槽嵴保存术、即刻种植、骨增量、软组织增量等领域展现出了较高的临床价值。本文以血浆基质研究与口腔种植临床应用为核心,结合国内外研究进展,系统梳理血浆基质在口腔种植软硬组织再生中的基础机制、应用策略与未来的优化和发展方向,以期为其规范化应用和深入研究提供参考。
1 血浆基质的分类及作用机制
1.1 血浆基质的分类
血浆基质是通过离心分离自体血液获得的一类富含血小板、白细胞与生长因子的三维纤维蛋白支架材料,按制备方法与产物形态的不同,经历了由富血小板血浆(platelet-rich plasma, PRP)、富血小板纤维蛋白(platelet-rich fibrin, PRF)、浓缩生长因子(concentrated growth factor, CGF)到近年发展形成的新一代血浆基质——水平富血小板纤维蛋白(horizontal platelet-rich fibrin, H-PRF)的技术演进[8]。第一代血浆基质PRP需添加抗凝剂与激活剂,操作繁琐且成分不稳定;第二代血浆基质PRF取消抗凝剂,形成固体凝胶,具备缓释生长因子的能力;第三代血浆基质CGF采用多段程序离心,试图进一步提高生长因子浓度和稳定性;第四代血浆基质H-PRF将传统的角度离心改变为水平离心方式,在细胞分布均匀性、生物成分保留、细胞损伤控制等方面具有显著优势,已成为血浆基质标准化制备的新方向[7]。
1.2 血浆基质促进再生的机制
血浆基质主要通过其三维纤维蛋白结构,实现包括血小板源性生长因子(platelet-derived growth factor, PDGF)、转化生长因子β (transforming growth factor-β, TGF-β)、血管内皮生长因子(vascular endothelial growth factor, VEGF)等生长因子的缓慢、持续释放,维持局部高浓度生长因子的修复微环境[9-10],因此,其可以调控多种修复相关细胞(成纤维细胞、成骨细胞、内皮细胞等)的增殖、迁移和分化,协同促进软硬组织再生[11-13]。血浆基质中的白细胞和细胞因子可调节局部免疫反应,实现部分抗菌效果,并且减少炎症,促进组织修复[7, 14]。此外,血浆基质的纤维蛋白网状结构可为细胞黏附、迁移和新生血管生成提供支架,同时作为生长因子的缓释库,促进组织修复。
1.3 血浆基质在口腔种植中的应用形式
血浆基质产物在口腔种植的临床应用上可以分为三种形式。
液态血浆基质:经手肘抽取患者静脉血于专用的液态血浆基质离心管,使用特定的离心参数制备而成,离心完成后通常可以在室温下保持十数分钟的液体状态[15],可用注射器抽取,在口腔种植中可用于冲洗拔牙窝、软组织注射、润湿种植体和其他生物材料等。
固态血浆基质:经手肘抽取患者静脉血于专用的固态血浆基质离心管,使用特定的离心参数制备而成,离心完成后可用器械夹取黄色凝胶部分,钝性分离红细胞后,根据需求将其压制成栓状或膜状,可单独或联合生物材料用于骨增量、软组织增量等[16]。
血浆基质骨块:血浆基质骨块是固态和液态血浆基质与颗粒状骨替代材料按照不同比例混合后获得的混合骨移植材料,它作为一个整体,具有一定的机械强度,便于操作,并且可以根据缺损区情况进行塑形,主要用于骨增量手术中[17]。
2 血浆基质在口腔种植相关领域的临床应用
在口腔种植领域,血浆基质广泛应用于引导骨组织再生术、牙槽嵴保存术、即刻种植、上颌窦底提升术及软组织增量等临床场景,以提升骨和软组织的再生效果。
2.1 引导骨组织再生术
在引导骨组织再生术中,血浆基质主要是通过混合自体骨屑或骨替代材料,形成具有机械强度的血浆基质骨块,用于水平或垂直骨增量时的骨缺损充填[18-19]。对于水平骨增量,根据术后是否可在理想位置植入理想尺寸的种植体及骨壁完整程度,将水平骨缺损分为三种类型:(1)种植体周围骨量足,但唇侧轮廓凹陷,可采用颗粒骨粉填充并覆盖固态血浆基质膜,以提升骨量与软组织质量;(2)种植体三面骨壁完整但颊侧存在缺损,适合采用血浆基质骨块填充,外覆胶原膜及固态血浆基质膜增强封闭效果与愈合速度;(3)骨量不足无法同步植入种植体时,需先期植骨,采用血浆基质骨块替代自体骨块,结合钛钉固定、胶原膜与固态血浆基质膜进行空间维持[19]。
2.2 牙槽嵴保存术
2.3 上颌窦底提升术
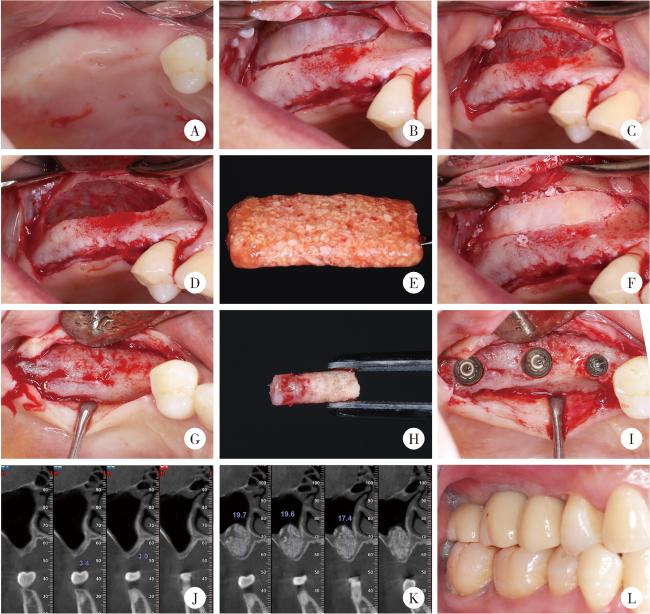
在经牙槽嵴顶上颌窦底提升术中,血浆基质可用于提升过程中分层支撑窦底黏膜,减少颗粒状骨替代材料外溢及膜穿孔风险。术中可将固态血浆基质膜折叠置入窦底下方,形成柔性缓冲层,再以血浆基质骨块逐层填入,适度敲击提升,每次提升幅度约1.5~2.0 mm。液态血浆基质可用于血浆基质骨块间隙塑形,增强成分整合[25]。在侧壁开窗上颌窦底提升术中,血浆基质膜可用于支撑上颌窦底黏膜,或是用于修补小的上颌窦底黏膜穿孔,血浆基质骨块则可以用于窦腔充填,从而发挥空间支撑和成骨引导的作用[26]。血浆基质膜可以在小范围上颌窦底提升中单独使用,在大范围上颌窦提升中血浆基质能够起到促进血管化和骨改建的作用[27-29], 如图 1所示。
{kind=link}
{kind=link}
图1 血浆基质骨块在上颌窦底提升术中的临床应用示例Figure 1 Clinical application of a representative plasmatrix bone block in maxillary sinus floor elevation A, intraoral view before surgery; B, preparation of the lateral window; C, exposure of the Schneiderian membrane; D, elevation of the Schneiderian membrane; E, plasmatrix bone block; F, repositioning of the lateral window after grafting with the bone block; G, alveolar bone condition six months after sinus floor elevation; H, intact bone column at the implant site; I, implant placement; J, preoperative CBCT showing insufficient alveolar bone height; K, CBCT at six months postoperatively showing adequate bone height; L, occlusion after prosthetic restoration. CBCT, cone beam CT. |
2.4 即刻种植
2.5 种植体周围软组织增量
2.6 种植体周围炎的治疗
3 血浆基质复合生物材料的研发
尽管血浆基质具有缓释多种生长因子、安全性高、生物相容性优良、操作简便等优势,但在口腔种植组织再生的应用中仍存在力学强度与体积有限、降解较快、生物活性有限等缺点,同时,因其成型性好、黏附性能佳,容易与其他材料结合,因此,可将血浆基质用作缓释载体或粘合剂成分,与其他生物材料复合,制备兼具机械支撑、生物活性与可控生长因子释放功能的三维复合支架,以满足口腔种植中对大体积骨缺损修复和长期组织再生的需求。目前的相关研究包括:血浆基质结合其他支架材料,例如混合透明质酸凝胶,使其兼具血浆基质的生长因子缓释与透明质酸的支架作用,显著提升牙龈成纤维细胞增殖、迁移及软组织再生效果[37];或是血浆基质混合壳聚糖-羟基磷灰石凝胶等,兼具机械支撑与生物活性[38];将血浆基质作为抗生素(如阿莫西林、甲硝唑、多西环素等)载体,使其具有持续抑菌能力,可显著减少术后的感染风险或用于感染性疾病的治疗[39];血浆基质负载外源活性成分或生长因子(如负载外泌体、维生素C、BMP-2等),可进一步提高其生物学活性[40];还可以结合数字化手段,基于影像学数据和口腔扫描数据设计个性化3D打印钛网或植骨导板,塑形血浆基质骨块,使其与骨缺损区紧密贴合,并且符合未来所需的骨再生形态,提高组织再生的精准性[41]。
4 总结与展望
血浆基质作为一种来源于自体血液的再生材料,凭借其富含生长因子、纤维蛋白与免疫细胞等多重活性成分,在口腔种植的多个环节中展现出了良好的生物学效应和广泛的适应性。无论是在拔牙后的拔牙窝保存,即刻种植术中的骨缺损填充和软组织封闭,还是在复杂的水平和垂直骨增量术、上颌窦底提升术以及软组织表型优化中,血浆基质均可通过多种形式(液态、膜状或骨块)参与组织修复与再建。然而,目前血浆基质的应用仍面临一些挑战与限制,其成分受个体因素影响较大,生物活性与治疗效果缺乏一致性;制备过程尚未完全标准化,不同离心参数和设备可能导致质量波动;在力学性能方面,尚难完全替代传统膜材料或自体组织移植,特别是在大体积骨缺损重建中。为进一步发挥其临床潜力,未来研究应致力于构建统一的制备标准与质量评价体系,发展其与其他骨再生或屏障材料的复合策略,并结合数字化技术与个性化医学理念优化其使用路径。此外,仍需更多前瞻性临床试验与长期随访数据支持其在不同适应证中的效果与安全性验证。