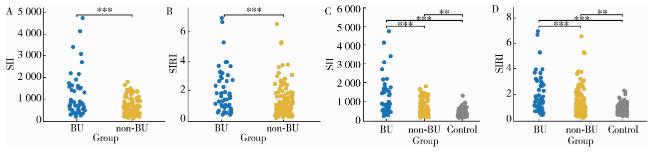
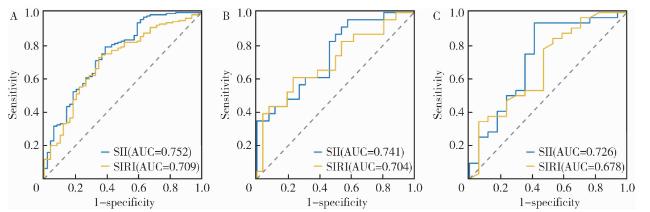
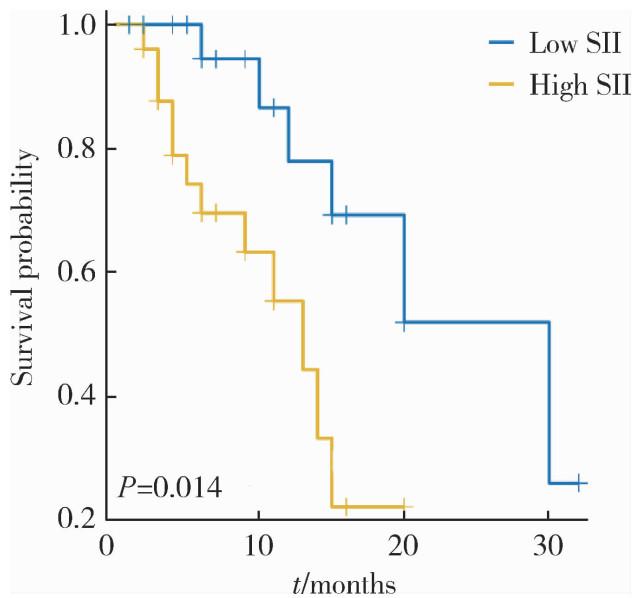
Objective: To evaluate the association of systemic immune-inflammation index (SII) and systemic inflammatory response index (SIRI) with Behçet disease uveitis (BU), and to assess their predictive value for inflammatory activity and clinical prognosis in BU patients. Methods: There were 194 patients diagnosed with Behçet disease (BD) and 122 healthy controls. The BD patients were classified into two subgroups based on disease activity: An active phase cohort (n=90) and a stable phase cohort (n=104). Furthermore, the patients were categorized according to the presence or absence of uveitis into two cohorts: BU (n=49) and non-BU (n=145). Among the BU cohort, 26 patients were in the active inflammatory stage, while 23 patients were in the quiescent inflammatory stage. SII and SIRI were calculated using routine blood parameters, including platelet, neutrophil, lymphocyte, and monocyte counts. Spearman correlation analysis was performed to assess the associations of SII and SIRI with BU onset, inflammatory activity, and inflammatory markers. Receiver operating characteristic (ROC) curve analysis was conducted to determine the optimal thresholds and predictive accuracy of SII and SIRI for BU onset and inflammatory activity. Results: SII and SIRI levels were significantly elevated in BD patients with ocular and vascular manifestations compared to those with stable disease (P < 0.05). No significant differences were observed in SII or SIRI levels among the patients with other clinical manifestations of BD. In the patients with BU, both SII and SIRI were significantly higher than in the non-BU and healthy control the groups (P < 0.001). Moreover, SII and SIRI levels were higher during the active inflamma-tory stage than in the inactive stage of BU (P=0.004). Spearman correlation analysis revealed that SII was positively associated with BD disease activity (ρ=0.303, P < 0.001), BU onset (ρ=0.442, P < 0.001), inflammatory activity (ρ=0.392, P=0.005), C-reactive protein (CRP, ρ=0.272, P < 0.001), and erythrocyte sedimentation rate (ESR, ρ=0.285, P < 0.001). SIRI was only positively correlated with BU onset (ρ=0.301, P=0.006). Logistic regression analysis demonstrated that eleva-ted SII was an independent risk factor for BU onset (OR=1.003, 95% CI: 1.001-1.004, P < 0.001). ROC curve analysis indicated that the optimal thresholds for SII were 711.800 [area under curve (AUC)=0.752] for predicting BU onset, 1 622.300 (AUC=0.741) for predicting inflammatory activity, and 1 634.200 (AUC=0.726) for predicting poor prognosis. The corresponding thresholds for SIRI were 1.260 (AUC=0.709), 1.390 (AUC=0.704), and 2.790 (AUC=0.678), respectively. Kaplan-Meier analysis indicated that elevated SII independently predicted adverse prognostic events (HR=3.440, 95%CI: 1.040-11.410, P=0.043). Conclusion: SII and SIRI may serve as potential clinical indicators for predicting inflammatory activity and prognosis in BD patients with uveitis. SII, in particular, demonstrates superior predictive performance for BU onset and disease activity, providing a basis for early identification of high-risk patients and clinical decision-making.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}