
抗磷脂综合征(antiphospholipid syndrome, APS)是一种以反复血管性血栓事件、复发性流产、血小板减少为主要临床表现,并伴随抗磷脂抗体(antiphospholipid antibodies, aPLs)持续中、高滴度阳性的自身免疫病[1]。流行病学资料显示,APS的患病率为40/10万~50/10万,年发病率为2/10万~ 5/10万,患者10年死亡率约为10%[2]。APS给患者的生理及心理带来双重打击,一项意大利研究以92名相对年轻的原发性APS患者(年龄18~45岁)为研究对象,发现与意大利普通人群相比,这些患者在生理健康和心理健康领域的生存质量(quality of life, QoL)均有所下降[3]。Sadetski等[4]的研究分析了36例原发性APS患者的心理状态,发现家庭照护依赖、社交能力丧失、自杀意念、焦虑、记忆减退等心理异常的发生率为97.1%。
1 资料与方法
1.1 研究对象
选择2021年9月至2025年10月于北京大学人民医院、郑州市第三人民医院就诊的APS患者进行调查。本研究样本由两部分构成:初始样本150例(收集于2021年9月至2022年12月);扩大样本46例(应评审专家建议,扩大样本量补充收集于2025年9月至10月)。入选标准:确诊的APS患者,所有患者均符合2006年在悉尼更新修订的APS分类诊断标准[6]。排除标准:(1)合并严重的活动性感染、活动性恶性肿瘤或其他严重的系统性自身免疫性疾病(如活动性系统性红斑狼疮)的患者;(2)存在认知功能障碍或精神疾病无法配合调查的患者;(3)不愿配合调查的患者;(4)妊娠期或哺乳期妇女。
健康对照组为年龄及性别相匹配的志愿者。排除标准:(1)经医生诊断或正在治疗中的任何器质性疾病,包括心血管、呼吸、内分泌、消化、泌尿、血液、神经、精神及免疫等系统的确诊疾病;(2)存在认知障碍,无法理解并配合完成本研究调查;(3)妊娠期或哺乳期妇女。
1.2 调查方法
由风湿免疫科医师组成调查小组,经患者知情同意后,采用手机扫码问卷星完成问卷调查,对照组在同时期填写问卷。
1.3 调查内容
患者一般情况:包括患者性别、年龄、病程、有无合并症等。
患者就医行为:包括就诊时间、就医途径、首次就诊及确诊的科室、首诊到确诊的间隔时间及分布、随诊的时间间隔。
患者用药情况:患者曾经用药及目前用药。
患者及对照组的焦虑抑郁情况:采用医院焦虑抑郁量表(hospital anxiety and depression scale, HADS)调查患者及对照组的焦虑抑郁情况,量表中A(1、3、5、7、9、11、13)代表焦虑项目,D(2、4、6、8、10、12、14)代表抑郁项目,将2套测试题的得分分别叠加即得出各自总分,>10分可视为焦虑或抑郁阳性[9]。
患者的用药依从性:采用普适性药物依从性量表(general medication adherence scale, GMAS)调查患者的用药依从性,30~33分表示患者依从性高,27~29分表示依从性良好,17~26分表示依从性一般,11~16分表示依从性低,0~10分表示依从性差[10]。
诊断延迟的定义:从首次出现相关症状到确诊为APS的时间[11]。
1.4 统计学分析
数据分析采用SPSS 26.0软件,使用Shapiro-Wilk检验进行正态性检验,符合正态分布的定量变量以均数±标准差表示,两组间比较采用t检验;不符合正态分布的数据采用中位数(四分位数间距)表示,两组间比较采用Mann-Whitney U检验;分类变量间的比较采用卡方检验。P < 0.05为差异有统计学意义。
2 结果
2.1 APS患者的一般情况
在196例APS患者中,女性171例,男性25例,男女比例为1 ∶ 6.8;中位年龄36岁(20~70岁),病程最长为31.1年,中位病程3.0年。12.8%(25/196)的患者合并系统性红斑狼疮,10.2%(20/196)的患者合并其他自身免疫病。在150例健康对照中,女性129例,男性21例,男女比例为1 ∶ 6.1;中位年龄36岁(22~60岁)。APS患者组及健康对照组之间性别(P=0.74)和年龄(P=0.31)的差异无统计学意义。
2.2 APS患者就医行为的分析
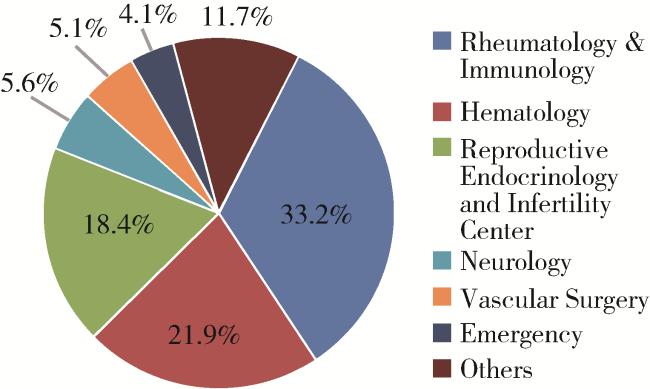
2.2.1 首诊及确诊科室分布
2.2.2 APS患者诊断延迟情况
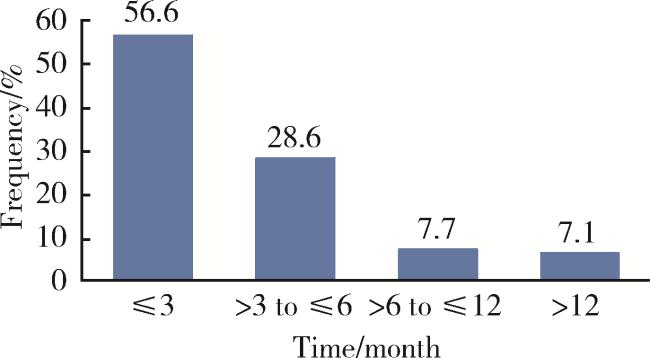
患者从出现血栓、反复流产、血小板减低等临床表现到确诊APS的中位时间为6.0(3.0,16.0)个月,其中诊断延迟超过1年的患者占32.1%(63/196)。从首诊到确诊时间≤6个月的患者占69.4%(136/196),>12个月的患者占13.8%(27/196)。
2.2.3 原发性与继发性APS患者就医路径和诊断延迟的比较
在151例原发性APS患者中,患者首次就诊于风湿免疫科者最多,占31.1%(47/151),其次为生殖科(20.5%,31/151),最终于风湿免疫科确诊者最多(80.8%,122/151),其次为生殖科(7.9%,12/151);而在45例继发性APS患者中,患者首次就诊于风湿免疫科者最多(40.0%,18/45),其次为血液科(26.7%,12/45),也是主要于风湿免疫科确诊(91.1%,41/45)。诊断延迟方面,原发性APS患者从出现临床表现到确诊APS的中位时间为6.0(3.0~16.0)个月,继发性APS患者为5.0(3.7~16.0)个月,二者差异无统计学意义(P=0.82)。
2.2.4 APS患者随诊的时间间隔
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
2.3 APS患者的用药情况
APS患者用药以羟氯喹、华法林等抗凝药物、抗血小板药物以及糖皮质激素为主。在治疗过程中,羟氯喹的使用率最高,占90.3%(177/196),其次为抗凝/抗血小板药物,总体使用率占88.3%(173/196),其中,抗血小板药物以阿司匹林为主(73.0%,143/196),抗凝药物中,低分子肝素的使用率为46.4%(91/196),华法林的使用率为23.0%(45/196),利伐沙班的使用率为11.2%(22/196)。此外,59.7%(117/196)的患者接受了包含糖皮质激素的治疗方案(表 1)。
表1 抗磷脂综合征患者的用药情况Table 1 Medication profiles of patients with antiphospholipid syndrome |
| Drugs | Previous, n (%) | Current, n (%) |
| Hydroxychloroquine | 177 (90.3) | 152 (77.6) |
| Antiplatelets and anticoagulants | 173 (88.3) | 141 (71.9) |
| Aspirin | 143 (73.0) | 94 (48.0) |
| Low molecular weight heparin | 91 (46.4) | 40 (20.4) |
| Rivaroxaban | 22 (11.2) | 6 (3.1) |
| Warfarin | 45 (23.0) | 35 (17.9) |
| Glucocorticoids | 117 (59.7) | 76 (38.8) |
| Immunosuppressants | 56 (28.6) | 41 (20.9) |
| Mycophenolate | 32 (16.3) | 19 (9.7) |
| Cyclophosphamide | 14 (7.1) | 1 (0.5) |
| Methotrexate | 6 (3.1) | 2 (1.0) |
| Leflunomide | 7 (3.6) | 2 (1.0) |
| Ciclosporin | 9 (4.6) | 8 (4.1) |
| Tacrolimus | 8 (4.1) | 8 (4.1) |
| Immunoglobulin | 21 (10.7) | 1 (0.5) |
| Rituximab | 13 (6.6) | 4 (2.0) |
| Statins | 17 (8.7) | 13 (6.6) |
| Drug-free | 0 (0) | 11 (5.6) |
用药依从性方面,在46例完成GMAS调查的患者中,34.8%(16/46)的患者依从性高,41.3%(19/46)的患者依从性良好,21.7%(10/46)的患者依从性一般,仅2.2%(1/46)的患者依从性差。
2.4 QoL和HADS调查
采用SF-36量表进行QoL评分调查,APS患者的GH评分显著低于健康人群,见表 2。
表2 抗磷脂综合征患者及健康对照的SF-36生存质量评估Table 2 Quality of life assessment using the SF-36 in patients with antiphospholipid syndrome and healthy controls |
| Sub-domain | SF-36 | P | |
| APS patients (n=196) | Healthy controls (n=150) | ||
| Physical functioning | 95 (85, 100) | 95 (90, 100) | 0.15 |
| Role physical | 100 (50, 100) | 100 (75, 100) | 0.07 |
| Bodily pain | 72 (62, 100) | 72 (62, 100) | 0.06 |
| General health | 57.0 (40.0, 77.0) | 65.0 (52.0, 77.8) | < 0.01* |
| Vitality | 60 (50, 75) | 65 (50, 75) | 0.33 |
| Social functioning | 87.5 (62.5, 100.0) | 87.5 (62.5, 100.0) | 0.65 |
| Role emotional | 100.0 (33.3, 100.0) | 100.0 (33.3, 100.0) | 0.57 |
| Mental health | 68 (49, 80) | 68 (55, 76) | 0.28 |
* P < 0.05. Data are presented as M (P25, P75). SF-36, 36-item short form health survey; APS, antiphospholipid syndrome. |
HADS量表调查显示,APS患者中存在焦虑症状的比例较健康人群显著增加(13.8% vs. 6.7%, P=0.03),见表 3。
表3 抗磷脂综合征患者及健康对照HADS评分情况Table 3 HADS scores in patients with antiphospholipid syndrome and healthy controls |
| HADS scores | APS patients (n=196) | Healthy controls (n=150) | P |
| HADS-A, M (P25, P75) | 5 (2, 8) | 4 (2, 7) | 0.20 |
| HADS-A>10, n (%) | 27 (13.8) | 10 (6.7) | 0.03* |
| HADS-D, M (P25, P75) | 4 (1, 7) | 3 (1, 7) | 0.96 |
| HADS-D>10, n (%) | 19 (19.7) | 14 (9.3) | 0.91 |
* P < 0.05. HADS, hospital anxiety and depression scale; APS, antiphospholipid syndrome;A, anxiety subscale; D, depression subscale. |
3 讨论
本研究发现,APS患者首次就诊的科室分布比较广泛,包括风湿免疫科、血液科、生殖科、血管外科、神经内科、急诊科等,提示APS的临床表现复杂。确诊科室主要为风湿免疫科(83.2%,163/196),表明风湿免疫科在APS的诊断中具有核心作用,能够综合评估aPLs阳性及患者相关临床表现,从而确立诊断,但同时也提示患者和非风湿免疫专业的医师对于APS的认识度不足。因此,临床工作中,既要注意给患者普及相关疾病的知识,提高患者的就诊意识,又要增强非专业医师对风湿病知识的认识,同时需完善多学科协作(multi-disciplinary team, MDT)机制,其在APS的早期识别和诊断中至关重要[5]。
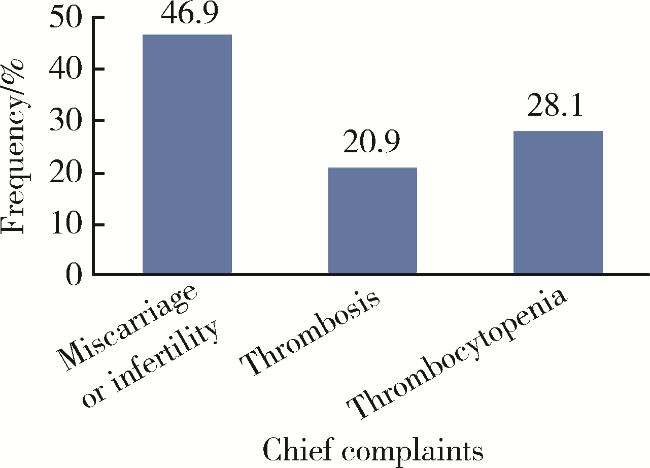
既往研究显示,APS患者中血栓发生率最高的是深静脉血栓,占31.7%[12],动脉血栓最常见的发生部位是脑循环系统,约30%的成人APS患者以缺血性卒中或短暂性脑缺血发作(transient ischemic attack, TIA)作为首发临床表现[13]。有文献报道,APS患者发生妊娠丢失的概率为23.8%~52.3%,以复发性流产和宫内死胎最多见[14],而APS的早发现、早诊断、早治疗可协助改善患者预后。对无症状aPLs携带者,使用低剂量阿司匹林进行一级预防,患者首次血栓形成的风险可降低一半[15]。有研究显示,通过规范化治疗,APS患者的血栓复发和妊娠结局可获得显著改善[16-17]。
由于APS临床表现复杂,症状多样化,累及多系统、多器官,致使部分患者的确诊时间较长,误诊、漏诊率较高,患者可能因延迟治疗而造成不可逆转的后遗症。国内有文献报道,从初始症状到确诊APS所需的中位时间为30个月,其中大于5年的患者有28%[5]。Radin等[11]的一项调查同样显示,自2000年以来,APS患者平均诊断延迟为2.2年,诊断延迟随时间推移有减低趋势,2015—2020年间,平均诊断延迟缩短为0.8年。本研究发现,随着对APS认识的逐渐加深,APS的中位诊断时间已缩短至6.0个月,反映了近年来在APS诊疗领域取得的巨大进步。这一效率的提升,主要得益于对APS认知的深化、检测技术的普及以及专科诊疗模式的推广。但是,从首次出现症状到确诊,时间间隔大于1年的患者仍高达32.1%,从初诊到确诊时间间隔大于1年的患者高达13.8%,表明仍有相当一部分患者会经历显著的诊断延迟,提示临床实践中仍需进一步提高对APS的警惕性,避免由于诊断延迟导致的血栓事件复发、器官功能损害或不良妊娠结局,给患者家庭和社会带来沉重负担。
有研究显示,APS患者可受益于硫酸羟氯喹[18]。本研究显示,APS患者的治疗过程中,羟氯喹的使用率高达90.3%,高于经典APS治疗方案(主要基于抗凝治疗),我们分析可能与以下几方面因素有关:首先,本研究人群可能包含了较高比例的复杂病例,例如复发性动脉血栓或合并其他自身免疫性疾病(如系统性红斑狼疮)的患者。对于此类患者,多项治疗指南均提出或推荐,在抗凝基础上联合使用羟氯喹进行辅助治疗[19-20]。其次,随着国内外研究的不断深入,发现羟氯喹除了具有免疫调节作用,还具有抑制血栓形成、改善妊娠结局等多种作用,已有研究显示,羟氯喹可使APS或aPLs阳性的患者获益[21-23]。此外,羟氯喹良好的药物安全性使其在长期管理中被广泛接受,特别是有生育需求的患者。这一现象揭示了当前APS临床实践正朝着更加个体化、强化免疫调节的方向发展,以期改善患者的远期预后。目前,国际治疗指南主要推荐采用维生素K拮抗剂、低分子肝素和(或)小剂量阿司匹林(75~100 mg/d)进行APS血栓和病理妊娠的预防和治疗,APS患者的二级血栓预防更推荐采用维生素K拮抗剂,而不是单用小剂量阿司匹林[19]。在本研究的41例以血栓为主诉的APS患者中,仅1例患者在治疗过程中单用小剂量阿司匹林。对于难治性产科APS,建议在妊娠前使用阿司匹林和羟氯喹的基础上,于妊娠期前3个月还应考虑加用小剂量(≤10 mg/d)泼尼松或同等剂量的糖皮质激素[1]。目前,免疫抑制剂的治疗效果仍有争议,有学者建议,微血管抗磷脂综合征(microvascular antiphospholipid syndrome, MAPS)的患者在病情活动时可使用霉酚酸酯[24]。治疗应个体化,根据不同患者的不同临床表现、病情严重程度及对治疗药物的反应等制定恰当的治疗方案[1]。如何规范治疗,以及系统评定达到最小疾病活动度甚至完全缓解,则需要患者进行规律随访,及时调整治疗方案以期改善预后。
本研究结果显示,对APS患者和健康人群进行SF-36量表调查,APS患者的GH评分显著下降。GH维度评估的是患者的总体健康感知和健康预期,GH评分低提示患者对于自身的总体健康评价低下,且预期趋于恶化[25],这可能源于疾病本身慢性、易复发的特性所导致的长期疾病不确定感,患者持续担忧血栓事件的复发、妊娠的失败以及治疗的长期副作用等。因此,未来对于患者的支持与干预,除了关注其生理症状的控制,也应重视对其疾病认知和心理预期的管理,以帮助患者重建积极的健康认同。根据HADS量表评估,APS患者焦虑的发病率较健康人群更高,与以往文献报道一致。APS患者常出现抑郁及焦虑等精神障碍和认知障碍,但其发生机制尚不清楚[26]。Gris等[27]的研究发现,相较于健康组,APS患者更容易出现抑郁症等情绪障碍和焦虑症。Georgopoulou等[28]的研究发现,APS患者健康相关生命质量(health related quality of life, HRQoL)减低与社会支持不足有关,增加对患者的宣教可能有助于改善APS患者的HRQoL。
综上所述,本研究发现APS患者在就诊延误、就诊科室选择、规律随诊、生存质量的健康感知方面及情绪焦虑方面存在问题,风湿免疫科应作为APS的诊治科室以提高诊断率,缩短确诊所需时间,并对患者进行心理疏导。本项调查结果为临床医生了解APS患者的就诊状况和规范化治疗提供了依据。