
1 病例资料
1.1 临床资料

图1 例1患者的影像特征及肉眼改变Figure 1 Imaging features and gross changes of case 1 A, the ultrasound image of case 1 showed mixed echogenic masses in the uterine cavity and bilateral ovaries with dark fluid areas (arrows indicate the fluid dark area of the mass); B, gross findings of case 1; The left side was the right ovary and the right side shows the whole uterus (arrows indicate the location of the mass). |
1.2 大体检查
1.3 镜下检查
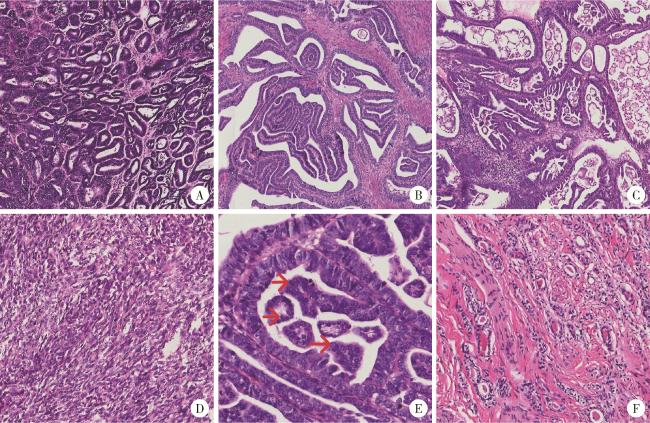
图2 3例患者的镜下特征(苏木精-伊红染色)Figure 2 Microscopic features of the three patients (hematoxylin-eosin staining) A, the tumor cells were tubular or glandular (×200); B, the tumor cells were papillary (×200); C, the tumor cells were micropapillary (×200); D, the tumor cells were spindle-shaped (×200); E, vesicular nuclei and nuclear furrows (red arrows) are visible at high magnification (×400); F, luminal eosinophilic homogeneous pink staining without structured secretions (×200). |
1.4 免疫组织化学染色
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
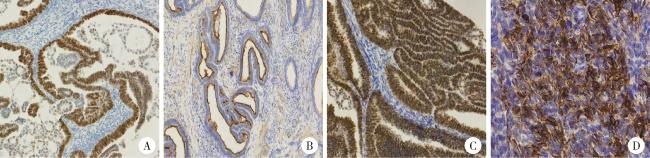
图3 3例患者的免疫组织化学染色特征(EnVision)Figure 3 Immunohistochemical staining characteristics of the three patients (EnVision) A, pair box gene 2 (PAX2) was diffusely positive in the nucleus (×200); B, the luminal margin was positive for CD10 (×200); C, thyroid transcription factor-1 (TTF1) was positive in the nucleus (×200); D, case 3 was positive for broad-spectrum CK in solid spindle cells (×200). |
1.5 分子特征
1.6 手术-病理分期
表1 3例患者手术-病理分期Table 1 Surgical-pathological staging of the three patients |
| Items | Case 1 | Case 2 | Case 3 |
| Depth of infiltration | 2/3 myometrium | Full myometrium and serosa | 3/5 myometrium |
| Tumor emboli in blood vessels and lymphatic vessels | >4 | >4 | >4 |
| Limited spread | Involving the cervix and both adnexa | Involving both adnexa | Involving the cervix |
| Pelvic lymph nodes | Negative | Negative | Negative |
| Distant metastasis | Negative | Peritoneal metastasis | Negative |