Journal of Peking University(Health Sciences) ›› 2018, Vol. 50 ›› Issue (6): 1049-1052. doi: 10.19723/j.issn.1671-167X.2018.06.019
• Article • Previous Articles Next Articles
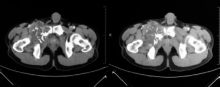
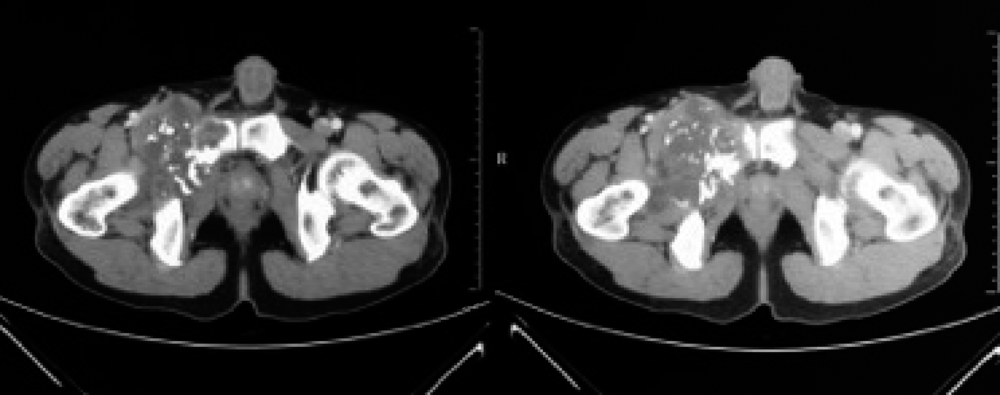
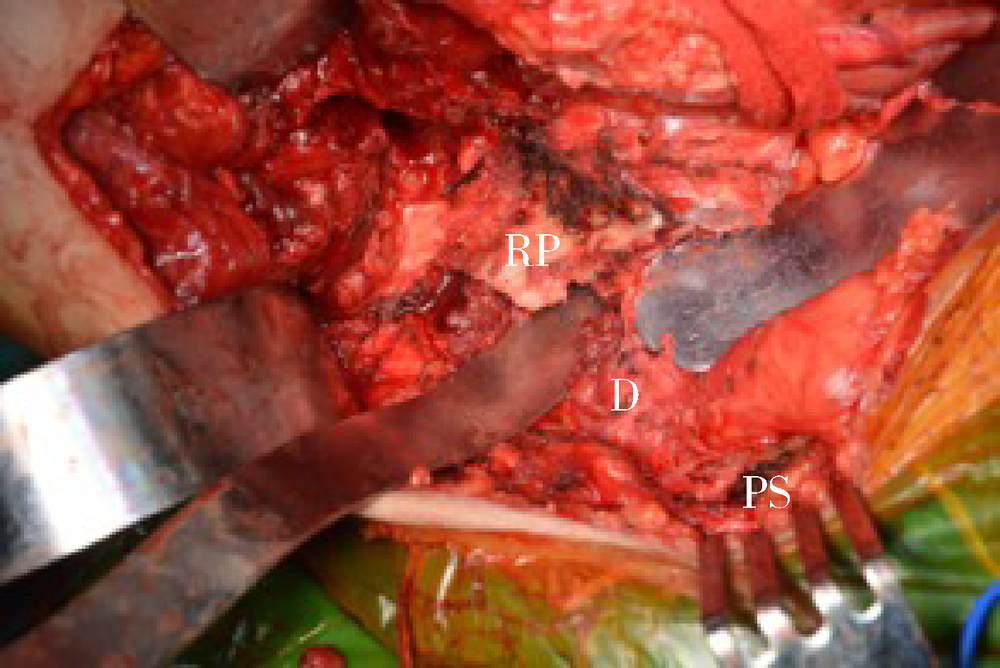
Application of artificial ligament in treatment of lower abdominal wall reconstruction after pubic tumor resection
Jie ZANG,Wei GUO( ),Xiao-dong TANG,Hua-yi QU,Da-sen LI
),Xiao-dong TANG,Hua-yi QU,Da-sen LI
- Musculoskeletal Tumor Center, Peking University People’s Hospital, Beijing 100044, China
CLC Number:
- R738.1







| [1] |
Enneking WF, Dunham WK . Resection and reconstruction for primary neoplasms involving the innominate bone[J]. J Bone Joint Surg Am, 1978,60(6):731-746.
doi: 10.2106/00004623-197860060-00002 pmid: 701308 |
| [2] |
Angelini A, Drago G, Trovarelli G , et al. Infection after surgical resection for pelvic bone tumors: an analysis of 270 patients from one institution[J]. Clin Orthop Relat Res, 2014,472(1):349-359.
doi: 10.1007/s11999-013-3250-x pmid: 3889428 |
| [3] |
Karim SM, Colman MW, Lozano-Calderon SA , et al. What are the functional results and complications from allograft reconstruction after partial hemipelvectomy of the pubis[J]. Clin Orthop Relat Res, 2015,473(4):1442-1448.
doi: 10.1007/s11999-014-4009-8 pmid: 4353538 |
| [4] |
Mankin HJ, Hornicek FJ . Internal hemipelvectomy for the management of pelvic sarcomas[J]. Surg Oncol Clin N Am, 2005,14(2):381-396.
doi: 10.1016/j.soc.2004.11.010 pmid: 15817245 |
| [5] |
Die Trill J, Madrid JM, Ferrero E , et al. Posthemipelvectomy hernia[J]. Hernia, 2005,9(4):375-377.
doi: 10.1007/s10029-005-0328-8 pmid: 15912261 |
| [6] |
Reddy SS, Bloom ND . En bloc resection of extra-peritoneal soft tissue neoplasms incorporating a type Ⅲ internal hemipelvectomy: a novel approach[J]. World J Surg Oncol, 2012,10:222.
doi: 10.1186/1477-7819-10-222 pmid: 3543210 |
| [7] |
Sternberg A, Yosipovich Z . Primary marlex-mesh reconstruction in partial resections of the hemipelvis. Report of 2 cases[J]. Acta Orthop Scand, 1989,60(3):365-368.
doi: 10.3109/17453678909149296 pmid: 2750517 |
| [8] |
Chao AH, Neimanis SA, Chang DW , et al. Reconstruction after internal hemipelvectomy: outcomes and reconstructive algorithm[J]. Ann Plast Surg, 2015,74(3):342-349.
doi: 10.1097/SAP.0b013e31829778e1 |
| [9] |
Lavoie P, Fletcher J, Duval N . Patient satisfaction needs as related to knee stability and objective findings after ACL reconstruction using the LARS artificial ligament[J]. Knee, 2000,7(3):157-163.
doi: 10.1016/S0968-0160(00)00039-9 pmid: 10927209 |
| [10] |
Parchi PD, Ciapini G, Paglialunga C , et al. Anterior cruciate ligament reconstruction with LARS artificial ligament-clinical results after a long-term follow-up[J]. Joints, 2018,6(2):75-79.
doi: 10.1055/s-0038-1653950 |
| [11] |
Wang XM, Ji G, Wang XM , et al. Biological and biomechanical evaluation of autologous tendon combined with ligament advanced reinforcement system artificial ligament in a rabbit model of anterior cruciate ligament reconstruction[J]. Orthop Surg, 2018,10(2):144-151.
doi: 10.1111/os.12370 pmid: 29624874 |
| [12] |
Wilson RJ, Freeman TH Jr, Halpern JL , et al. Surgical outcomes after limb-sparing resection and reconstruction for pelvic sarcoma: asystematic review[J]. JBJS Rev, 2018,6(4):e10.
doi: 10.2106/JBJS.RVW.17.00072 |
| [13] |
Reali C, Guy R, Darby CR , et al. Complex reconstruction with flaps after abdominoperineal resection and groin dissection for anal squamous cell carcinoma: adifficult case involving many specialities[J]. Am J Case Rep, 2018,19:61-67.
doi: 10.12659/AJCR.906818 |
| [1] | YUE Lei,WANG Yue-tian,BAI Chun-bi,CHEN Hao,FU Hao-yong,YU Zheng-rong,LI Chun-de,SUN Hao-lin. Analysis of surgical strategy of percutaneous endoscopic lumbar discectomy in young and middle-aged double-segment patients with lumbar disc herniation [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 734-739. |
|
||