Journal of Peking University(Health Sciences) ›› 2019, Vol. 51 ›› Issue (4): 632-635. doi: 10.19723/j.issn.1671-167X.2019.04.006
Previous Articles Next Articles
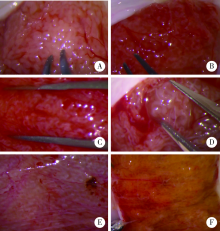
Analysis of intratesticular condition in micro-dissection testicular sperm extraction era
Lian-ming ZHAO1,Hui JIANG1,△( ),Kai HONG1,Hao-cheng LIN1,Wen-hao TANG1,De-feng LIU2,Jia-ming MAO2,Zhe ZHANG1,Sheng-li LIN2,Lu-lin MA1
),Kai HONG1,Hao-cheng LIN1,Wen-hao TANG1,De-feng LIU2,Jia-ming MAO2,Zhe ZHANG1,Sheng-li LIN2,Lu-lin MA1
- 1.Department of Urology, Peking University Third Hospital, Beijing 100191, China
2. Department of Obstetrics and Gynecology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R699

| [1] | Schlegel PN . Testicular sperm extraction: microdissection improves sperm yield with minimal tissue excision[J]. Hum Reprod, 1999,14(1):131-135. |
| [2] | AbdellRaheem A, Garaffa G, Rushwan N , et al. Testicular histopathology as a predictor of a positive sperm retrieval in men with non-obstructive azoospermia[J]. BJU Int, 2013,111(3):492-499. |
| [3] | Ramasamy R, Ricci JA, Palermo GD , et al. Successful fertility treatment for Klinefelter’s syndrome[J]. J Urol, 2009,182(3):1108-1113. |
| [4] | Jarow JP, Espeland MA, Lipshultz LI . Evaluation of the azoospermic patient[J]. J Urol, 1989,142(1):62-65. |
| [5] | Walker WH, Cheng J . FSH and testosterone signaling in Sertoli cells[J]. Reproduction, 2005,130(1):15-28 |
| [6] | Valenti D, La Vignera S, Condorelli RA , et al. Follicle-stimu-lating hormone treatment in normogonadotropic infertile men[J]. Nat Rev Urol, 2013,10(1):55-62 |
| [7] | Acosta AA, Khalifa E, Oehninger S . Pure human follicle stimu-lating hormone has a role in the treatment of severe male infertility by assisted reproduction: Norfolk’s total experience[J]. Hum Reprod, 1992,7(8):1067-1072. |
| [8] | 杨俊, 刘继红 . 睾丸活检在非梗阻性无精症中应用前景及问题[J]. 中国男科学杂志, 2011,25(4):61-64. |
| [9] | Bryson CF, Ramasamy R, Sheehan M , et al. Severe testi-cular atrophy does not affect the success of microdissection testicular sperm extraction[J]. J Urol, 2014,191(1):175-178. |
| [10] | Ramasamy R, Lin K, Gosden LV , et al. High serum FSH levels in men with nonobstructive azoospermia does not affect success of microdissection testicular sperm extraction[J]. Fertil Steril, 2009,92(2):590-593. |
| [1] | Jia-ming MAO,Lian-ming ZHAO,De-feng LIU,Hao-cheng LIN,Yu-zhuo YANG,Hai-tao ZHANG,Kai HONG,Rong LI,Hui JIANG. Analysis of clinical outcome of synchronous micro-dissection testicular sperm extraction and intracytoplasmic sperm injection in male infertility with Y chromosome azoospermia factor c region deletion [J]. Journal of Peking University (Health Sciences), 2022, 54(4): 652-657. |
| [2] | PENG Jing,FANG Dong,ZHANG Zhi-chao,GAO Bing,YUAN Yi-ming,TANG Yuan,SONG Wei-dong,CUI Wan-shou. Testosterone levels in patients with varicocele and azoospermia [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 294-298. |
| [3] | DAI Xiao-wei, XU Ying, ZHENG Lian-wen, LI Ling-yun, LI Dan-dan1 TAN Xin, GAO Fei, WANG Yan, WU Gui-jie. Analysis of chromosome in 1 324 patients with oligozoospermia or azoosperm [J]. Journal of Peking University(Health Sciences), 2018, 50(5): 774-777. |
| [4] | MAO Jia-ming, LIU De-feng,ZHAO Lian-ming,HONG Kai, ZHANG Li, MA Lu-lin, JIANG Hui, QIAO Jie. Effect of testicular puncture biopsy on the success rate of microdissection testicular sperm extraction for idiopathic non-obstructive azoospermia [J]. Journal of Peking University(Health Sciences), 2018, 50(4): 613-616. |
|
||