Journal of Peking University (Health Sciences) ›› 2020, Vol. 52 ›› Issue (5): 875-880. doi: 10.19723/j.issn.1671-167X.2020.05.013
Previous Articles Next Articles
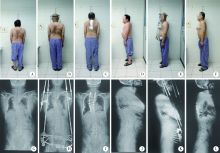
Clinical efficacy of short-term halo-pelvic traction combined with surgery in the treatment of severe spinal deformities
Bei-yu XU1,Long-tao QI1,Yu WANG1,∆( ),Chun-de LI1,∆(),Hao-lin SUN1,Shi-jun WANG1,Zheng-rong YU1,Yao ZHAO1,Long-long LIU2
),Chun-de LI1,∆(),Hao-lin SUN1,Shi-jun WANG1,Zheng-rong YU1,Yao ZHAO1,Long-long LIU2
- 1. Department of Orthopedics, Peking University First Hospital, Beijing 100034, China
2. Department of Orthopedics, Linfen Second People’s Hospital, Shanxi 041000, China
CLC Number:
- R682.1+3

| [1] |
Hamzaoglu A, Alanay A, Ozturk C, et al. Posterior vertebral column resection in severe spinal deformities: a total of 102 cases[J]. Spine (Phila Pa 1976), 2011,36(5):E340-E344.
doi: 10.1097/BRS.0b013e3182015712 |
| [2] | Bouchoucha S, Khelifi A, Saied W, et al. Progressive correction of severe spinal deformities with halo-gravity traction[J]. Acta Orthop Belg, 2011,77(4):529-534. |
| [3] |
Gollogly S, Smith JT, Campbell RM. Determining lung volume with three-dimensional reconstructions of CT scan data: a pilot study to evaluate the effects of expansion thoracoplasty on children with severe spinal deformities[J]. J Pediatr Orthop, 2004,24(3):323-328.
pmid: 15105731 |
| [4] |
Zhang Y, Xie J, Wang Y, et al. Thoracic pedicle classification determined by inner cortical width of pedicles on computed tomography images: its clinical significance for posterior vertebral column resection to treat rigid and severe spinal deformities-a retrospective review of cases[J]. BMC Musculoskelet Disord, 2014,15:278.
doi: 10.1186/1471-2474-15-278 pmid: 25124922 |
| [5] |
O’Brien JP, Yac ACMC, Hodgson AR. Halo pelvic traction: a technic for severe spinal deformities[J]. Clin Orthop Relat Res, 1973,93:179-190.
doi: 10.1097/00003086-197306000-00018 |
| [6] |
Arlet V, Papin P, Marchesi D. Halo femoral traction and sliding rods in the treatment of a neurologically compromised congenital scoliosis: technique[J]. Eur Spine J, 1999,8(4):329-331.
doi: 10.1007/s005860050182 pmid: 10483837 |
| [7] |
Qiu Y, Liu Z, Zhu F, et al. Comparison of effectiveness of Halo-femoral traction after anterior spinal release in severe idiopathic and congenital scoliosis: a retrospective study[J]. J Orthop Surg Res, 2007,2:23.
doi: 10.1186/1749-799X-2-23 pmid: 18047681 |
| [8] | Zhang HQ, Gao QL, Ge L, et al. Strong halo-femoral traction with wide posterior spinal release and three dimensional spinal correction for the treatment of severe adolescent idiopathic scoliosis[J]. Chin Med J (Engl), 2012,125(7):1297-1302. |
| [9] | 李彩红, 张梅清, 李晔, 等. 严重脊柱畸形患者术前颅-股骨牵引的护理[J]. 世界最新医学信息文摘:电子版, 2016,16(18):297-298. |
| [10] |
Hsu LC. Halo-pelvic traction: a means of correcting severe spinal deformities[J]. Hong Kong Med J, 2014,20(4):358-359.
pmid: 25243266 |
| [11] |
Yang C, Wang H, Zheng Z, et al. Halo-gravity traction in the treatment of severe spinal deformity: a systematic review and meta-analysis[J]. Eur Spine J, 2017,26(7):1810-1816.
pmid: 27858237 |
| [12] |
Pourtaheri S, Shah SA, Ditro CP, et al. Preoperative halo-gravity traction with and without thoracoscopic anterior release for skeletal dysplasia patients with severe kyphoscoliosis[J]. J Child Orthop, 2016,10(2):135-142.
doi: 10.1007/s11832-016-0721-0 pmid: 27016925 |
| [13] |
Kim NH, Kim HJ, Moon SH, et al. 20-year-follow up of treatment using spine osteotomy and halo-pelvic traction for tuberculous kyphosis[J]. Asian Spine J, 2009,3(1):27-31.
pmid: 20404943 |
| [14] |
Hodgson AR. Halo-pelvic traction in scoliosis[J]. Isr J Med Sci, 1973,9(6):767-770.
pmid: 4724284 |
| [15] | Dove J, Hsu LC, Yau AC. The cervical spine after halo-pelvic traction. An analysis of the complications of 83 patients[J]. J Bone Joint Surg Br, 1980,62B(2):158-161. |
| [16] | 赵聚峰, 杜志伟. 严重脊柱侧后凸畸形头盆环支撑牵引预治疗31例体会[J]. 实用骨科杂志, 2005,11(3):265-266. |
| [17] | 田慧中, 吕霞, 马原. 头盆环牵引全脊柱截骨内固定治疗重度脊柱弯曲[J]. 中国矫形外科杂志, 2007,15(3):167-172. |
| [18] |
Rozario RA, Stein BM. Complications of halo-pelvic traction. Case report[J]. J Neurosurg, 1976,45(6):716-718.
doi: 10.3171/jns.1976.45.6.0716 pmid: 978245 |
| [19] |
Ransford AO, Manning CW. Complications of halo-pelvic distraction for scoliosis[J]. J Bone Joint Surg Br, 1975,57(2):131-137.
pmid: 1141278 |
| [20] |
Ma JK, Ning LH. Posterior instrumentation and spondylodesis for scoliosis under halo-pelvic distraction with local anesthesia[J]. Zhonghua Wai Ke Za Zhi, 1987,25(7):390-393, 444.
pmid: 3677941 |
| [21] |
Zielke K, Pellin B. Halo-pelvic traction. How to reduce its dangers by simplifying its use[J]. Z Orthop Ihre Grenzgeb, 1974,112(2):351-354.
pmid: 4276749 |
| [22] |
Tredwell SJ, O’Brien JP. Avascular necrosis of the proximal end of the dens. A complication of halo-pelvic distraction[J]. J Bone Joint Surg Am, 1975,57(3):332-336.
pmid: 1123386 |
| [23] |
Tredwell SJ, O’Brien JP. Apophyseal joint degeneration in the cervical spine following halo-pelvic distraction[J]. Spine (Phila Pa 1976), 1980,5(6):497-501.
doi: 10.1097/00007632-198011000-00002 |
| [24] |
Dove J, Hsu LC, Yau AC. Spontaneous cervical spinal fusion. A complication of halo-pelvic traction[J]. Spine (Phila Pa 1976), 1981,6(1):45-48.
doi: 10.1097/00007632-198101000-00008 |
| [25] | Ransford AO, Manning CW. Halo-pelvic apparatus: peritoneal penetration by pelvic pins[J]. J Bone Joint Surg Br, 1978,60B(3):404-405. |
| [26] |
O’Brien JP, Yau AC, Smith TK, et al. Halo pelvic traction. A preliminary report on a method of external skeletal fixation for correcting deformities and maintaining fixation of the spine[J]. J Bone Joint Surg Br, 1971,53(2):217-229.
pmid: 5578217 |
| [1] | Jiajun LIU, Guokang LIU, Yuhu ZHU. Immune-related severe pneumonia: A case report [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 932-937. |
| [2] | Yifan CHEN,Zhongdi LIU,Peng ZHANG,Wei HUANG. Consistency of injury severity score in severe trauma patients [J]. Journal of Peking University (Health Sciences), 2024, 56(1): 157-160. |
| [3] | Zhan-peng SHANG,Yang YI,Rong YU,Jing-jing FAN,Yu-xi HUANG,Xue QIAO,Min YE. Bioactive compounds of Jingfang Granules against SARS-CoV-2 virus proteases 3CLpro and PLpro [J]. Journal of Peking University (Health Sciences), 2022, 54(5): 907-919. |
| [4] | Fu-zheng GUO,Xiu-juan ZHAO,Jiu-xu DENG,Zhe DU,Tian-bing WANG,Feng-xue ZHU. Early changes within the lymphocyte population are associated with the long term prognosis in severely injured patients [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 552-556. |
| [5] | Zhe DU,Wei HUANG,Zhi-wei WANG,Jing ZHOU,Jian XIONG,Ming LI,Peng ZHANG,Zhong-di LIU,Feng-xue ZHU,Chuan-lin WANG,Bao-guo JIANG,Tian-bing WANG. Application of multidisciplinary team (MDT) in the treatment of severe trauma [J]. Journal of Peking University (Health Sciences), 2020, 52(2): 298-301. |
| [6] | Yue YAN,Xian-e WANG,Ya-lin ZHAN,Li-li MIAO,Ye HAN,Chu-ren ZHANG,Zhao-guo YUE,Wen-jie HU,Jian-xia HOU. Clinical outcomes of ultrasonic subgingival debridement combined with manual root planing in severe periodontitis [J]. Journal of Peking University(Health Sciences), 2020, 52(1): 64-70. |
| [7] | Lei HOU,Guo-hua YE,Xiao-jing LIU,Zi-li LI. Evaluation of mandibular stability and condylar volume after orthognathic surgery in patients with severe temporomandibular joint osteoarthrosis [J]. Journal of Peking University(Health Sciences), 2020, 52(1): 113-118. |
| [8] | LI Yi, XU Li,ZHOU Yan-heng, OUYANG Xiang-ying, CAO Tian. Combination of periodontal, orthodontic and endodontic therapy in upper anterior teeth with hopeless prognosis and long-time follow-up: a case report [J]. Journal of Peking University(Health Sciences), 2017, 49(4): 740-744. |
|
||