Journal of Peking University (Health Sciences) ›› 2026, Vol. 58 ›› Issue (1): 214-219. doi: 10.19723/j.issn.1671-167X.2026.01.029
Previous Articles Next Articles
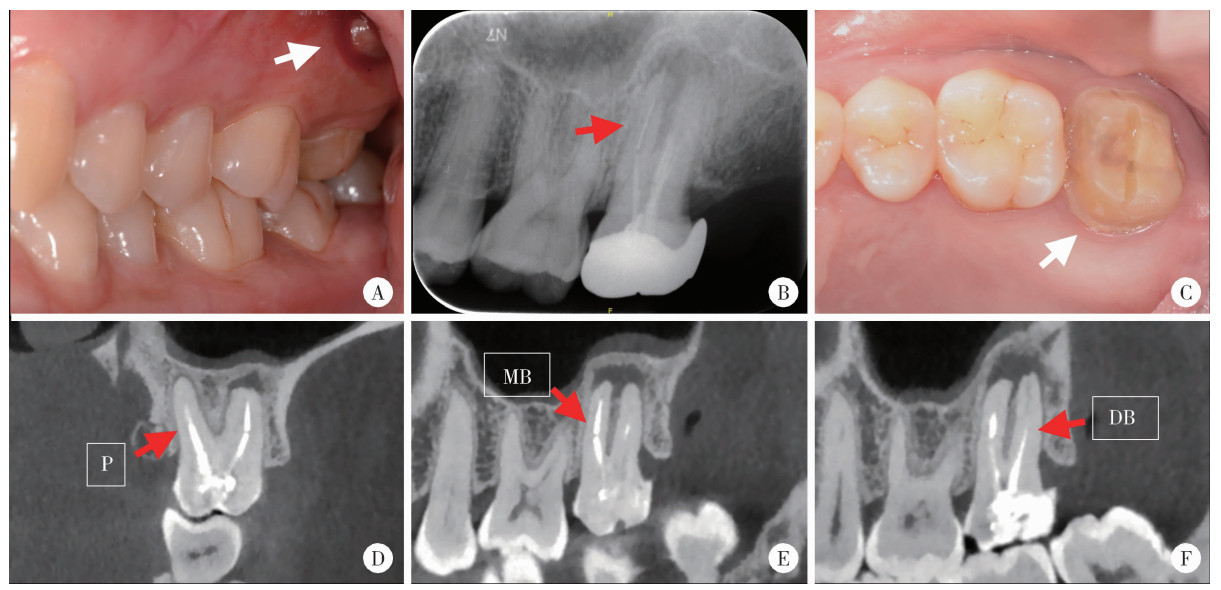
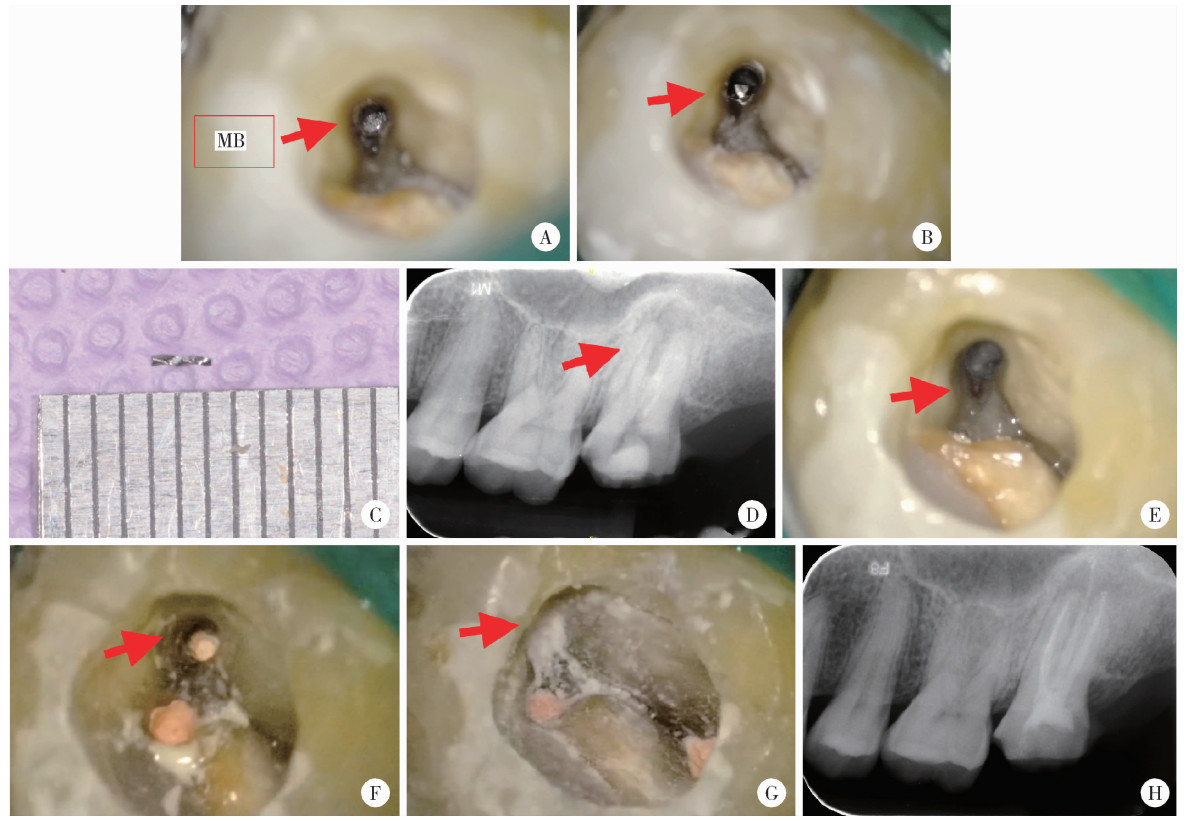
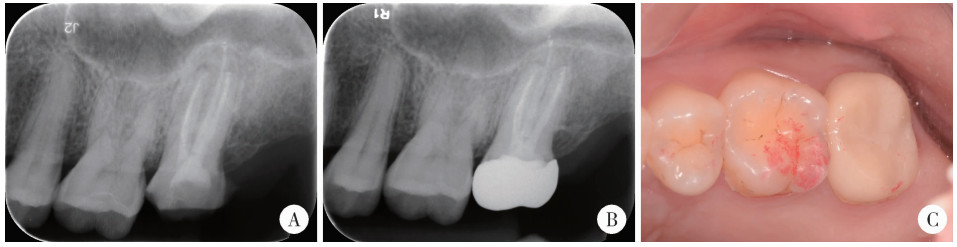
Endodontic retreatment of a maxillary second molar with chronic apical periodontitis and separated instrument: A case report
Hailing ZANG1, Yuhong LIANG2,*( )
)
- 1. Department of Stomatology, Peking University International Hospital, Beijing 102206, China
2. Department of Oral Emergency, Peking University School and Hospital of Stomatology & National Center for Stomatology & National Clinical Research Center for Oral Diseases & National Engineering Research Center of Oral Biomaterials and Digital Medical Devices & Beijing Key Laboratory of Digital Stomatology & NHC Research Center of Engineering and Technology for Computerized Dentistry & NMPA Key Laboratory for Dental Materials, Beijing 100081, China
CLC Number:
- R781.3


| 1 |
岳林, 王晓燕. 牙体牙髓病学[M]. 3版 北京: 北京大学医学出版社, 2022: 407.
|
| 2 |
doi: 10.1111/j.1365-2591.2011.01872.x |
| 3 |
|
| 4 |
doi: 10.1016/j.joen.2021.05.003 |
| 5 |
|
| 6 |
doi: 10.1038/s41368-025-00372-w |
| 7 |
doi: 10.1111/iej.13187 |
| 8 |
doi: 10.1016/j.joen.2020.08.011 |
| 9 |
doi: 10.1111/j.1365-2591.2009.01652.x |
| 10 |
doi: 10.1016/j.joen.2022.06.005 |
| 11 |
|
| 12 |
doi: 10.1111/iej.12148 |
| 13 |
梁宇红, 岳林. 锥形束CT在牙髓根尖周病诊治中的合理应用与思考[J]. 中华口腔医学杂志, 2019, 54 (9): 591- 597.
|
| 14 |
doi: 10.1016/j.joen.2012.12.033 |
| 15 |
doi: 10.1038/sj.bdj.2013.324 |
| 16 |
doi: 10.1097/01.don.0000164127.62864.7c |
| 17 |
doi: 10.1111/j.1365-2591.2004.00916.x |
| 18 |
doi: 10.1111/j.1365-2591.2003.00733.x |
| 19 |
doi: 10.1111/iej.13025 |
| 20 |
|
| 21 |
doi: 10.1007/s00784-023-05468-3 |
| 22 |
doi: 10.3390/bioengineering10030354 |
| 23 |
doi: 10.1007/s00784-021-03800-3 |
| [1] | XU Hao,ZHANG Guo-dong,FAN Guang-pu,CHEN Yu. Preoperative plasma predictive factors of new-onset atrial fibrillation after coronary artery bypass graft surgery: A propensity score matching study [J]. Journal of Peking University (Health Sciences), 2021, 53(6): 1139-1143. |
| [2] | YANG Yang,XIAO Feng,WANG Jin,SONG Bo,LI Xi-hui,ZHANG Shi-jie,HE Zhi-song,ZHANG Huan,YIN Ling. One-stage surgery in patients with both cardiac and non-cardiac diseases [J]. Journal of Peking University (Health Sciences), 2021, 53(2): 327-331. |
| [3] | Zhi-feng XU,Yun-peng LING,Zhong-qi CUI,hong ZHAO,Yi-chen GONG,Yuan-hao FU,Hang YANG,Feng WAN. Feasibility and safety of minimally invasive cardiac coronary artery bypass grafting surgery for patients with multivessel coronary artery disease: Early outcome and short-mid-term follow up results [J]. Journal of Peking University (Health Sciences), 2020, 52(5): 863-869. |
| [4] | Wen-qiang SUN,Zhou ZHAO,Qing GAO,Zeng-qiang HAN,Wei YANG,Bo LIAN,Gang LIU,Sheng-long CHEN,Yu CHEN. Effects of intraoperative graft flow measurements on the early mid-term outcomes after off-pump coronary artery bypass grafting [J]. Journal of Peking University(Health Sciences), 2019, 51(5): 851-855. |
| [5] | ZHANG Lu-feng, LING Yun-peng, YANG Hang, GONG Yi-chen, SONG Zhi-ming, WAN Feng. Comparison of outcomes of two minimally invasive approaches for multi-vessel coronary revascularization [J]. Journal of Peking University(Health Sciences), 2017, 49(6): 1066-1070. |
| [6] | LI Xi-hui, XIAO Feng, ZHANG Si-yu. Investigation of risk factors of acute kidney injury after off-pump coronary artery bypass grafting and 3 years’ follow-up [J]. Journal of Peking University(Health Sciences), 2017, 49(1): 131-136. |
| [7] | YU Jie, WAN Feng, XIE Ji-yan, WU Song, CUI Zhong-qi, XU Min, ZHANG Zhe, GAO Wei. Role of EuroSCORE and SinoSCORE in prediction of early postoperative quality of life in patients after coronary artery bypass surgery [J]. Journal of Peking University(Health Sciences), 2015, 47(5): 769-773. |
|
||