Journal of Peking University(Health Sciences) ›› 2019, Vol. 51 ›› Issue (6): 1096-1102. doi: 10.19723/j.issn.1671-167X.2019.06.021
Previous Articles Next Articles
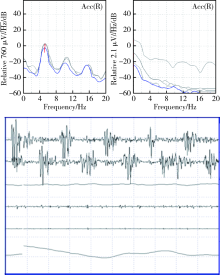
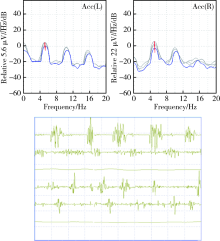
Diagnostic value of tremor analysis in identifying the early Parkinson’s syndrome
Xiao-xuan LIU,Shuo ZHANG,Na LIU,A-ping SUN,Ying-shuang ZHANG,Dong-sheng FAN( )
)
- Department of Neurology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R742.5




| [1] | Thenganatt MA, Jankovic J . Parkinson disease subtypes[J]. JAMA Neurol, 2014,71(4):499-504. |
| [2] | 中华医学会神经病学分会帕金森病及运动障碍学组. 中国帕金森病的诊断标准(2016 年)[J]. 中华神经科杂志, 2016,49(4):268-271. |
| [3] | Postuma RB, Berg D, Stern M , et al. MDS clinical diagnostic criteria for Parkinson’s disease[J]. Mov Disord, 2015,30(12):1591-1601. |
| [4] | Arshad AR, Sulaiman SA, Saperi AA , et al. MicroRNAs and target genes as biomarkers for the diagnosis of early onset of Parkinson disease [J/OL]. Front Mol Neurosci , 2017, 10: 352. (2017-10-31). doi: 10.3389/fnmol.2017.00352. |
| [5] | Marras C, Chaudhuri KR . Nonmotor features of Parkinson’s disease subtypes[J]. Mov Disord, 2016,31(8):1095-1102. |
| [6] | Hess CW, Pullman SL. Tremor: clinical phenomenology and assessment techniques [J/OL]. Tremor Other Hyperkinet Mov (N Y), ( 2012 -06-28). doi: 10.7916/D8WM1C41. |
| [7] | Buijink AW, Contarino MF, Koelman JH , et al. How to tackle tremor-systematic review of the literature and diagnostic work-up [J/OL]. Front Neurol, 2012, 3: 146. ( 2012-10-23). doi: 10.3389/fneur.2012.00146. |
| [8] | 杨硕, 潘华, 简凡 , 等. 帕金森病与多系统萎缩P型震颤峰频率、功率及谐波研究[J]. 中华神经科杂志, 2017,50(9):650-654. |
| [9] | Berg D, Roggendoff W, Schroder U , et al. Echogenicity of the substantia nigra: association with increased iron content and mar-ker for susceptibility to nigrostriatal injury[J]. Arch Neurol, 2002,59(6):999-1005. |
| [10] | Schrag A, Horsfall L, Walters K , et al. Prediagnostic presentations of Parkinson’s disease in primary care: a case-control study[J]. Lancet Neurol, 2015,14(1):57-64. |
| [11] | Lawton M, Ben-Shlomo Y, May MT , et al. Developing and validating Parkinson’s disease subtypes and their motor and cognitive progression[J]. J Neurol Neurosurg Psychiatry, 2018,89(12):1279-1287. |
| [12] | Rahimi F, Bee C, Wang D , et al. Subgroup analysis of PD tremor with loading: action tremor as a combination of classical rest and physiological tremor[J]. Clin Biomech (Bristol, Avon), 2015,30(2):114-120. |
| [13] | Abdullah R, Basak I, Patil KS , et al. Parkinson’s disease and age: The obvious but largely unexplored link[J]. Exp Gerontol, 2015,68:33-38. |
| [14] | 冯涛, 陈李 . 早发型帕金森病及其基因研究进展[J]. 中华神经科杂志, 2015,48(8):729-731. |
| [15] | Duval C, Daneault JF, Hutchison WD , et al. A brain network model explaining tremor in Parkinson’s disease[J]. Neurobiol Dis, 2016,85:49-59. |
| [16] | Levin J, Kurz A, Arzberger T , et al. The differential diagnosis and treatment of atypical Parkinsonism[J]. Dtsch Arztebl Int, 2016,113(5):61-69. |
| [17] | Becker G, Seufert J, Bogdahn U , et al. Degeneration of substantia nigra in chronic Parkinson’s disease visualized by transcranial color-coded real-time sonography[J]. Neurology, 1995,45(1):182-184. |
| [18] | Gaenslen A, Unmuth B, Godau J , et al. The specificity and sensitivity of transcranial ultrasound in the differential diagnosis of Parkinson’s disease: a prospective blinded study[J]. Lancet Neurol, 2008,7(5):417-424. |
| [19] | Shafieesabet A, Fereshtehnejad SM, Shafieesabet A , et al. Hyperechogenicity of substantia nigra for differential diagnosis of Parkinson’s disease: A meta-analysis[J]. Parkinsonism Relat Disord, 2017,42:1-11. |
| [20] | Li DH, He YC, Liu J, et al. Diagnostic accuracy of transcranial sonography of the substantia nigra in parkinson’s disease: A systematic review and meta-analysis [J/OL]. Sci Rep, 2016, 6: 20863. ( 2016-02-16). doi: 10.1038/srep20863. |
| [21] | 王宏利, 樊东升, 刘娜 , 等. 肌萎缩侧索硬化患者的中脑超声临床研究[J]. 中华神经科杂志, 2016,49(9):678-681. |
| No related articles found! |
|
||