Journal of Peking University (Health Sciences) ›› 2020, Vol. 52 ›› Issue (5): 828-835. doi: 10.19723/j.issn.1671-167X.2020.05.006
Previous Articles Next Articles
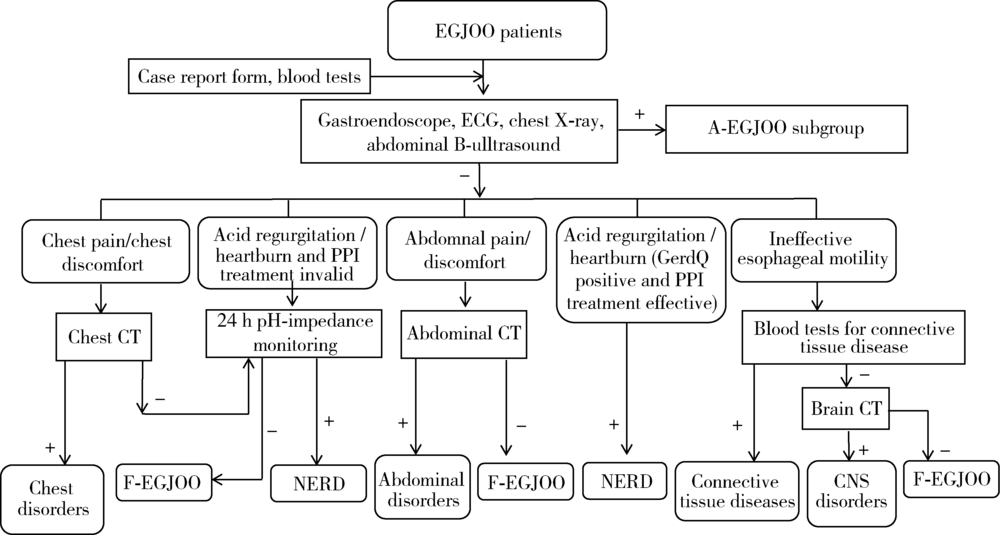
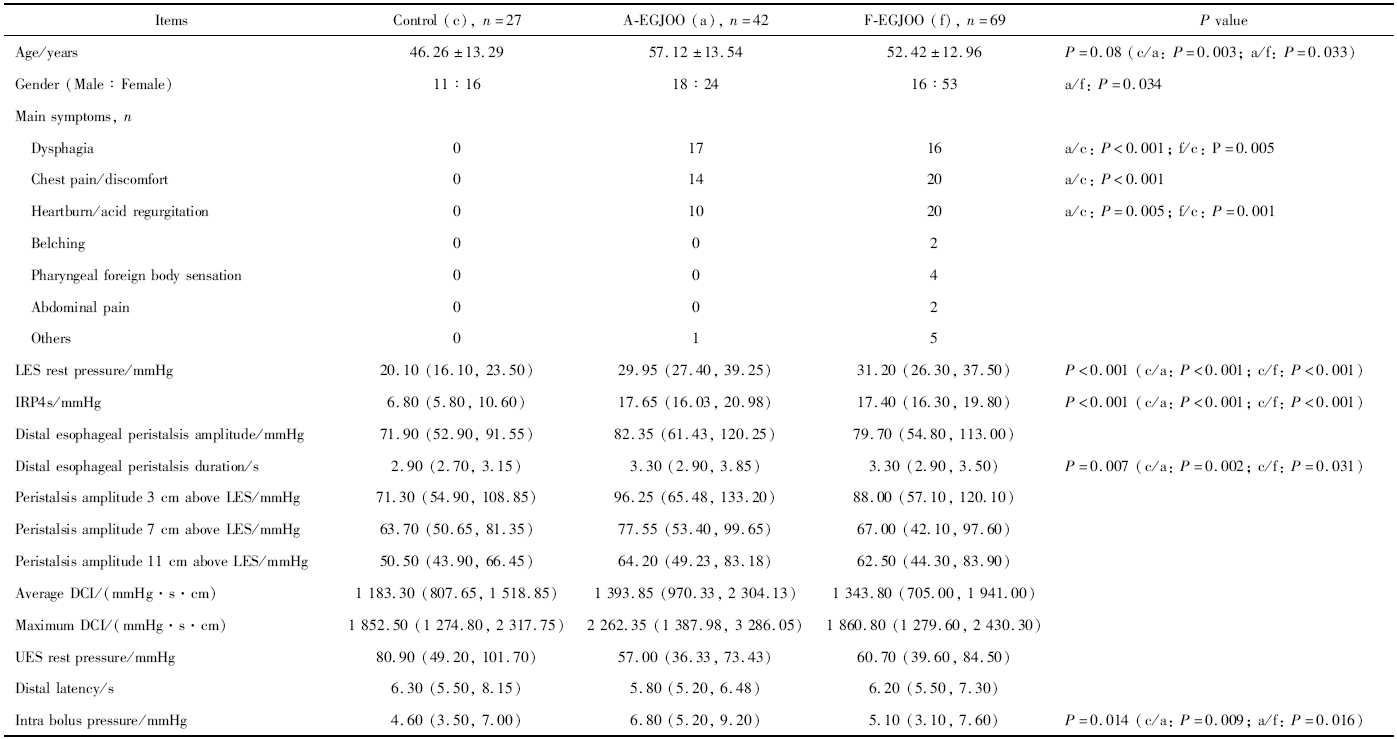
Study of etiology and esophageal motility characteristics of esophagogastric junction outlet obstruction patients
Kun WANG,Zhi-jie XU,Ying GE,Zhi-wei XIA,Li-ping DUAN( )
)
- Department of Gastroenterology, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R571


| [1] |
Kahrilas PJ, Bredenoord AJ, Fox M, et al. The Chicago classification of esophageal motility disorder, v3.0[J]. Neurogastroenterol Motil, 2015,27(2):160-174.
doi: 10.1111/nmo.12477 pmid: 25469569 |
| [2] |
Clayton SB, Patel R, Richter JE. Functional and anatomic eso-phagogastic junction outflow obstruction: Manometry, timed barium esophagram findings, and treatment outcomes[J]. Clin Gastroenterol Hepatol, 2016,14(6):907-911.
doi: 10.1016/j.cgh.2015.12.041 pmid: 26792374 |
| [3] | Shin IS, Min YW, Rhee PL. Esophagogastric junction outflow obstruction transformed to type Ⅱ achalasia[J]. J Neurogastorne-terol Motil, 2016,22(2):344-345. |
| [4] |
Ihara E, Muta K, Fukaura K, et al. Diagnosis and treatment strategy of Achalasia subtypes and esophagogastric junction outflow obstruction based on high-resolution manometry[J]. Digestion, 2017,95(1):29-35.
doi: 10.1159/000452354 pmid: 28052278 |
| [5] |
Kim HP, Vance RB, Shaheen NJ, et al. The prevalence and diagnostic utility of endoscopic features of eosinophilic esophagitis: A meta-analysis[J]. Clin Gastroenterol Hepatol, 2012,10(9):988-996.
doi: 10.1016/j.cgh.2012.04.019 pmid: 22610003 |
| [6] |
Armstrong D, Bennett JR, Blum AL, et al. The endoscopic assessment of esophagitis: a progress report on observer agreement[J]. Gastroenterology, 1996,111(1):85-92.
doi: 10.1053/gast.1996.v111.pm8698230 pmid: 8698230 |
| [7] | Zerbib F, Des Varannea SB, Roman S, et al. Normal values and day-to-day variability of 24-h-ambulatory oesophageal impedance pH monitoring in a Belgian-French cohort of healthy subjects[J]. Aliment Pha rmacol Ther, 2005,22(10):1011-1021. |
| [8] |
Samo S, Qayed E. Esophagogastric junction outflow obstruction: Where are we now in diagnosis and management?[J]. World J Gastroenterol, 2019,25(4):411-417.
doi: 10.3748/wjg.v25.i4.411 pmid: 30700938 |
| [9] |
Pérez-Fernández MT, Santander C, Marinero A, et al. Characte-rization and follow-up of esophagogastric junction outflow obstruction detected by high resolution manometry[J]. Neurogastroenterol Motil, 2016,28(1):116-126.
pmid: 26517978 |
| [10] | Schupack D, Katzka DA, Geno DM, et al. The clinical significance of esophagogastric junction outflow obstruction and hypercontractile esophagus in high resolution esophageal manometry[J]. Neruogastroenterol Motil, 2017,29(10):1-9. |
| [11] |
Ong AML, Namasivayam V, Wang YT. Evaluation of symptomatic esophagogastric junction outflow obstruction[J]. J Gastroenterol Hepatol, 2018,33(10):1745-1750.
doi: 10.1111/jgh.14155 pmid: 29660156 |
| [12] |
Gyawali CP, Kushnir VM. High-resolution manometric characte-ristics help differentiate types of distal esophageal obstruction in patients with peristalsis[J]. Neurogastroenterol Motil, 2011,23(6):502-508, e197.
pmid: 21303431 |
| [13] | 王琨, 段丽萍, 夏志伟, 等. 基于高分辨食管压力测定及阻抗-pH监测的难治性烧心患者食管动力特点[J]. 中华医学杂志, 2014,94(34):2650-2655. |
| [1] | Weihua HOU, Shujie SONG, Zhongyue SHI, Lu LIU, Mulan JIN. Neuroendocrine carcinoma with significantly vacuolar nucleus at the esophagogastric junction: A case report [J]. Journal of Peking University (Health Sciences), 2025, 57(5): 1005-1009. |
|
||