Journal of Peking University (Health Sciences) ›› 2024, Vol. 56 ›› Issue (6): 1101-1105. doi: 10.19723/j.issn.1671-167X.2024.06.025
Previous Articles Next Articles
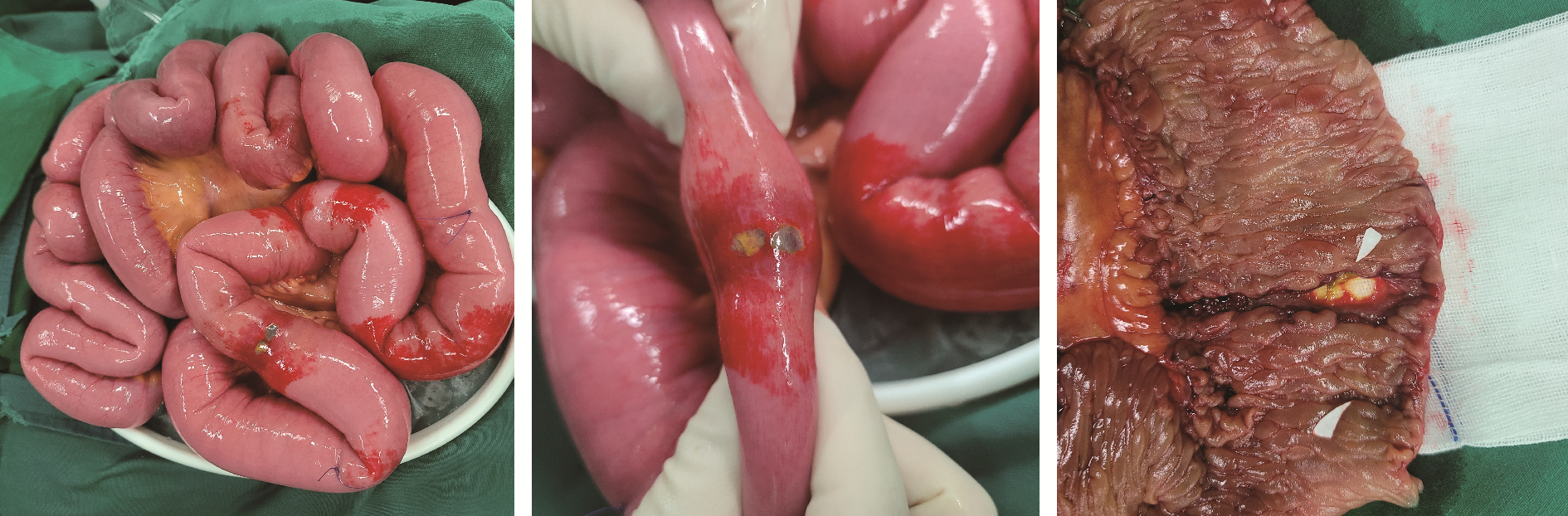
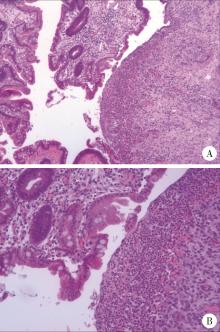
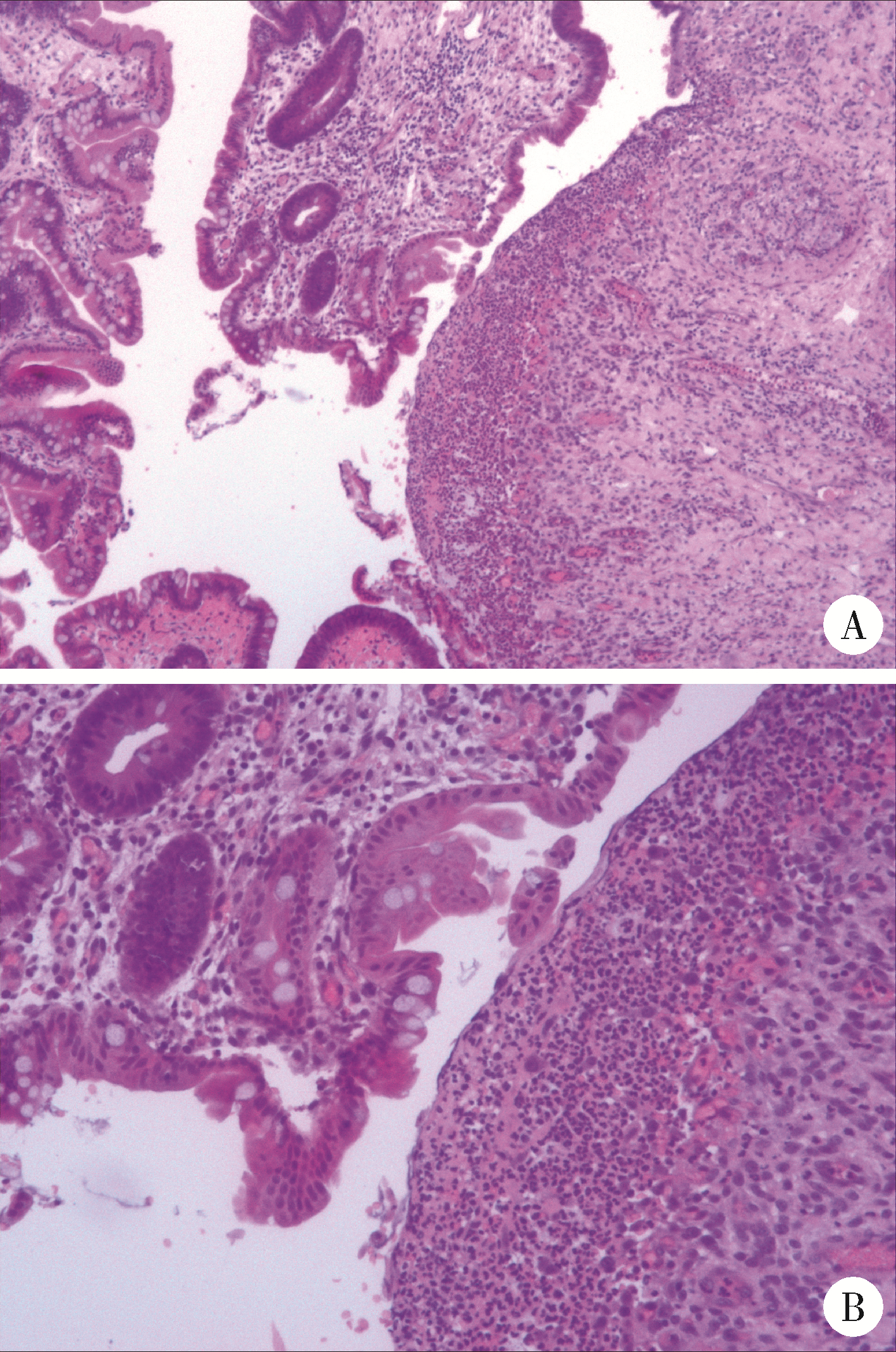
IgA vasculitis with necrosis of the small intestine secondary to monoclonal gammopathy of renal significance: A case report
Yan DING1, Chaoran LI1, Wensheng HUANG2, Linzhong ZHU3, Lifang WANG1, Doudou MA1, Juan ZHANG4, Lianjie SHI1,*( )
)
- 1. Department of Rheumatology and Immunology, Peking University Shougang Hospital, Beijing 100144, China
2. Department of Gastrointestinal Surgey, Peking University Shougang Hospital, Beijing 100144, China
3. Department of Interventional Medicine, Peking University Shougang Hospital, Beijing 100144, China
4. Department of Gastroneterology, Peking University Shougang Hospital, Beijing 100144, China
CLC Number:
- R593.2





| 1 |
Rajkumar SV , Dimopoulos MA , Palumbo A , et al. International myeloma working group updated criteria for the diagnosis of multiple myeloma[J]. Lancet Oncol, 2014, 15 (12): e538- e548.
doi: 10.1016/S1470-2045(14)70442-5 |
| 2 | 关艾, 沈恺妮, 张路, 等. 意义未明的单克隆丙种球蛋白血症的临床特征及疾病进展相关因素分析[J]. 中华血液学杂志, 2023, 44 (2): 137- 140. |
| 3 | 饶向荣. 具有肾脏意义的单克隆免疫球蛋白血症的诊治[J]. 中华肾病研究电子杂志, 2017, 6 (5): 208- 213. |
| 4 |
Song Y , Huang X , Yu G , et al. Pathogenesis of IgA vasculitis: An up-to-date review[J]. Front Immunol, 2021, 12, 771619.
doi: 10.3389/fimmu.2021.771619 |
| 5 |
Ozen S , Pistorio A , Iusan SM , et al. EULAR/PRINTO/PRES criteria for Henoch-Schönlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: Ankara 2008. Part Ⅱ: Final classification criteria[J]. Ann Rheum Dis, 2010, 69 (5): 798- 806.
doi: 10.1136/ard.2009.116657 |
| 6 |
Audemard-Verger A , Pillebout E , Amoura Z , et al. Gastrointestinal involvement in adult IgA vasculitis (Henoch-Schönlein purpura): Updated picture from a French multicentre and retrospective series of 260 cases[J]. Rheumatology (Oxford), 2020, 59 (10): 3050- 3057.
doi: 10.1093/rheumatology/keaa104 |
| 7 |
Mills JA , Michel BA , Bloch DA , et al. The American College of Rheumatology 1990 criteria for the classification of Henoch-Schönlein purpura[J]. Arthritis Rheum, 1990, 33 (8): 1114- 1121.
doi: 10.1002/art.1780330809 |
| 8 |
Jennette JC , Falk RJ , Bacon PA , et al. 2012 revised international chapel hill consensus conference nomenclature of vasculitides[J]. Arthritis Rheum, 2013, 65 (1): 1- 11.
doi: 10.1002/art.37715 |
| 9 |
Leung N , Bridoux F , Batuman V , et al. The evaluation of monoclonal gammopathy of renal significance: A consensus report of the international kidney and monoclonal gammopathy research group[J]. Nat Rev Nephrol, 2019, 15 (1): 45- 59.
doi: 10.1038/s41581-018-0077-4 |
| 10 |
Gozzetti A , Guarnieri A , Zamagni E , et al. Monoclonal gammopathy of renal significance (MGRS): Real-world data on outcomes and prognostic factors[J]. Am J Hematol, 2022, 97 (7): 877- 884.
doi: 10.1002/ajh.26566 |
| 11 |
Hočevar A , TomšičM , Jurčić V , et al. Predicting gastrointestinal and renal involvement in adult IgA vasculitis[J]. Arthritis Res Ther, 2019, 21 (1): 302.
doi: 10.1186/s13075-019-2089-2 |
| 12 | Rousset L , Cordoliani F , Battistella M , et al. Vasculitis and IgA monoclonal gammopathy of cutaneous significance[J]. J Eur Acad Dermatol Venereol, 2018, 32 (5): e175- e176. |
| 13 |
Lipsker D . Monoclonal gammopathy of cutaneous significance: Review of a relevant concept[J]. J Eur Acad Dermatol Venereol, 2017, 31 (1): 45- 52.
doi: 10.1111/jdv.13847 |
| 14 |
Umemura H , Yamasaki O , Iwatsuki K . Leukocytoclastic vasculitis associated with immunoglobulin A lambda monoclonal gammopathy of undetermined significance: A case report and review of previously reported cases[J]. J Dermatol, 2018, 45 (8): 1009- 1012.
doi: 10.1111/1346-8138.14466 |
| 15 |
Vignon M , Cohen C , Faguer S , et al. The clinicopathologic characteristics of kidney diseases related to monotypic IgA deposits[J]. Kidney Int, 2017, 91 (3): 720- 728.
doi: 10.1016/j.kint.2016.10.026 |
| 16 |
Hankard A , Ingen-Housz-Oro S , El Karoui K , et al. IgA vasculitis with underlying monoclonal IgA gammopathy: Innovative therapeutic approach targeting plasma cells. A case series[J]. Clin Rheumatol, 2022, 41 (10): 3119- 3123.
doi: 10.1007/s10067-022-06181-4 |
| [1] | Handong DING, Qin WANG, Guiyi LIAO, Zongyao HAO. Diagnosis and treatment of gastrointestinal bleeding after kidney transplantation [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 902-907. |
| [2] | Jing XU,Jing XU,He LI,Jie TANG,Jian-long SHU,Jing ZHANG,Lian-jie SHI,Sheng-guang LI. Dermatomyositis combined with IgA vasculitis: A case report [J]. Journal of Peking University(Health Sciences), 2019, 51(6): 1173-1177. |
|
||