Journal of Peking University (Health Sciences) ›› 2020, Vol. 52 ›› Issue (4): 780-784. doi: 10.19723/j.issn.1671-167X.2020.04.033
Previous Articles Next Articles
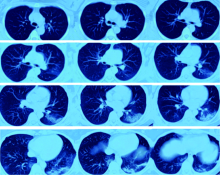
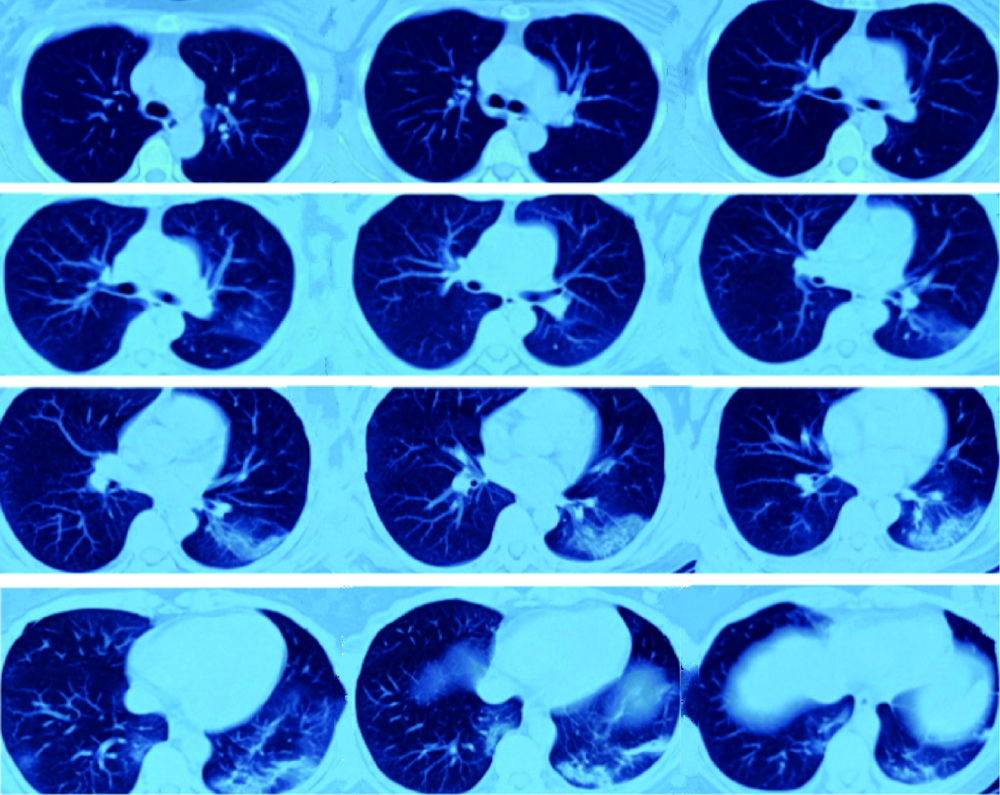
Severe acute respiratory syndrome coronavirus 2 infection in renal transplant recipients: A case report
Qiu-yu LI1,Qin CHENG1,Zhi-ling ZHAO2,Ni-ni DAI1,Lin ZENG3,Lan ZHU4,Wei GUO5,Chao LI2,Jun-hong WANG6,Shu LI6,Qing-gang GE2,Ning SHEN1,△( )
)
- 1. Department of Respiratory and Critical Care Medicine, Peking University Third Hospital, Beijing 100191, China
2. Department of Critical Care Medicine, Peking University Third Hospital, Beijing 100191, China
3. Research Center of Clinical Epidemiology, Peking University Third Hospital, Beijing 100191, China
4. Institute of Organ Transplantation, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430030, China
5. Department of Radiology, Peking University Third Hospital, Beijing 100191, China
6. Department of Emergency, Peking University Third Hospital, Beijing 100191, China
CLC Number:
- R563.1





| [1] |
Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study[J]. Lancet, 2020,395(10223):507-513.
pmid: 32007143 |
| [2] | Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients[J]. Am J Transplant, 2009,9(Suppl 3):S1-155. |
| [3] |
Kumar D, Michaels MG, Morris MI, et al. Outcomes from pandemic influenza A H1N1 infection in recipients of solid-organ transplants: a multicentre cohort study[J]. Lancet Infect Dis, 2010,10(8):521-526.
pmid: 20620116 |
| [4] | Zhang H, Chen Y, Yuan Q, et al. Identification of kidney transplant recipients with coronavirus disease 2019[J]. Eur Urol, 2020,77(6):742-747. |
| [5] | Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China[J]. JAMA, 2020,323(11):1061-1069. |
| [6] | Lansbury L, Rodrigo C, Leonardi-Bee J, et al. Corticosteroids as adjunctive therapy in the treatment of influenza [J]. Cochrane Database Syst Rev, 2019, 2(2): CD010406. |
| [7] |
Russell CD, Millar JE, Baillie JK. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury[J]. Lancet, 2020,395(10223):473-475.
pmid: 32043983 |
| [1] | Yayun ZHAO, Mengfan NI, Xue LI, Bei WANG, Gong CHENG, Jing HE, Yuebo JIN. Clinical efficacy and safety of rituximab in treating renal injury in primary Sjögren syndrome [J]. Journal of Peking University (Health Sciences), 2025, 57(6): 1051-1060. |
| [2] | Zhao ZHAO, Weiyu ZHANG, Wenbo YANG, Yongjie ZHANG, Xiaopeng ZHANG, Huiying ZHAO, Gang ZHOU, Qiang WANG. Kidney transplantation in low-age, low-weight children: A report of two cases [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 803-807. |
| [3] | Qiming ZHANG, Zebo CHEN, Yu TIAN, Dameng PAN, Lei LIU, Hongxian ZHANG, Lei ZHAO, Shudong ZHANG, Lulin MA, Xiaofei HOU. Experience summary of robot-assisted laparoscopic transplant nephrectomy [J]. Journal of Peking University (Health Sciences), 2025, 57(4): 666-669. |
| [4] | Handong DING, Qin WANG, Guiyi LIAO, Zongyao HAO. Diagnosis and treatment of gastrointestinal bleeding after kidney transplantation [J]. Journal of Peking University (Health Sciences), 2024, 56(5): 902-907. |
| [5] | Wenbo YANG,Lei YU,Weiyu ZHANG,Tao XU,Qiang WANG. Effect and safety of self-draining ureteral stent with thread in kidney transplant reci-pients [J]. Journal of Peking University (Health Sciences), 2024, 56(4): 656-660. |
| [6] | Jin-hui LAI,Qi WANG,Jia-xiang JI,Ming-rui WANG,Xin-wei TANG,Ke-xin XU,Tao XU,Hao HU. Effects of delayed ureteral stents removal during the COVID-19 pandemic on the quality of life and psychological status of postoperative patients with urinary calculi [J]. Journal of Peking University (Health Sciences), 2023, 55(5): 857-864. |
| [7] | HONG Peng,TIAN Xiao-jun,ZHAO Xiao-yu,YANG Fei-long,LIU Zhuo,LU Min,ZHAO Lei,MA Lu-lin. Bilateral papillary renal cell carcinoma following kidney transplantation: A case report [J]. Journal of Peking University (Health Sciences), 2021, 53(4): 811-813. |
| [8] | Kai MA,Xing-ke QU,Qing-quan XU,Liu-lin XIONG,Xiong-jun YE,Li-zhe AN,Wei-nan CHEN,Xiao-bo HUANG. Endoscopic treatment for ureterovesical junction stenosis in patients with kidney transplantation: 13 cases report [J]. Journal of Peking University(Health Sciences), 2019, 51(6): 1155-1158. |
| [9] | ZHAO Lei, MA Lu-lin, ZHANG Hong-xian, HOU Xiao-fei, LIU Lei, FU Yan, KOU Yun-geng, SONG Yi-meng. Technical improvement in retroperitoneal laparoscopic living donor nephrectomy: report of 193 cases [J]. Journal of Peking University(Health Sciences), 2017, 49(5): 867-871. |
| [10] | ZHANG Hong-xian, ZHAO Lei, MA Lu-lin, HOU Xiao-fei, LIU Lei, DENG Shao-hui. Retroperitoneal laparoscopic nephrectomy with autotransplantation for severe iatrogenic ureteral injury [J]. Journal of Peking University(Health Sciences), 2016, 48(4): 622-626. |
| [11] | LIU Yu-Qing, LU Jian, ZHAO Lei, HOU Xiao-Fei, MA Lu-Lin. Prognostic factors for intravesical recurrence after surgery for upper tract urothelial carcinoma in renal transplant recipients [J]. Journal of Peking University(Health Sciences), 2015, 47(4): 605-610. |
| [12] | LIU Lei, MA Lu-Lin, ZHAO Lei, ZHANG Hong-Xian, HOU Xiao-Fei. Ureteral stricture following renal transplantation: risk factors and surgical management [J]. Journal of Peking University(Health Sciences), 2014, 46(4): 548-551. |
|
||