Journal of Peking University (Health Sciences) ›› 2023, Vol. 55 ›› Issue (4): 762-765. doi: 10.19723/j.issn.1671-167X.2023.04.032
Previous Articles Next Articles
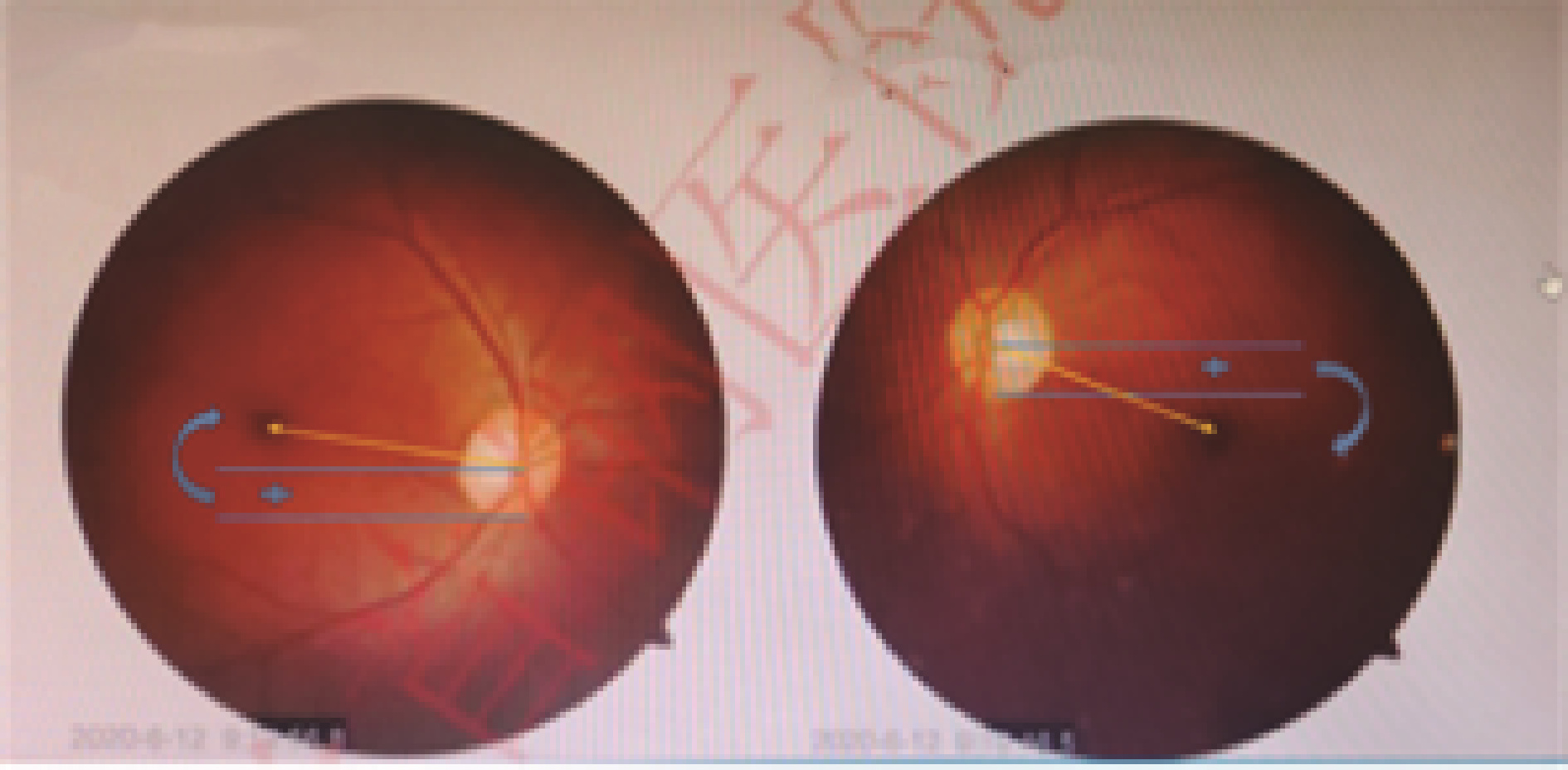
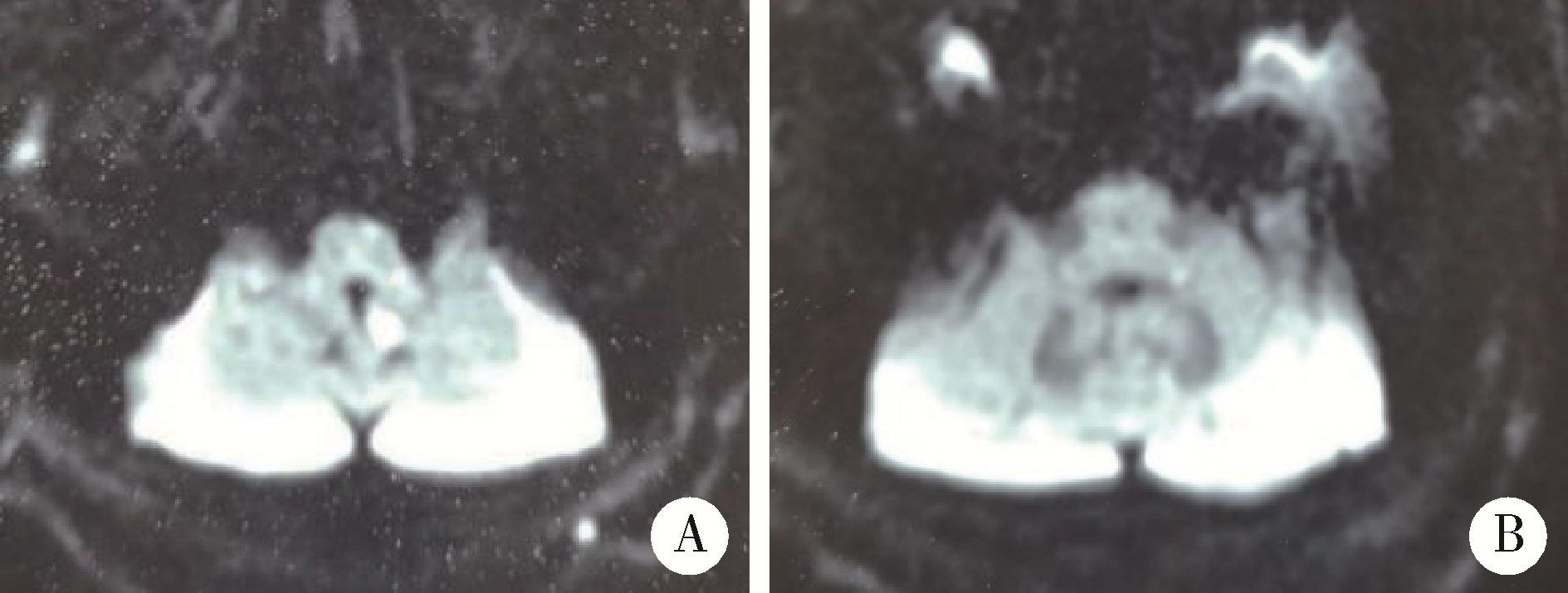
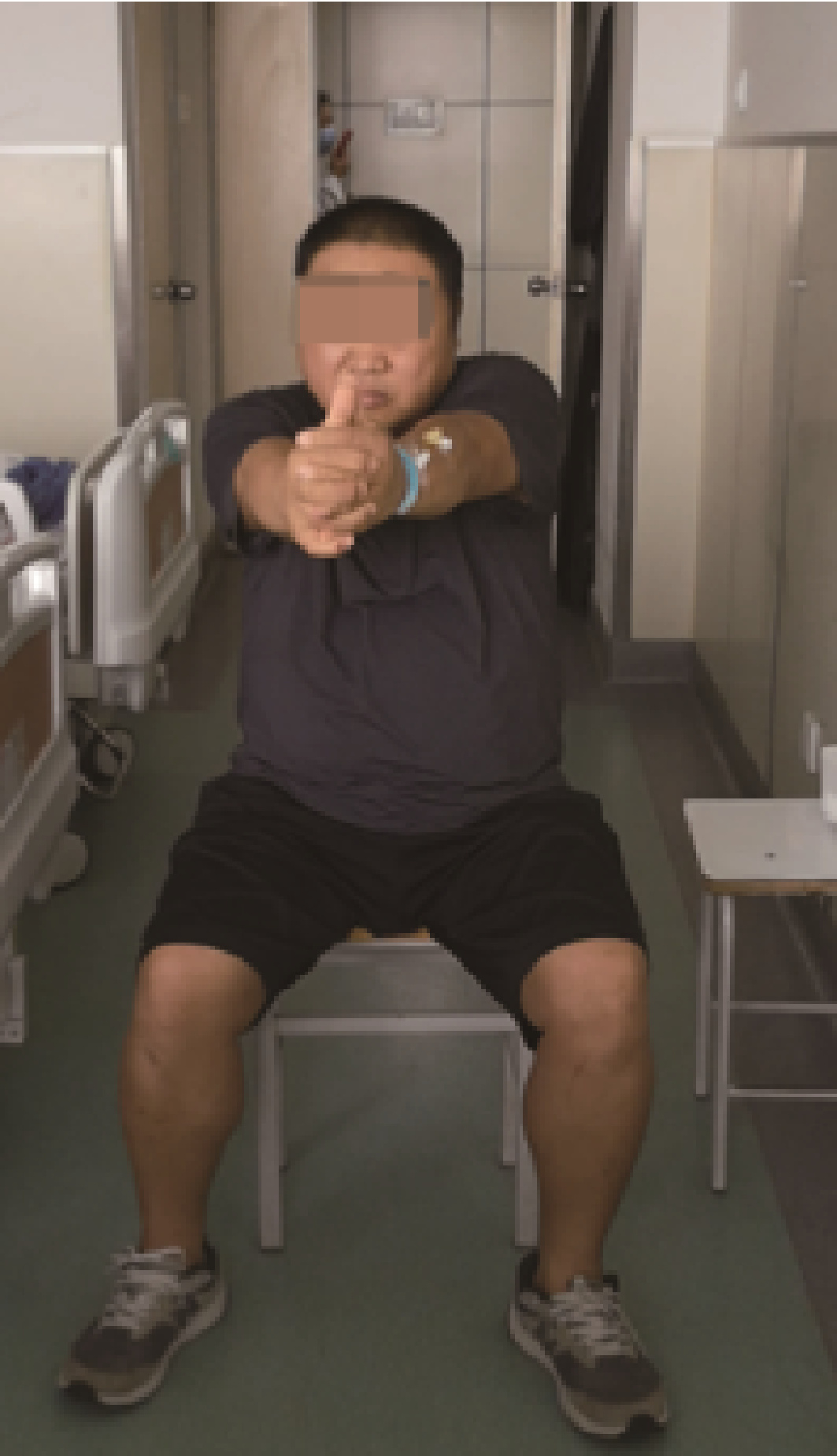
Posterior inferior cerebellar artery infarction with episodic postural diplopia as the initial symptom: A case report
Chang-feng FAN1,2,*( ),Ya-ping HUANG1,Xia LI1,Yun CHEN1,Zhen LI3,Shu-dong QIAO1
),Ya-ping HUANG1,Xia LI1,Yun CHEN1,Zhen LI3,Shu-dong QIAO1
- 1. Department of Neurology, Peking University Shougang Hospital, Beijing 100041, China
2. Department of Geriatrics, Peking University Shougang Hospital, Beijing 100041, China
3. Department of ophthalmology, Peking University Shougang Hospital, Beijing 100041, China
CLC Number:
- R743.3







| 1 | Brandt T , Strupp M , Dieterich M . Towards a concept of disorders of "higher vestibular function"[J]. Front Integr Neurosci, 2014, 2, 47. |
| 2 | 田军茹. 眩晕诊治[M]. 北京: 人民卫生出版社, 2015: 50- 52. |
| 3 |
Dieterich M , Brand T . Wallenberg's syndrome: Lateropulsion, cyclorotation, and subjective visual vertical in thirty-six patients[J]. Ann Neurol, 1992, 31 (4): 399- 408.
doi: 10.1002/ana.410310409 |
| 4 |
Dieterich M , Brandt T . Perception of verticality and vestibular disorders of balance and falls[J]. Front Neurol, 2019, 10, 172.
doi: 10.3389/fneur.2019.00172 |
| 5 |
Pergallo JH , Newman NJ . Diplopia-An Update[J]. Semin Neurol, 2016, 36 (4): 357- 361.
doi: 10.1055/s-0036-1585428 |
| 6 |
Rasool N , Prasad S . Teaching neuroimages: Upright-supine test to evaluate vertical diplopia[J]. Neurology, 2015, 84 (19): e153- e154.
doi: 10.1212/WNL.0000000000001569 |
| 7 |
Wong AMF . New understanding on the contribution of the central otolithic system to eye movement and skew deviation[J]. Eye (Lond), 2015, 29 (2): 153- 156.
doi: 10.1038/eye.2014.243 |
| 8 |
Wong AMF , Colpa L , Chandrakumar M . Ability of an upright-supine test to differentiate skew deviation from other vertical strabismus causes[J]. Arch Ophthalmol, 2011, 129 (12): 1570- 1575.
doi: 10.1001/archophthalmol.2011.335 |
| [1] | BAI Peng,WANG Tao,ZHOU Yang,TAO Li-yuan,LI Gang,LI Zheng-qian,GUO Xiang-yang. Effect of different shunt strategies on cerebral infarction after carotid endarterectomy [J]. Journal of Peking University (Health Sciences), 2021, 53(6): 1144-1151. |
|
||