
泌尿系统结石是常见的泌尿外科疾病,发病率高,我国平均每年因泌尿系统结石住院的患者约70万人,开展输尿管镜治疗的手术约30万例,手术5年增长率达18%[1]。输尿管镜碎石术是常用的输尿管结石手术方式,适用范围广,且能获得较满意的结石清除率[2]。然而,输尿管镜治疗结石引起的输尿管狭窄发生率为0.3%~4.9%[3],近2倍于没有接受输尿管镜治疗的结石患者[4]。输尿管狭窄可引起肾积水、反复泌尿系统感染及肾功能损害等。及时且合理的输尿管狭窄修复重建手术有机会从根本上解决输尿管狭窄,避免长期留置DJ管或肾造瘘管造成的困扰,改善患者生活质量[5]。本研究旨在总结北京大学第一医院泌尿外科结石相关输尿管狭窄的上尿路修复手术技术与临床结局,为结石相关输尿管狭窄的诊治提供参考。
1 资料与方法
1.1 病例选择
选择2014年3月至2023年11月于北京大学第一医院泌尿外科诊治的结石相关输尿管狭窄患者的病例资料进行回顾性分析,共纳入71例患者,其中,男性43例,女性28例。纳入标准:(1)输尿管镜碎石术中出现撕裂、撕脱或横断;(2)手术碎石治疗后出现症状或体征,影像学表现确认输尿管狭窄。排除标准:(1)其他原因导致输尿管狭窄者;(2)未接受手术治疗者;(3)临床及影像数据不完整者;(4)心肺功能不全等内科疾病不能耐受手术者。接受多次手术的重复病例按北京大学第一医院泌尿外科首次采用的治疗方式计入本研究,本研究开始前已经北京大学第一医院伦理委员会审查批准(2024研521)。
1.2 数据收集与随访
自北京大学第一医院泌尿外科上尿路修复(reconstruction of urinary tract: technology, epidemiology, and result, RECUTTER)数据库收集患者基线特征、泌尿系统结石病史、血肌酐、影像学检查、围手术期数据、并发症和随访情况。常规术前影像学评估包括泌尿系统超声、泌尿系统增强计算机体层成像尿路造影(computed tomography urography, CTU)、顺/逆行输尿管造影和利尿肾动态显像,肾积水严重者需留置经皮肾穿刺造瘘管引流。术前输尿管狭窄长度定义为顺/逆行输尿管造影检查无造影剂通过或管壁僵硬部分长度。术中输尿管狭窄长度通过带有刻度的输尿管导管进行测量,判断困难者可术中联合吲哚菁绿明确输尿管狭窄段。根据Clavien-Dindo分级标准对围手术期并发症进行分级。手术成功定义为术后肾积水程度改善或未再加重、肾功能处于正常范围且保持稳定。术后第一年每3个月对患者进行一次随访,此后每6个月至少随访一次。每次随访完成症状评估、体格检查、尿常规、血常规、血肌酐和泌尿系统超声。术后每6个月复查CTU。对于回肠代输尿管术后患者,还需要定期完善血气分析。
1.3 统计学分析
使用SPSS 26.0软件,正态分布的连续变量以${\bar x}$±s表示,非正态分布的连续变量以M(min~max)表示,分类变量以n(%)表示。Kolmogorov-Smirnov检验用于检查变量是否符合正态分布。正态分布的连续变量手术前后对比采用配对t检验,双侧检验,P < 0.05认为差异有统计学意义。
2 结果
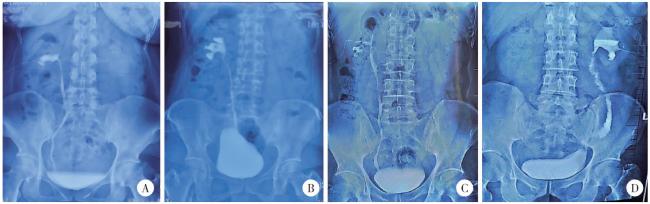
患者中位年龄56(18~74)岁。所有患者中,左侧和右侧输尿管狭窄各有35例,另有1例双侧狭窄。上段输尿管狭窄的患者最多(36/71, 50.7%),其次是下段输尿管狭窄(15/71,21.1%)和中段输尿管狭窄(9/71, 12.7%),另有11例(15.5%)患者为多发输尿管狭窄(图 1)。术前影像学测得中位输尿管狭窄长度为5.0(3.0~15.0) cm。术前最常见的症状是腰痛(28/71, 39.4%),其次是发热(19/71, 26.8%)、尿路刺激症状(5/71, 7.0%)、恶心(5/71, 7.0%)和血尿(3/71, 4.2%),另有24例患者(33.8%)无明显症状。术前超声检查显示积水程度轻度20例(28.2%)、中度24例(33.8%)、重度20例(28.2%),另有7例(9.9%)患者于北京大学第一医院泌尿外科就诊前已留置肾造瘘管,超声显示无积水。引流方式方面,9例患者曾留置输尿管支架管,35例患者接受肾造瘘置管,16例患者既有输尿管支架管留置病史,也曾留置肾造瘘管。10(14.1%)例患者曾接受球囊扩张或输尿管镜扩张等腔内治疗,13例(18.3%)患者曾接受修复重建手术。术前平均血肌酐(91.29±23.46) μmoL/L,平均估算肾小球滤过率(estimated glomerular filtration rate,eGFR)(82.19±19.97) mL/(min·1.73 m2)。

手术治疗方式及围术期数据见表 1,术中中位输尿管狭窄长度为5.0(3.0~15.0) cm,中位手术时间为186.0(141.5~223.0) min,中位出血量30(20~50) mL, 中位术后住院天数6.0(4.0~7.5) d。根据输尿管狭窄的位置及长度选择不同的修复重建策略(表 2)。自体补片输尿管成形术(21/36, 58.3%)是治疗上段输尿管狭窄最常用的方式(口腔黏膜13例,阑尾8例)。下段输尿管狭窄患者中最常用的术式为输尿管膀胱再植术(10/15, 66.7%), 其中8例联合膀胱瓣技术。中段输尿管狭窄的治疗复杂,常规治疗包括输尿管端端吻合术(1/9, 11.1%), 阑尾补片输尿管成形术(1/9, 11.1%),口腔黏膜补片输尿管成形术(2/9, 22.2%),1例患者因术中发现输尿管狭窄长度超过术前评估,手术方式术中由舌黏膜补片输尿管成形术改为回肠代输尿管术。上、中、下段输尿管短段狭窄接受输尿管镜球囊扩张术分别为1、1、2例。此外,上、中、下段输尿管狭窄分别有7、4、3例患者因狭窄长度过长或撕脱行回肠代输尿管术。另有11例结石相关多发输尿管狭窄的患者均接受回肠代输尿管术。
表1 患者手术方式与围手术期数据Table 1 Surgical methods and perioperative data of the patients |
| Operation | Operation time/min | Estimated blood loss/mL | Postoperative hospitalization days/d | Follow up/months |
| Total | 186.0 (21.0-372.0) | 30.0 (0-1 000.0) | 6.0 (2.0-18.0) | 14.2 (6.1-107.1) |
| Ureteroureterostomy | 145.0 (129.0-155.0) | 20.0 (5.0-30.0) | 5.0 (3.0-6.0) | 12.1 (6.6-45.7) |
| Pyeloplasty | 176.0 (113.0-198.0) | 20.0 (20.0-20.0) | 7.0 (4.0-7.0) | 19.8 (12.8-20.6) |
| Ureteral reimplantation | 122.5 (92.0-219.0) | 20.0 (0-70.0) | 4.0 (3.0-6.0) | 8.9 (6.3-22.3) |
| Appendiceal graft ureteroplasty | 168.0 (131.0-276.0) | 30.0 (10.0-100.0) | 6.0 (4.0-10.0) | 20.2 (6.8-35.6) |
| Oral graft ureteroplasty | 170.0 (130.0-270.0) | 30.0 (10.0-200.0) | 5.0 (4.0-8.0) | 10.0 (6.1-37.7) |
| Ileal ureter | 230.0 (170.0-372.0) | 50.0 (10.0-1 000.0) | 9.5 (5.0-18.0) | 19.6 (6.4-107.1) |
| Balloon dilation | 70.0 (21.0-82.0) | 0 (0-0) | 2.0 (2.0-3.0) | 56.5 (13.7-92.1) |
Data were M(min-max). |
表2 修复策略及临床结局Table 2 Reconstructive strategies and clinical outcomes |
| Operation | n | Location | Length of stricture/cm, M(min-max) | |||||||||
| Upper | Middle | Lower | Long/Multiple | |||||||||
| Ureteroureterostomy | 5 | 4 | 1 | 0 | 0 | 2.0 (1.0-3.0) | ||||||
| Pyeloplasty | 3 | 3 | 0 | 0 | 0 | 1.0 (1.0-3.0) | ||||||
| Ureteral reimplantation | 10 | 0 | 0 | 10 | 0 | 5.0 (4.0-10.0) | ||||||
| Appendiceal graft ureteroplasty | 9 | 8 | 1 | 0 | 0 | 4.0 (2.5-5.5) | ||||||
| Oral graft ureteroplasty | 15 | 13 | 2 | 0 | 0 | 3.0 (2.0-5.0) | ||||||
| Ileal ureter replacement | 25 | 7 | 4 | 3 | 11 | 19.0 (4.5-30.0) | ||||||
| Balloon dilation | 4 | 1 | 1 | 2 | 0 | 0.75 (0.5-1.0) | ||||||
| Operation | Symptoms* | Degree of hydronephrosis | Renal function | Success rate/% | ||||||||
| Complete relief | Partial relief | Cured | Improved | Stable | Aggravated | Improved | Stable | Aggravated | ||||
| Ureteroureterostomy | 2 | 1 | 4 | 1 | 0 | 0 | 2 | 3 | 0 | 100 | ||
| Pyeloplasty | 2 | 0 | 1 | 2 | 0 | 0 | 2 | 1 | 0 | 100 | ||
| Ureteral reimplantation | 2 | 2 | 2 | 4 | 4 | 0 | 4 | 6 | 0 | 100 | ||
| Appendiceal graft ureteroplasty | 4 | 4 | 4 | 3 | 2 | 0 | 4 | 5 | 0 | 100 | ||
| Oral graft ureteroplasty | 8 | 2 | 7 | 4 | 4 | 0 | 8 | 7 | 0 | 100 | ||
| Ileal ureter replacement | 10 | 6 | 9 | 7 | 8 | 1 | 11 | 13 | 1 | 96 | ||
| Balloon dilation | 2 | 2 | 1 | 1 | 1 | 1 | 2 | 2 | 0 | 75 | ||
*Only patients presented with symptoms before surgery were included. |
中位随访时间为14.2(6.1~107.1)个月,总体成功率97.2%(图 2)。手术前后肌酐分别为(91.29±23.46) μmol/L vs.(92.15±23.10) μmol/L(P=0.572),估算肾小球过滤率分别为(83.81±20.21) mL/(min·1.73 m2) vs.(81.35± 18.59) mL/(min·1.73 m2)(P=0.204)。1例患者在球囊扩张术后1年出现肾积水加重,影像学检查提示输尿管狭窄,再次手术应用阑尾补片重建输尿管,术后随访1年,肾积水程度减轻。1例回肠代输尿管患者术后14个月积水程度加重,保守观察,继续随访4年肾积水稳定。术后并发症见表 3。
{kind=link}
{kind=link}
{kind=link}
{kind=link}
图2 结石相关输尿管狭窄的不同重建手术策略Figure 2 Different surgical strategies for stone related ureteral stricture A, ureteroureterostomy; B, ureteral reimplantation (psoas hitch); C, autologous mucosal graft ureteroplasty; D, ileal ureter replacement. |
表3 患者术后并发症及治疗Table 3 Postoperative complications and management |
| Grade | Complications | Operation and incidence rate | Management |
| Ⅰ | Urine leakage at the proximal anastomotic site | Ileal ureter (1/25) | Prolong the DJ stent drainage time |
| Obstruction | Ileal ureter (1/25) | Prolong the DJ stent drainage time | |
| Urinary tract infection | Ileal ureter (2/25) Appendiceal graft (1/9) | Oral antibiotic | |
| Ⅱ | Incomplete intestinal obstruction | Ileal ureter (1/25) | Nothing by mouth, gastrointestinal decompression, parenteral nutrition |
| Ⅲb | Incisional hernia | Ileal ureter (1/25) | Herniorrhaphy |
| Calculi | Ileal ureter (1/25) | Lithohtripsy |
3 讨论
结石相关输尿管狭窄主要发生在输尿管结石嵌顿、黏膜损伤或手术干预后,其病理机制复杂,临床表现多样,处理具有一定挑战性。近年来,随着泌尿外科微创技术的广泛应用,结石相关输尿管狭窄的发生率有所升高。结石相关输尿管狭窄的发生机制主要涉及机械损伤与热损伤[6-7]、感染与炎症、瘢痕形成等因素。长期嵌顿的输尿管结石可损伤输尿管黏膜,导致纤维化及管腔狭窄;伴有尿路感染者细菌毒素及炎症介质可引起局部组织水肿、肉芽组织增生,最终形成瘢痕性狭窄[8]。输尿管镜碎石术及经皮肾镜碎石术等微创技术在治疗输尿管结石方面应用广泛[9],但术中输尿管损伤、术后炎症反应及支架管的长期放置均可能增加输尿管狭窄发生的风险,影响患者预后及生活质量。
手术重建输尿管是治疗结石相关输尿管狭窄的有效手段。修复重建应遵循无张力、不漏水、细线吻合、不钳夹黏膜、保护输尿管血供的原则,在此基础上由简入繁选择重建方式[13]。位于输尿管上段近肾盂或下段近膀胱的输尿管狭窄,输尿管端端吻合术、肾盂成形术或输尿管膀胱再植术无法满足无张力吻合时,可借助泌尿系统组织瓣进行修复以减少吻合张力。本研究上段输尿管长段狭窄的患者采用肾盂瓣肾盂成形术,该术式使用肾盂组织修复输尿管缺损的同时,裁剪缩小肾盂体积,有利于构建符合流体力学的肾盂输尿管连接部[14-15]。下段输尿管狭窄患者可借助膀胱腰肌悬吊及Boari瓣缩短缺损长度[16]。长段输尿管狭窄(3~8 cm)如伴随输尿管闭锁,则需进行病变组织切除输尿管后壁加强重建,并采用自体黏膜补片修补缺损[17-18]。阑尾由于其解剖位置和组织特性,可用于修复复杂的右侧输尿管长段狭窄[19-20],但应用阑尾进行修复重建具有一定的偶然性[21],本研究中阑尾补片输尿管成形术往往经历术者术中评估阑尾条件后决定。口腔黏膜厚度适中、弹性好、适应潮湿环境、血供丰富,是输尿管修复的理想材料[22-24],尤其在结石相关狭窄中较为常用,本研究中2~5 cm狭窄的自体黏膜补片修复成功率为100%。对于长段或复杂的输尿管狭窄,回肠代输尿管手术是一种有效的修复方法,有经验的术者手术成功率可达96%,需要注意回肠代输尿管术后并发症较其他术式多,应密切规范随访,监测患者酸碱平衡和电解质稳定情况[25-26]。
针对结石相关输尿管狭窄,本课题组总结诊治经验如下,首先,术前详细了解病史并评估有助于合理的选择治疗方式;第二,术前应制定完备的修复策略和备选方案,根据术中情况灵活选择重建方式;第三,结石相关输尿管狭窄病变周围条件往往较差,术中彻底切除瘢痕组织及活力和血供不佳的输尿管,可减少再狭窄的发生;第四,条件允许的情况下使用网膜或肾周脂肪包裹吻合区域可提供良好的屏障和血供[27];最后,术后严格管理和随访非常必要。
本研究存在一定的局限,首先,受限于回顾性研究的性质,存在不可避免的选择偏倚;其次,患者既往结石治疗多为外院进行,难以获取详细准确的结石情况及相关信息;最后,入组患者例数相对较少,治疗经验有待推广验证,未来将开展前瞻性大样本研究进一步提高证据等级。
综上所述,结石相关输尿管狭窄以上段多见,疾病特点异质性强。根据狭窄的位置、长度、严重程度选择合适的修复重建方式,可以获得满意的手术成功率。