
1 资料与方法
1.1 临床资料
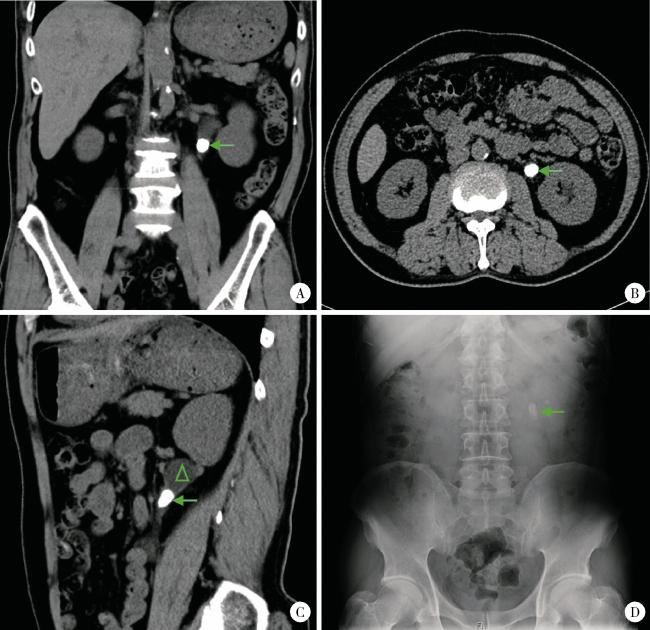
图1 最大径≥1.5 cm输尿管结石的术前影像学表现Figure 1 Imaging characteristics of urolithiasis with largest diameter ≥ 1.5 cm A, coronal CT image, with the arrow indicating the left ureteral calculus, measuring greater than 1.5 cm in length; B, axial CT image, where the arrow marks the location of the calculus; C, sagittal CT image, with the arrow identifying the calculus; notable hydronephrosis due to ureteral obstruction is observed above the calculus (indicated by the triangle); D, the kidneys, ureters, and bladders appearance of a ureteral calculus with a maximum dia-meter of ≥1.5 cm, highlighted by the arrow. |
表1 匹配前患者基线数据Table 1 Baseline statistics of patients before match |
| Items | Urolithiasis patients with largest diameter ≥ 1.5 cm (n=38) | Urolithiasis patients with largest diameter < 1.5 cm (n=305) | P value |
| Age/years, M (Min, Max) | 48.0 (19.0, 73.0) | 48.0 (21.0, 78.0) | 0.659 |
| Gender, n(%) | 0.398 | ||
| Male | 7 (18.4) | 80 (26.2) | |
| Female | 31 (81.6) | 225 (73.8) | |
| BMI/(kg/m2), M (Min, Max) | 24.8 (17.9, 32.7) | 25.6 (17.4, 38.8)b | 0.331 |
| Preoperative SCr/(μmol/L), M (Min, Max) | 97.5 (70.0, 190.0) | 85.0 (47.0, 237.0) | 0.001 |
| Preoperative GFR /[mL/(min·1.73 m2)], M (Min, Max) | 87.0 (44.0, 114.0) | 94.9 (31.0, 143.0) | 0.020 |
| Distance/mma, M (Min, Max) | 17.5 (0.0, 181.0) | 59.0 (0.0, 244.0)c | < 0.001 |
| CT value of stones/HU, M (Min, Max) | 1 120 (424, 1 660) | 800 (116, 1 780)c | < 0.001 |
a, distance refers to that from stone to ureteropelvic junction; b, data of one patient missed; c, data of two patients missed. BMI, body mass index; SCr,serum creatinine; GFR,glomerular filtration rate. |
1.2 手术方法
1.3 统计学分析
2 结果
2.1 匹配前分析
表2 术后1 d清石率影响因素的Logistic回归分析Table 2 Logistic regression analysis of factors affecting stone clearance on 1 d after surgery |
| Variables | B | Standard error | Wald | df | P value | Exp(B) | 95% CI for Exp(B) |
| Gender | 0.305 | 0.400 | 0.761 | 1 | 0.446 | 1.356 | 0.574 - 3.215 |
| Age | -0.014 | 0.016 | 0.922 | 1 | 0.357 | 0.986 | 0.957 - 1.017 |
| Preoperative SCr | -0.014 | 0.009 | 1.481 | 1 | 0.139 | 0.987 | 0.969 - 1.005 |
| Preoperative GFR | -0.013 | 0.014 | 0.898 | 1 | 0.369 | 0.987 | 0.960 - 1.015 |
| Diameter of stone | -0.004 | 0.036 | 0.118 | 1 | 0.906 | 0.996 | 0.931 - 1.066 |
| CT value of stones | -0.001 | 0.001 | 1.837 | 1 | 0.066 | 0.999 | 0.999 - 1.000 |
| Constant | 5.421 | 2.523 | 2.149 | 1 | 0.032 | 224.801 |
SCr, serum creatinine; GFR, glomerular filtration rate. |
表3 术后1个月清石率影响因素的Logistic回归分析Table 3 Logistic regression analysis of factors affecting stone clearance on 1 month after surgery |
| Variables | B | Standard error | Wald | df | P value | Exp(B) | 95% CI for Exp(B) |
| Gender | 0.514 | 0.393 | 1.313 | 1 | 0.189 | 1.671 | 0.758 - 3.672 |
| Age | -0.029 | 0.016 | 1.847 | 1 | 0.065 | 0.971 | 0.936 - 1.008 |
| Preoperative SCr | -0.019 | 0.009 | 5.493 | 1 | 0.032 | 0.981 | 0.963 - 0.999 |
| Preoperative GFR | -0.025 | 0.014 | 3.031 | 1 | 0.081 | 0.976 | 0.948 - 1.004 |
| Diameter of Stone | -0.003 | 0.004 | 0.066 | 1 | 0.947 | 0.998 | 0.992 - 1.005 |
| CT value of stones | 0.000 | 0.000 | 0.002 | 1 | 0.958 | 1.000 | 0.999 - 1.000 |
| Constant | 6.837 | 2.504 | 2.730 | 1 | 0.006 | 9.307 |
SCr, serum creatinine; GFR, glomerular filtration rate. |
2.2 匹配后基线数据分析
表4 匹配后患者基线数据Table 4 Baseline statistics of patients after match |
| Items | Urolithiasis patients with largest diameter ≥ 1.5 cm (n=31) | Urolithiasis patients with largest diameter < 1.5 cm (n=31) | P value |
| Age/years, M (Min, Max) | 47.0 (19.0, 73.0) | 38.0 (22.0, 72.0) | 0.292 |
| Gender, n(%) | 1.000 | ||
| Male | 26 (83.9) | 26 (83.9) | |
| Female | 5 (16.1) | 5 (16.1) | |
| BMI/(kg/m2), ${\bar x}$±s | 25.00 ± 2.64 | 24.70 ± 2.59 | 0.688 |
| Preoperative SCr/(μmol/L), M (Min, Max) | 91.0 (70.0, 158.0) | 93.0 (53.0, 156.0) | 0.844 |
| Preoperative GFR /[mL/(min·1.73 m2)], M (Min, Max) | 88.3 (44.0, 114.0) | 97.3 (40.0, 143.0) | 0.130 |
| Distance/mma, M (Min, Max) | 17 (0, 181) | 25.0 (0, 189) | 0.773 |
| CT value of stones/HU, ${\bar x}$±s | 1 140 ± 330 | 910 ± 291 | 0.005 |
a, distance refers to that from stone to ureteropelvic junction; BMI, body mass index; SCr,serum creatinine; GFR,glomerular filtration rate. |
表5 最大径≥1.5 cm输尿管结石患者匹配上和未匹配上的基线数据对比Table 5 Baseline statistics of urolithiasis patients with largest diameters≥1.5 cm matched and not matched |
| Items | Urolithiasis patients with largest diameter ≥ 1.5 cm not matched (n=7) | Urolithiasis patients with largest diameter ≥ 1.5 cm matched (n=31) | P value |
| Age/years, ${\bar x}$±s | 50.3 ± 13.7 | 48.8 ± 13.6 | 0.706 |
| Gender, n(%) | 0.820 | ||
| Male | 2 (28.6) | 26 (83.9) | |
| Female | 5 (71.4) | 5 (16.1) | |
| BMI/(kg/m2), ${\bar x}$±s | 24.90 ± 2.88 | 25.00 ± 2.64 | 0.825 |
| Preoperative SCr/(μmol/L), M (Min, Max) | 116.0 (74.0, 190.0) | 91.0 (70.0, 158.0) | 0.057 |
| Preoperative GFR/[mL/(min·1.73 m2)], ${\bar x}$±s | 81.3 ± 11.1 | 86.2 ± 19.6 | 0.228 |
| Distance/mma, M (Min, Max) | 18.0 (0.0, 57.8) | 17.0 (0.0, 181.0) | 0.865 |
| CT value of stones/HU, ${\bar x}$±s | 850 ± 371 | 1 140 ± 330 | 0.060 |
a, distance refers to that from stone to ureteropelvic junction. BMI, body mass index; SCr, serum creatinine; GFR, glomerular filtration rate. |
表6 最大径 < 1.5 cm输尿管结石组患者匹配上和未匹配上的基线数据对比Table 6 Baseline statistics of urolithiasis patients with largest diameters < 1.5 cm matched and not matched |
| Items | Urolithiasis patients with largest diameter < 1.5 cm not matched (n=274) | Urolithiasis patients with largest diameter < 1.5 cm matched (n=31) | P value |
| Age/years, M (Min, Max) | 48.0 (21.0, 78.0) | 38.0 (22.0, 72.0) | 0.150 |
| Gender, n(%) | 0.253 | ||
| Male | 75 (27.5) | 26 (83.9) | |
| Female | 199 (72.6) | 5 (16.1) | |
| BMI/(kg/m2), M (Min, Max) | 25.6 (17.4, 38.8)b | 24.7 (18.0, 30.8) | 0.121 |
| Preoperative SCr/(μmol/L), M (Min, Max) | 84.0 (47.0, 237.0) | 93.0 (53.0, 156.0) | 0.069 |
| Preoperative GFR/[mL/(min·1.73 m2)], M (Min, Max) | 94.5 (31.0, 142.0) | 97.3 (40.0, 143.0) | 0.669 |
| Distance/mma, M (Min, Max) | 68.0 (0.0, 244.0)c | 25.0 (0.0, 189.0) | < 0.001 |
| CT value of stones/HU, M (Min, Max) | 790 (116, 1 780)c | 950 (348, 1 510) | 0.113 |
a, distance refers to that from stone to ureteropelvic junction; b, data of one patient missed; c, data of two patients missed. BMI, body mass index; SCr, serum creatinine; GFR, glomerular filtration rate. |
2.3 术后结局变量分析
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
表7 匹配后病例的RULL + N-trap手术治疗结果Table 7 RULL + N-trap outcomes of cases after matching |
| Items | Urolithiasis patients with largest diameter ≥1.5 cm (n=31) | Urolithiasis patients with largest diameter < 1.5 cm (n=31) | P value |
| Largest diameter of stone/mma, M (Min, Max) | 17.0 (15.0, 27.1) | 10.8 (4.0, 14.0) | < 0.001 |
| ΔSCr/(μmol/L)b, ±s | -6.58 ± 16.10 | -13.70 ± 12.50 | 0.149 |
| ΔGFR/[mL/(min·1.73 m2)]c, ±s | 5.92 ± 14.90 | 7.47 ± 11.20 | 0.508 |
| Hospitalization after surgery/d, ±s | 2.26 ± 1.79 | 2.03 ± 0.80 | 0.927 |
| Operating time/min, ±s | 85.8 ± 28.8 | 62.4 ± 24.6 | 0.001 |
| Stone clearance 1 d, n(%) | 0.237 | ||
| Success | 28 (90.3) | 31 (100.0) | |
| Fail | 3 (9.7) | 0 (0.0) | |
| Stone clearance 1 month, n(%) | 0.472 | ||
| Success | 29 (93.5) | 31 (100.0) | |
| Fail | 2 (6.5) | 0 (0.0) |
a, largest diameter refers to that of stones; b, ΔSCr means perioperative SCr changes; c, ΔGFR means perioperative GFR changes. RULL + N-trap, rigid ureteroscopic laser lithotripsy combined with N-trap; BMI, body mass index; SCr, serum creatinine; GFR, glomerular filtration rate. |
表8 RULL + N-trap术后1 d清石率Table 8 Stone clearance on 1 d after RULL + N-trap |
| Items | Total | Success, n(%) | Fail, n(%) | χ2 | P |
| Urolithiasis patients with largest diameter ≥1.5 cm | 31 | 28 (90.3) | 3 (9.7) | 1.401 | 0.237 |
| Urolithiasis patients with largest diameter < 1.5 cm | 31 | 31 (100.0) | 0 (0.0) |
RULL + N-trap, rigid ureteroscopic laser lithotripsy combined with N-trap. |
表9 RULL + N-trap术后1个月清石率Table 9 Stone clearance on 1 month after RULL + N-trap |
| Items | Total | Success, n(%) | Fail, n(%) | χ2 | P |
| Urolithiasis patients with largest diameter ≥1.5 cm | 31 | 29 (93.5) | 2 (6.5) | 0.517 | 0.472 |
| Urolithiasis patients with largest diameter < 1.5 cm | 31 | 31 (100.0) | 0 (0.0) |
RULL + N-trap, rigid ureteroscopic laser lithotripsy combined with N-trap. |