
女性高雄激素血症是指女性体内雄激素水平异常升高,常伴随一系列相关症状,如胰岛素抵抗、肥胖、多毛、痤疮等[1],但也有部分患者可能仅表现为实验室检测的睾酮水平升高,而无多毛、痤疮、脱发等典型高雄激素症状,这种现象可能与个体的雄激素受体敏感性、种族差异及检测方法的局限性有关[2-4]。高雄激素血症还与多囊卵巢综合征(polycystic ovary syndrome,PCOS)、代谢综合征、胰岛素抵抗、2型糖尿病(type 2 diabetes mellitus, T2DM) 以及心血管疾病等有一定相关性[5-8]。研究表明,PCOS患者中约70%左右存在高雄激素血症[9],而在高雄激素血症女性中,胰岛素抵抗的发生率可高达50%~ 70%[10]。目前,临床上检测睾酮水平的方法主要包括免疫法和质谱法。免疫法因其操作简便、成本较低而被广泛应用,但其特异性较差,容易受到交叉反应的干扰,导致睾酮水平假性升高[11]。相较之下,液相色谱-串联质谱法(liquid chromatography-tandem mass spectrometry,LC-MS/MS)因具有更高的灵敏度和特异性,被认为是测定睾酮水平的金标准[4, 12]。已有研究表明,在使用免疫法检测的部分高雄激素血症患者中,采用质谱法复测后睾酮水平显示正常[4, 13]。国内外相关研究也表明,免疫法检测的睾酮水平较质谱法偏高,尤其是在低浓度范围内(如女性、儿童患者)[14-16]。然而,在临床上我们发现,部分被诊断为高雄激素血症的女性患者并没有典型的高雄激素血症的临床表现(如多毛、痤疮、脱发、肥胖、嗓音变粗等),提示其可能存在假性升高的情况。此外,一些因月经稀发、不孕等原因就诊的女性患者采用免疫法检测睾酮水平升高,但质谱法的检测结果却显示睾酮水平正常。这种假性升高现象可能导致患者进行一系列后续检查(如影像学检查、内分泌功能评估等),但这些检查结果的阳性率并不高,这不仅可能对患者造成心理负担,还可能导致医疗资源的浪费。为此,我们开展了本项研究,旨在探讨女性睾酮假性升高现象的发生比例,并评估质谱法检测在女性睾酮检测中的重要意义,希望本研究结果能有助于减少因误诊或不必要的治疗对患者造成的不良影响,优化诊断和治疗策略,同时减少医疗资源的浪费。
1 资料与方法
1.1 研究设计和血清睾酮水平检测
本研究为横断面研究,基于北京大学人民医院科研数据平台,回顾性分析2020年1月1日至2024年5月1日期间在北京大学人民医院就诊的女性患者,这些患者初次通过化学发光免疫分析法(chemiluminescence immunoassay, CLIA)检测发现血清睾酮水平升高,随后再次采集血样,并使用LC-MS/MS进行复测。本研究为回顾性研究,符合临床实际操作流程,分别在同一患者不同次的血清样本中进行CLIA和LC-MS/MS检测。CLIA的检测平台为美国Beckman Coulter DXI800全自动化学分析仪,成年女性血清睾酮水平的参考范围为0.00~2.60 nmol/L;质谱法的检测平台为美国Waters TQS液相色谱串联质谱仪,成年女性血清睾酮水平的参考范围为0.07~1.56 nmol/L。本研究经北京大学人民医院医学伦理委员会审查批准(2024PHB421-001)。
1.2 纳入标准、排除标准和患者分组
纳入标准:(1)年龄≥18岁的成年女性;(2)免疫法检测睾酮水平高于参考范围(>2.60 nmol/L);(3)同期进行了质谱法复测的患者。排除标准:(1)病历记录不全,无法获取完整的实验室和临床数据的患者;(2)使用激素类药物或其他可能影响雄激素水平的药物治疗的患者;(3)孕期或哺乳期患者。
使用LC-MS/MS检测的睾酮值作为诊断睾酮升高的参考标准,将患者分成两组:(1)真性睾酮升高组:CLIA检测睾酮水平升高(>2.6 nmol/L)且LC-MS/MS检测睾酮水平也升高(>1.56 nmol/L);(2)假性睾酮升高组:CLIA检测睾酮水平升高(>2.6 nmol/L),但LC-MS/MS检测结果未达到升高标准(≤1.56 nmol/L)。
1.3 数据收集
收集患者的一般信息及检查结果,包括年龄,睾酮、胰岛素、血糖、皮质醇、促肾上腺皮质激素(adrenocorticotrophic hormone,ACTH)水平,甲状腺功能,胰岛素样生长因子1水平,妇科彩超,肾上腺彩超,肾上腺CT,甲状腺彩超等。
1.4 统计学分析
采用SPSS 26.0 (IBM corporation, Armonk, NY, USA)软件进行数据分析及处理。计数资料用率描述,计量资料采用Shapiro-Wilk检验数据正态性,若数据呈正态分布,则采用均值±标准差表示,组间差异检验采用t检验;若数据为非正态分布,则采用M(P25,P75)表示,组间差异采用秩和检验。显著性水准α设为0.05,P < 0.05为差异有统计学意义。
2 结果
2.1 两组间CLIA检测睾酮水平的比较
共纳入287例CLIA检测出睾酮水平升高的女性患者,患者平均就诊年龄为(33.01±8.65)岁。根据LC-MS/MS检测的睾酮水平是否升高,178例(62.0%)患者被归类为假性睾酮升高组,109例(38.0%)患者被归类为真性睾酮升高组。CLIA的假阳性率为62.0%,提示其假阳性率较高。在假性睾酮升高组中,CLIA检测的睾酮水平为(3.63± 1.60) nmol/L,LC-MS/MS检测的睾酮水平为(0.92± 0.33) nmol/L。在真性睾酮升高组中,CLIA检测的睾酮水平为(4.13±2.20) nmol/L,LC-MS/MS检测的睾酮水平为(2.86±2.66) nmol/L。进一步的统计分析显示,CLIA测定的睾酮水平在两组间差异有统计学意义(P < 0.05)。
2.2 CLIA检测方法的敏感性和特异性
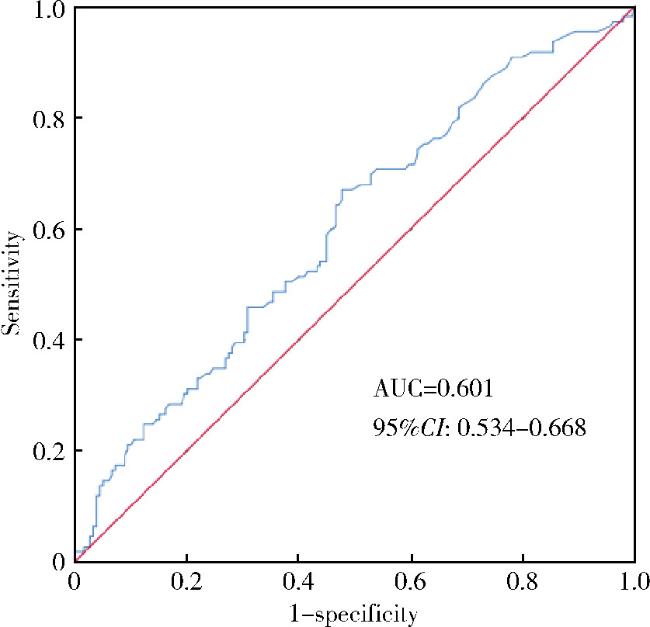
以LC-MS/MS检测结果超过正常范围作为定性结局,将CLIA的检测值作为连续变量,通过受试者工作特征(receiver operating characteristic, ROC)曲线分析,得到CLIA检测睾酮水平的ROC曲线下面积(area under the curve,AUC)为0.601(95%CI:0.534~0.668),提示其诊断准确性较低,难以通过设定截断值来提高诊断性能(图 1)。
{kind=link}
{kind=link}
2.3 假性睾酮升高组患者的后续检查
在178例假性睾酮升高组患者中,有118例(66.29%)无脱发、多毛、痤疮等高雄激素血症的临床表现,一部分患者接受了进一步的检查评估,其中,40.45%的患者进行了多次CLIA的复测,最多者复测了9次;61例(34.27%)被诊断为PCOS的患者中,有33例(54.10%)彩超检查未见多囊卵巢样改变;血糖检测显示,85.91%的患者血糖正常;胰岛素水平检测显示,95.04%的患者结果正常;178例患者均进行了皮质醇检测,复测后均为正常。此外,部分患者接受了妇科超声、甲状腺超声及功能、肾上腺影像学及功能检查(表 1)。
表1 假性睾酮升高组(n=178)患者的进一步检查情况Table 1 Additional evaluations in testosterone level pseudo-elevated group (n=178) |
| Evaluation items | Cases, n (%) | Results or special conditions |
| Testosterone retesting (CLIA) | 72 (40.45) | Up to 9 retests |
| Diagnosed with PCOS | 61 (34.27) | 28 cases (45.90%) with polycystic ovaries on ultrasound, 33 cases (54.10%) without |
| BG | 149 (83.71) | 128 normal cases (85.91%), 21 cases (14.09%) diagnosed with diabetes or elevated blood sugar |
| Insulin | 121 (67.98) | 115 normal cases (95.04%), 3 elevated cases (2.48%), 3 decreased cases (2.48%) |
| Cortisol | 178 (100.00) | 18 elevated cases (10.11%), retests normal; 42 decreased cases (23.60%), retests normal |
| ACTH | 63 (35.39) | 7 elevated cases (11.11%), retests normal |
| IGF-1 | 19 (10.67) | 3 elevated cases (15.79%), 2 retests normal |
| GH | 10 (5.62) | 9 normal cases (90.00%), 1 elevated (10.00%) |
| Thyroid function | 142 (79.78) | 22 cases (15.79%) with abnormal thyroid function |
| Gynecological ultrasound | 132 (74.16) | 28 cases (21.21%) with polycystic changes, 30 cases (22.73%) with uterine fibroids |
| Adrenal ultrasound | 18 (10.11) | No significant abnormalities in all cases (100.00%) |
| Adrenal CT | 18 (10.11) | 10 cases (55.56%) with no significant abnormalities, 8 cases (44.44%) with adrenal nodules or thickening |
| Thyroid ultrasound | 30 (16.85) | 19 cases (63.33%) with thyroid nodules, 9 cases (30.00%) with diffuse changes, 6 cases (20.00%) with heterogeneous echogenicity, 4 cases (13.33%) with no abnormalities |
CLIA, chemiluminescent immunoassay; PCOS, polycystic ovary syndrome; BG, blood glucose; ACTH, adrenocorticotrophic hormone; IGF-1, insulin-like growth factor 1; GH, growth hormone. |
3 讨论
既往已有研究表明,免疫法在高雄激素血症检测中的应用受到限制,其检测结果的假阳性率较高[20],特别是在睾酮水平低的女性和儿童中[14-16]。Rosner等[13]比较了免疫法和质谱法在检测成年女性及性腺功能低下男性样本中的睾酮水平,也发现免疫法存在显著的高估现象。本研究进一步验证了免疫法在低浓度睾酮水平检测中准确性较低这一问题,ROC分析显示,CLIA检测的AUC仅为0.601,提示其准确性较差,这表明CLIA难以通过设定截断值来提高诊断性能,假阳性率较高,容易导致误诊。此外,在对于青春期女孩的研究中,CLIA检测的中位数显著高于LC-MS/MS[21],与本研究中CLIA假阳性率较高的结果相符。免疫法的假阳性主要源于其低特异性,易受其他类固醇激素或类似分子的干扰[11]。
国内亦有报道免疫法测定女性患者睾酮水平假性升高的病例[22],该报道主要聚焦于11例睾酮假性升高患者的临床特征,而本研究进一步从大样本数据中验证了这一现象,并系统分析了睾酮假性升高的比例及其对诊疗流程的影响,特别是由此导致的诊疗错误和医疗资源浪费问题,并强调了LC-MS/MS在提高诊断准确性中的重要作用。本研究发现,假性睾酮升高组中40.45%的患者进行了CLIA复测,复测次数最多者高达9次,显著增加了患者的经济负担和精神压力。此外,74.16%的患者接受了妇科彩超检查,但仅21.21%的患者提示有多囊样改变。假性睾酮升高组的所有患者均进行了皮质醇水平检测,检测结果中虽有60例(33.71%)提示异常,但在后续的复测及ACTH检测中均提示正常,这显著浪费了医疗资源,并加剧了患者的精神焦虑和经济负担。20.22%的患者接受了肾上腺彩超或CT检查,但均未发现明显异常。这些不必要的检查不仅浪费了医疗资源,还可能延误其他疾病的诊断。与既往研究相比,本研究从患者诊疗流程的角度进一步揭示了CLIA假阳性结果增加了临床工作量和医疗成本。
LC-MS/MS具有高特异性和高灵敏度,能够更精确地区分睾酮以及与其结构类似的代谢物或干扰物(如双氢睾酮、雌二醇等),从而显著减少交叉反应导致的假性升高或假性降低,被认为是检测类固醇激素的“金标准”[12, 25],本研究结果也支持这一观点。然而,LC-MS/MS在常规临床实践中的应用受到设备成本高、操作复杂和检测周期长等因素的限制[26]。相比之下,CLIA因其操作简便、成本较低,仍然是许多医疗机构的首选检测方法。因此,如何在临床实践中合理选择检测方法,平衡检测的准确性与可及性,是当前需要解决的重要问题。本研究建议,未来可以从以下几个方面优化检测流程:(1)在初筛阶段仍可采用免疫法检测,但对于检测结果升高的患者,应优先采用质谱法复测,以提高诊断准确率,避免误诊和不必要的检查;(2)随着技术的进步,质谱法的设备成本和操作复杂性有望逐步降低,这将有助于其在常规临床实践中的广泛应用;(3)可以通过卫生经济学模型进一步量化免疫法假阳性导致的额外检查和治疗成本,与质谱法检测的直接成本进行比较,为临床实践提供更具体的经济学依据。
本研究存在一定的局限性:(1)本研究为回顾性研究,所有数据均来源于门诊病历记录,缺乏对患者体重、腰围和体重指数等变量的完整记录,无法进一步分析肥胖与睾酮水平的关系;(2)免疫法和质谱法检测未使用同一血样,而是基于两次独立采血完成,可能受到生理波动(如月经周期、昼夜节律等)的影响,未来研究可通过更精确的时间控制或动态监测设计优化研究策略;(3)本研究仅使用了单一检测平台的数据,未能纳入其他检测平台[如罗氏(Roche)、雅培(Abbott Laboratories)等]的比对数据,未来应设计前瞻性研究,纳入多种检测平台进行比对,以进一步探讨不同平台在女性睾酮检测中的表现差异;(4)本研究也未纳入真阴性和假阴性患者,无法全面评估CLIA的敏感性和特异性,这将在后续研究中进一步完善。
综上所述,本研究通过大样本数据验证了免疫法在女性睾酮检测中的假阳性问题,量化了其假阳性率及其对临床诊疗流程的影响,强调了质谱法在提高诊断准确性中的重要性,并从诊疗流程的角度揭示了假阳性结果对医疗资源的浪费和患者负担的影响。然而,质谱法在实际临床应用中仍存在设备成本高、操作复杂、检测周期长等局限性,限制了其在常规临床实践中的广泛应用。未来应进一步探索如何优化检测流程,降低质谱法的应用门槛,同时结合不同检测方法的优势,为女性雄激素检测提供更高效、更精准的解决方案。