
1 材料与方法
1.1 模型制作
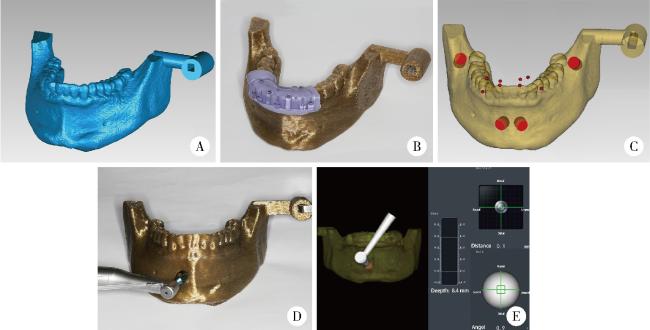
图2 导航辅助环钻取骨的方案设计及实施Figure 2 Digital plan and conduction of the navigation-assisted trephine method for bone harvesting A, digitally designed model of the in vitro study; B, registration device of dynamic navigation system was positioned on the lower anterior teeth; C, design digital trephine osteotomy tracts (red); D, use trephines to complete the osteotomy tracts under the guidance of dynamic navigation; E, real-time positioning and angular deviations of the trephine are displayed in the dynamic navigation system. |
1.2 环钻取骨方案设计
1.3 环钻取骨方案实施
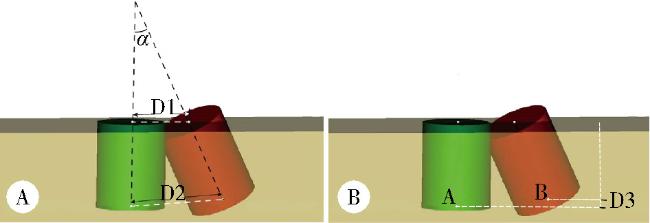
1.4 准确度测量与评价
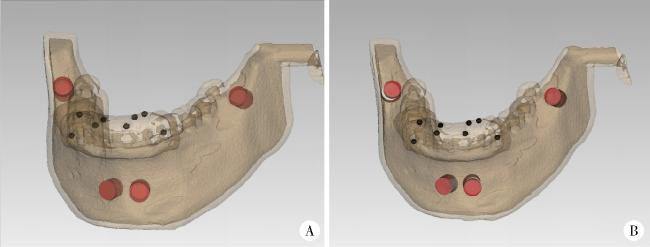
图3 动态导航辅助环钻取骨准确性的数据分析Figure 3 Statistical measurement for dynamic navigation-assisted trephine bone harvesting accuracy A, actual osteotomy tracts were adapted in the post-lab CBCT (red); B, superimpose the actual osteotomy tracts (red) to the planned ones (white) based on the mental fiducial markers on the registration device (black). |
2 结果
表1 动态导航辅助环钻取骨误差Table 1 Descriptive values of deviations in dynamic navigation-assisted trephine methods for bone harvesting |
| Deviations | n | ${\bar x}$±s | Minimum | Maximum |
| Coronal center point/mm | 40 | 1.91±0.69 | 0.64 | 3.12 |
| Apical center point/mm | 40 | 1.54±0.66 | 0.41 | 2.94 |
| Depth of apical center point/mm | 40 | -0.84±0.77 | -2.22 | 0.63 |
| Axis angle/(°) | 40 | 3.02±0.38 | 2.11 | 3.72 |
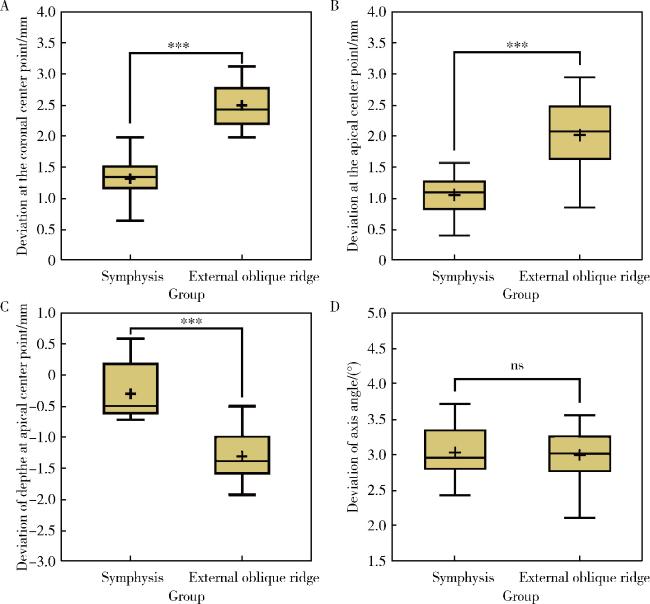
表2 动态导航辅助环钻取骨在颏部及外斜线区域的误差Table 2 Descriptive values of deviations in dynamic navigation-assisted trephine methods for bone harvesting in the symphysis and external oblique line area |
| Deviations | Donor sites | n | ${\bar x}$±s | Minimum | Maximum | t | P |
| Coronal center point/mm | Symphysis | 20 | 1.32±0.36 | 0.64 | 1.98 | -10.42 | <0.01 |
| External oblique line | 20 | 2.50±0.35 | 1.98 | 3.12 | |||
| Apical center point/mm | Symphysis | 20 | 1.06±0.31 | 0.41 | 1.57 | -6.70 | <0.01 |
| External oblique line | 20 | 2.02±0.56 | 0.86 | 2.94 | |||
| Depth of apical center point/mm | Symphysis | 20 | -0.30±0.52 | -1.13 | 0.63 | 4.81 | <0.01 |
| External oblique line | 20 | -1.38±0.57 | -2.22 | -0.55 | |||
| Axis angle/(°) | Symphysis | 20 | 3.03±0.38 | 2.43 | 3.72 | 0.26 | 0.80 |
| External oblique line | 20 | 3.00±0.39 | 2.11 | 3.56 |
The independent sample t test was used to analyse the difference between the groups, the significant level was P<0.05. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
图5 在颏部外斜线区使用动态导航辅助环钻取骨准确性的差异分析Figure 5 Analysis of differences in bone harvesting accuracy using dynamic navigation-assisted trephine in extraoral oblique line and symphysis A, deviations in coronal center points; B, deviations in apical center points; C, deviations in depth of apical center points; D, deviations in the axial angles. ns, correlation is not significant at the 0.05 level (2-tailed); * * * correlation is significant at the 0.001 level (2-tailed). |