
1 材料与方法
1.1 实验动物及实验前准备
1.2 模型建立方法
1.2.1 实验Ⅰ组
1.2.2 实验Ⅱ组
1.2.3 空白对照组
1.3 内镜下检查
1.4 食管造影检查及狭窄指数
1.5 组织病理学检查及羟脯氨酸测定
表1 病变损伤评分标准Table 1 Lesion damage scoring criteria |
| Damage category | Lesion degree | Score |
| Submucosal collagen deposition | No submucosal collagen deposition | 0 |
| Mild (collagen deposition in submucosa < twice the thickness of muscularis mucosae) | 1 | |
| Severe (collagen deposition in submucosa>twice the thickness of muscularis mucosae) | 2 | |
| Mucosal muscularis injury | No | 0 |
| Yes | 1 | |
| Muscularis propria injury and collagen deposition | No | 0 |
| Mild (collagen deposition around smooth muscle fibers) | 1 | |
| Severe (in addition to the above changes, some smooth muscle fibers are replaced by collagen) | 2 |
1.6 统计学方法
2 结果
2.1 一般情况
表2 实验前后各组体重Table 2 Weight in each group before and after the operation |
| Group | Before the operation | 1 week after the operation | 2 weeks after the operation | 4 weeks after the operation | |||||||
| n | Weight/kg | n | Weight/kg | n | Weight/kg | n | Weight/kg | ||||
| Blank control group | 4 | 3.10±0.39 | 4 | 3.25±0.34 | 4 | 3.48±0.33 | 4 | 4.13±0.25* | |||
| Experimental group Ⅰ | 9 | 2.91±0.54 | 9 | 2.52±0.59 | 8 | 2.72±0.54 | 8 | 2.91±0.28 | |||
| Experimental group Ⅱ | 9 | 3.51±0.37 | 9 | 2.90±0.35 | 8 | 2.62±0.37 | 7 | 2.02±0.31* | |||
Data are expressed as ${\bar x}$±s. *P<0.05, vs. before the operation. |
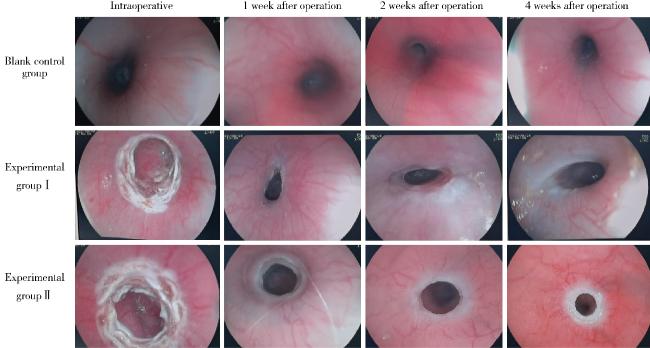
2.2 食管在内镜下的表现
2.3 造影下食管内径及狭窄指数
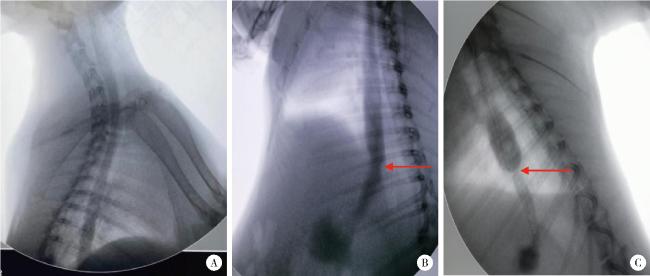
图2 各组术后4周食管造影Figure 2 Esophagography at 4 weeks after operation in each group A, blank control group; B, experimental group Ⅰ; C, experimental group Ⅱ. The arrows show the sites of esophageal stenosis. |
表3 造影下测得的食管内径及狭窄指数Table 3 Esophageal inner diameter by angiography and the stricture index |
| Group | Esophageal inner diameter/mm | Stricture index | |
| Preoperative | 4 weeks after operation | ||
| Blank control group | 12.83±1.07 | 12.89±0.83 | 0.995±0.028 |
| Experimental group Ⅰ | 12.06±0.32 | 11.19±0.97 | 1.083±0.104 |
| Experimental group Ⅱ | 12.58±1.11 | 10.49±1.76* | 1.242±0.148#△ |
Data are expressed as ${\bar x}$±s. *P < 0.05,vs. preoperative; # P<0.05, vs. blank control group; △P<0.05, vs. experimental group Ⅰ. |
2.4 组织病理学检查结果
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
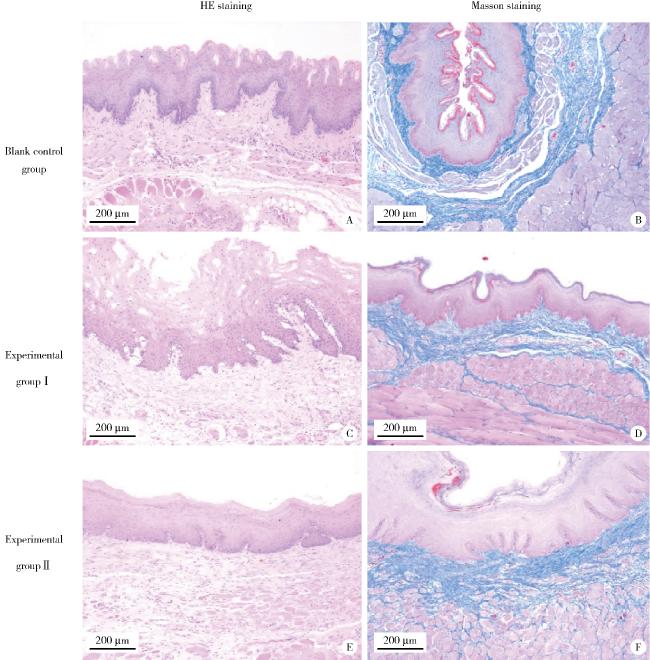
图3 各组病理HE染色和Masson染色结果Figure 3 Pathological HE staining and Masson staining results of each group A, C and E are the hematoxylin eosin (HE) staining results of blank control group, experimental group Ⅰ and experimental group Ⅱ, repecitively; B, D and F are the Masson staining results of blank control group, experimental group Ⅰ and experimental group Ⅱ, repecitively. |
表4 各组食管组织病理学评分和羟脯氨酸含量Table 4 Esophageal histopathological score and hydroxyproline content in each group |
| Group | Pathology score | Hydroxyproline/(μg/g) |
| Blank control group (n=4) | 0 | 91.37±29.74 |
| Experimental group Ⅰ (n=9) | 2.55±0.52* | 182.90±72.75* |
| Experimental group Ⅱ (n=9) | 4.55±0.52*# | 210.81±54.28* |
Data are expressed as ${\bar x}$±s. *P<0.05, vs. blank control group; # P<0.05, vs. experimental group Ⅰ. |