
胃肝样腺癌(hepatoid adenocarcinoma of the stomach,HAS)是一种罕见的胃癌亚型,约占所有胃癌病例的1%[1], 其病理学特征表现为腺癌和肝细胞癌样分化共存,常伴有组织甲胎蛋白(alpha-fetoprotein,AFP)表达或血清AFP升高。HAS恶性程度高,易发生血行转移和淋巴结转移,肝转移概率高,预后差。目前,HAS的综合治疗尚无高级别证据共识,手术仍是唯一可能治愈的治疗手段。临床中,常规新辅助/转化治疗方案在HAS中往往效果有限,这可能与其特殊的分子生物学机制密切相关。基于此,本文对1例初始不可切除HAS病例的诊疗经过、病理特征及分子生物学特点进行分析,探讨该疾病的诊断及治疗策略,为临床实践提供参考。
1 病例报告
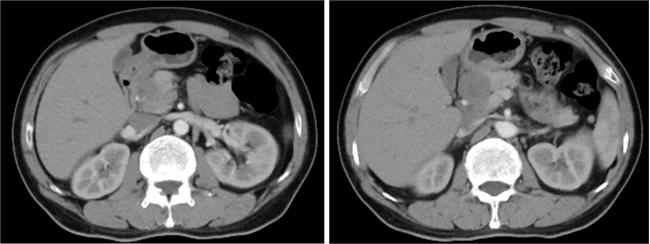
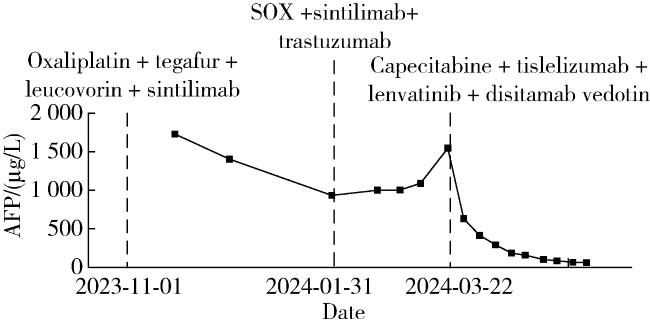
患者为56岁男性,因“无明显诱因腹痛、腹胀、黑便1年”就诊于当地医院。胃镜检查提示胃窦黏膜充血水肿,前壁可见一溃疡,表面可见大量血管裸露,少量渗血;病理活检报告提示为分化差的癌,倾向腺癌(中-低分化);腹盆计算机断层扫描(computed tomography,CT)提示胃窦壁增厚,肝胃间隙、肝门区及大网膜区见肿大淋巴结,大者最大截面约3.9 cm×2.7 cm,腹膜后可见稍大淋巴结(图 1);肿瘤标志物检测结果为癌胚抗原(carcinoembryonic antigen,CEA)16.53 μg/L,糖类抗原19-9(carbohydrate antigen 19-9,CA19-9)17.1 U/mL。诊断为胃窦腺癌,初始不可切除。随后于当地医院行3个周期的一线转化治疗(奥沙利铂+替加氟+亚叶酸钙+ 信迪利单抗)。第2周期治疗前复查肿瘤标志物,AFP为1 729.53 μg/L,CEA为18.70 μg/L;同时复查腹盆CT提示胃窦壁不均匀性增厚,呈中度略不均匀强化,肝胃间隙、肝门区及大网膜区见肿大淋巴结,大者最大截面约3.4 cm×3.3 cm,腹膜后可见稍大淋巴结。依据实体瘤疗效评价标准(Response Evaluation Criteria in Solid Tumors,RECIST),疗效评价为疾病稳定(stable disease,SD)。第3周期治疗前肿瘤标志物检测结果为AFP 1 403.1 μg/L、CEA 11.01 μg/L。第4周期治疗前AFP和CEA分别降至666.39 μg/L和7.72 μg/L,继续于当地医院行第4周期一线治疗,用药调整为奥沙利铂+卡培他滨+信迪利单抗。
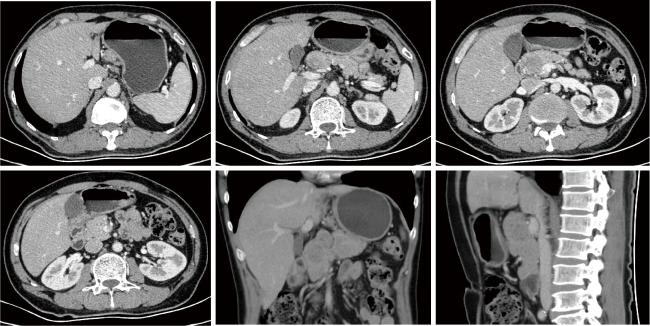
第4周期一线治疗后,患者于2024年1月17日就诊于北京大学肿瘤医院,经病理会诊确诊为(胃窦)中分化腺癌伴肝样腺癌分化(Lauren:肠型)。免疫组织化学染色结果:细胞间质上皮转化因子(cellular-mesenchymal to epithelial transition factor,c-MET)(80%中等+)、EB病毒编码的小RNA(Epstein-Barr virus encoded small RNA,EBER)(-)、表皮生长因子受体(epidermal growth factor receptor,EGFR)(90%强+)、错配修复功能完整(proficient mismatch repair,pMMR)、程序性死亡配体1(programmed death-ligand 1,PD-L1)联合阳性评分(combined positive score,CPS)15分、人表皮生长因子受体2(human epidermal growth factor receptor 2,HER2)(2+)。荧光原位杂交(fluorescence in situ hybridization,FISH)检测结果证实为HER2基因扩增。腹盆CT提示胃窦部胃壁增厚,较厚处约12 mm,增强扫描强化明显;胃周多发淋巴结肿大,较大者仍约34 mm×31 mm,与胰腺分界欠清(图 2)。建议患者联合曲妥珠单抗靶向治疗。患者返当地医院继续行第5、6周期奥沙利铂+卡培他滨+信迪利单抗+曲妥珠单抗方案的一线转化治疗,治疗过程中AFP持续进展:第5周期后1 003.02 μg/L,第6周期后上升为1 546.07 μg/L。
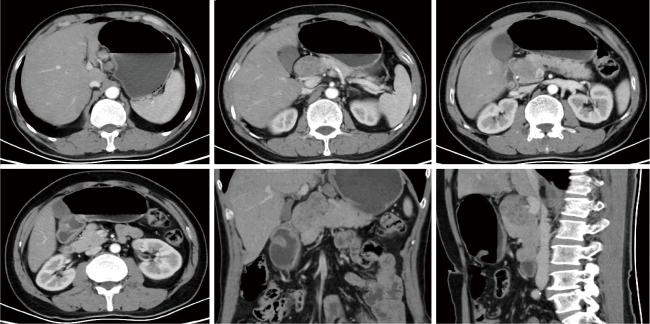
第6周期一线转化治疗后,患者至我院复诊,复查腹盆CT提示胃周部分淋巴结继续增大,较大者原约34 mm×31 mm,现约46 mm×31 mm(图 3)。临床疗效评价综合考虑为疾病进展(progressive disease,PD)。经多学科讨论建议改行二线卡培他滨+替雷利珠单抗+仑伐替尼+维迪西妥单抗方案转化治疗。
患者返回当地医院行第1周期二线转化治疗,治疗过程中血小板减少Ⅲ度,伴乏力、发热,因此,卡培他滨用药7 d后停药,仑伐替尼用药13 d后停药。后续第2、3周期二线治疗改用维迪西妥单抗+仑伐替尼+替雷利珠单抗,过程中患者AFP持续下降,第2周期治疗后为102.3 μg/L。复查CT可见胃窦部胃壁增厚大致同前,胃周多发肿大淋巴结部分缩小,较大者原约46 mm×31 mm,现约25 mm×22 mm (图 4)。疗效评价为部分缓解(partial response,PR)。第3周期二线治疗后再次复查CT见胃周肿大淋巴结继续缩小,较大者原约25 mm×22 mm,现约14 mm×13 mm(图 5)。疗效评价为PR。完善氟-18标记氟代脱氧葡萄糖正电子发射断层/计算机断层扫描(fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography,18F-FDG PET-CT),提示胃窦壁增厚伴放射性摄取轻度增高,最大标准化摄取值(maximum standard uptake value,SUVmax)为2.8;胃小弯侧、胃左动脉旁、肝总动脉旁、腹腔干旁见多发肿大淋巴结,较大者伴放射性浓聚,摄取最高及最大者位于肝总动脉旁,SUVmax为15.7,大小约2.7 cm×2.1 cm,病灶与胰头分界不清(图 6)。整个转化治疗中AFP检测结果见图 7。
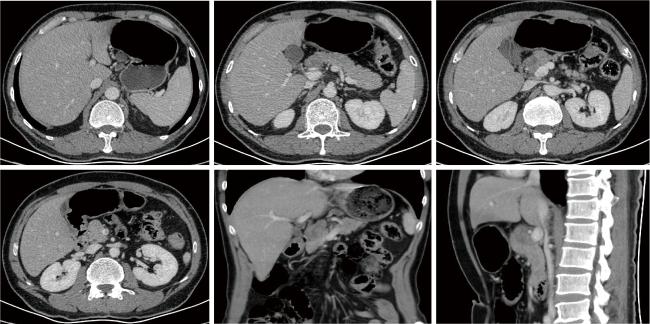
图4 二线治疗2周期后的腹盆增强CT图像Figure 4 Images of enhanced abdominal and pelvic CT scan after 2 cycles of second-line therapy |
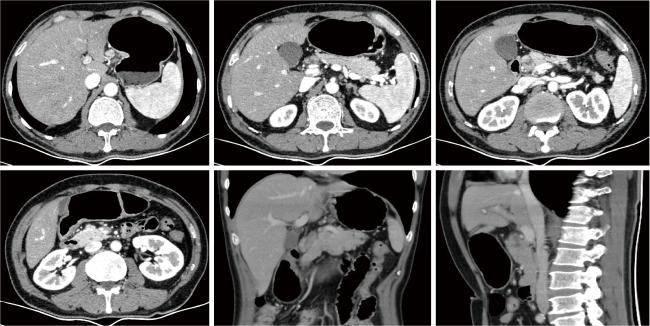
图5 二线治疗3周期后的腹盆增强CT图像Figure 5 Images of enhanced abdominal and pelvic CT scan after 3 cycles of second-line therapy |
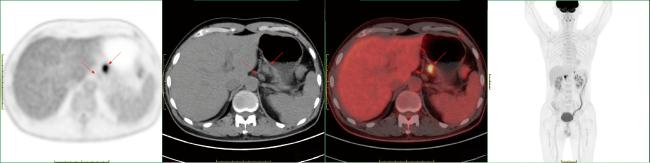
图6 二线治疗3周期后的 18F-FDG PET-CT图像Figure 6 Images of 18F-FDG PET-CT scan after 3 cycles of second-line therapy Red arrows show enlarged perigastric lymph nodes. 18F-FDG PET-CT, fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography. |
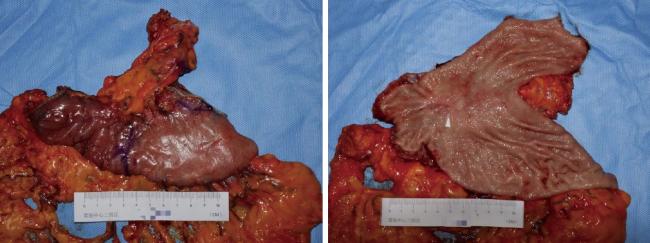
手术及病理结果:患者在我院行腹腔镜探查+开腹根治性远端胃大部切除术。术中探查见第8组淋巴结融合成团,与胰腺上缘及肝总动脉关系密切,无明显侵犯,成功完成R0切除。手术标本见图 8。术后病理回报:低分化肝样腺癌(ypT1bN1),Lauren分型为肠型。免疫组织化学染色结果:AFP(少数+)、磷脂酰肌醇蛋白聚糖-3(glypican-3,GPC-3)(+)、HER2(2+)、Sal样蛋白4(Sal-like protein 4,SALL4)(+)、pMMR、PD-L1 CPS 5分。
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
术后治疗:术后1个月患者相继行维迪西妥单抗+替雷利珠单抗+仑伐替尼方案治疗1周期、维迪西妥单抗+仑伐替尼治疗1周期,后因药物治疗耐受性差改为随访观察。
预后:患者术后1年半复查未见肿瘤复发。
2 讨论
HAS是一种兼具腺癌与肝细胞癌样分化特征的高度侵袭性肿瘤,其恶性程度高, 进展迅速,对常规化疗不敏感,且缺乏标准治疗方案。本文报道了1例初始不可切除的HAS患者,历经一线常规治疗失败后,通过基于分子特征的个体化强效联合方案成功实现转化并接受根治性手术,为这一罕见难治性肿瘤的治疗提供了思路。
本例患者初始接受基于奥沙利铂的化疗联合程序性死亡受体1(programmed death-1,PD-1)抑制剂的治疗,并后续联用曲妥珠单抗,结果疾病进展,这反映了HAS与普通胃腺癌的生物学差异。HAS基因组图谱分析显示,其较普通胃腺癌存在更明显的铂类耐药基因上调[2],这从机制上解释了为何以铂类为基础的常规化疗方案在该病中效果有限。尽管患者存在HER2扩增这一明确的治疗靶点,但传统的抗HER2单克隆抗体——曲妥珠单抗的应用并未很好控制肿瘤进展,首先,HAS的高度异质性意味着仅有部分肿瘤细胞依赖HER2信号通路,而曲妥珠单抗作为单纯的信号阻断剂,难以清除不依赖该通路的细胞亚群;其次,HAS常伴随其他驱动基因的改变,本例中同时存在c-MET的高表达,该通路的激活是已知的HER2靶向治疗耐药机制之一[3]。因此,对于HAS这类特殊亚型,套用普通胃腺癌的治疗模式可能收效甚微。
维迪西妥单抗作为一种新型HER2靶向抗体偶联药物(antibody-drug conjugate,ADC),在本例中逆转了肿瘤进展的趋势。维迪西妥单抗由人源化抗HER2免疫球蛋白G1(immunoglobulin G1,IgG1)单克隆抗体、可裂解的缬氨酸-瓜氨酸连接子以及微管抑制剂单甲基奥利司他汀E(monomethyl auristatin E,MMAE)组成。通过其抗体部分精准定位HER2阳性肿瘤细胞,并被内吞至细胞内,其携带的小分子毒素MMAE可直接破坏微管组装,导致细胞周期阻滞于G2/M期,最终诱导肿瘤细胞凋亡[4]。此外,维迪西妥单抗所采用的Val-Cit连接子具有膜通透性,释放的MMAE可扩散至邻近的肿瘤微环境,对HER2低表达甚至HER2阴性的肿瘤细胞亦产生细胞毒作用——即所谓的“旁观者效应”。这一特性对于HER2表达异质性较高的肿瘤(如胃癌)尤为重要,有助于实现更广泛的肿瘤细胞清除。研究显示,维迪西妥单抗对于HER2过表达的晚期胃癌患者具有显著疗效,不仅提高了治疗反应率,还延长了患者生存期[5]。本例患者在二线治疗中使用维迪西妥单抗联合仑伐替尼与替雷利珠单抗后,肿瘤负荷显著减轻,为后续手术创造了条件,充分体现了维迪西妥单抗在逆转HAS疾病进展中的作用。
仑伐替尼作为一种多靶点酪氨酸激酶抑制剂(tyrosine kinase inhibitor,TKI),在本例中也发挥了重要作用。其靶向血管生成相关受体(如血管内皮生长因子受体)和其他酪氨酸激酶致癌受体的机制,不仅能够抑制肿瘤新生血管的生成,还通过免疫调节作用进一步增强了抗肿瘤活性[6]。具体而言,仑伐替尼可以通过抑制免疫抑制性调节性T(regulatory T,Treg)细胞的功能,同时激活细胞毒性CD8+ T细胞,从而促进肿瘤微环境的免疫效应[7]。这种免疫调节作用,为肿瘤治疗提供了更强大的免疫支持。近年来,越来越多的研究表明,TKI与免疫检查点抑制剂联合使用可产生协同抗癌效果。仑伐替尼联合PD-1抗体的治疗策略在肝细胞癌、胃癌等多种实体瘤中均取得了较好疗效[8-9]。这种组合疗法的优势在于,仑伐替尼不仅通过血管靶向作用改善肿瘤血管正常化,还通过调控肿瘤微环境的免疫细胞成分,增强免疫检查点抑制剂的抗癌效应。
当前,HAS的治疗经验尚局限于个案报道,缺乏前瞻性临床试验的证据支持,本例的治疗成功为类似患者提供了重要参考。针对HAS生物学行为差、常规方案疗效差的特性,对于初始不可切除的局部晚期或转移性患者,应考虑在治疗伊始就采用基于分子特征的、更强效的联合方案,避免因治疗强度不足而错失转化时机。对于HER2表达且传统方案疗效不佳的病例,可以考虑联合使用ADC药物,其独特的杀伤机制为克服肿瘤异质性和旁路耐药提供了新武器。ADC药物联合抗血管生成TKI及免疫检查点抑制剂的“去化疗”或“弱化疗”强效方案,展现出了令人鼓舞的转化潜力,值得在HAS中进一步探索。未来,针对HAS的多中心前瞻性队列研究和转化研究将进一步阐明其驱动基因、耐药机制及与治疗反应的关系,从而最终建立基于分子分型的个体化精准治疗体系,改善这类预后不良患者的生存结局。