Journal of Peking University (Health Sciences) ›› 2021, Vol. 53 ›› Issue (6): 1133-1138. doi: 10.19723/j.issn.1671-167X.2021.06.021
Previous Articles Next Articles
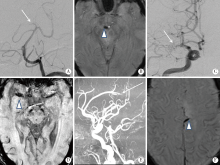
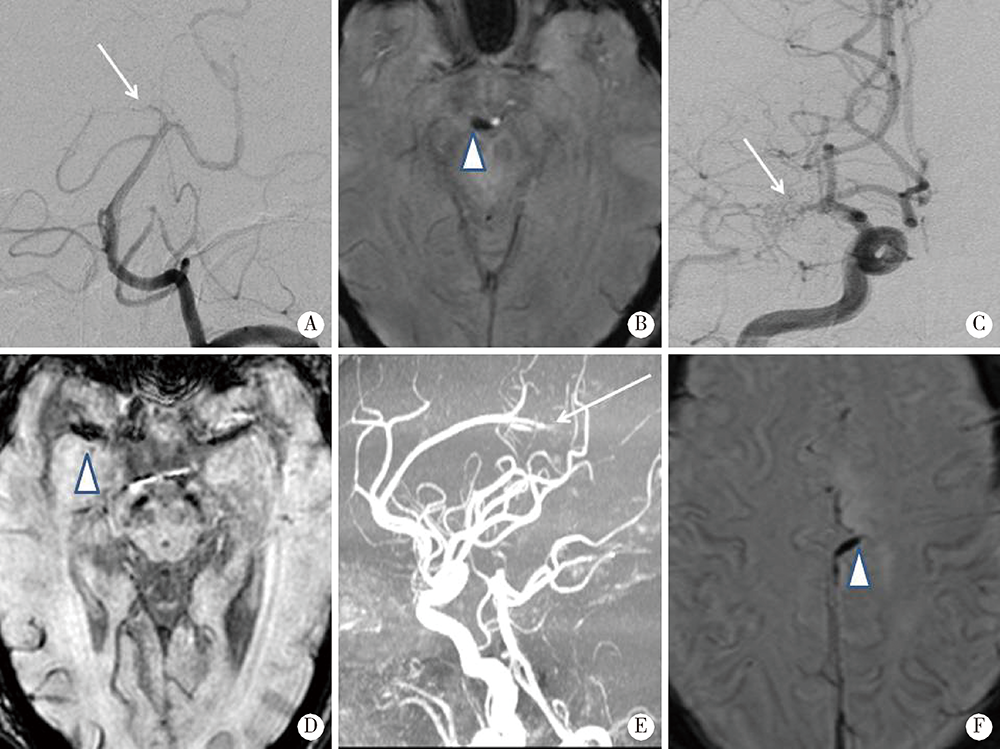
Susceptibility vessel sign in subacute stroke patients with large vessel occlusion
REN Guo-yong1,2,WU Xue-mei2, 1,LI Jie-yu1,SUN Wei-ping1,△( ),HUANG Yi-ning1
),HUANG Yi-ning1
- 1. Department of Neurology, Peking University First Hospital, Beijing 100034, China
2. Department of Neurology, General Hospital of Taiyuan Iron & Steel CO., LTD.(TISCO), Taiyuan 030003, China]
CLC Number:
- R741
| [1] |
Gorelick PB, Wong KS, Bae HJ, et al. Large artery intracranial occlusive disease: A large worldwide burden but a relatively neglected frontier[J]. Stroke, 2008, 39(8):2396-2399.
doi: 10.1161/STROKEAHA.107.505776 pmid: 18535283 |
| [2] |
Ornello R, Degan D, Tiseo C, et al. Distribution and temporal trends from 1993 to 2015 of ischemic stroke subtypes: A systematic review and meta-analysis[J]. Stroke, 2018, 49(4):814-819.
doi: 10.1161/STROKEAHA.117.020031 |
| [3] |
Tian C, Cao X, Wang J. Recanalisation therapy in patients with acute ischaemic stroke caused by large artery occlusion: Choice of therapeutic strategy according to underlying aetiological mechanism[J]. Stroke Vasc Neurol, 2017, 2(4):244-250.
doi: 10.1136/svn-2017-000090 |
| [4] |
Allibert R, Billon GC, Vuillier F, et al. Advantages of susceptibility-weighted magnetic resonance sequences in the visualization of intravascular thrombi in acute ischemic stroke[J]. Int J Stroke, 2014, 9(8):980-984.
doi: 10.1111/ijs.12373 pmid: 25319168 |
| [5] |
Cho KH, Kim JS, Kwon SU, et al. Significance of susceptibility vessel sign on T2*-weighted gradient echo imaging for identification of stroke subtypes[J]. Stroke, 2005, 36(11):2379-2383.
doi: 10.1161/01.STR.0000185932.73486.7a |
| [6] |
Horie N, Tateishi Y, Morikawa M, et al. Acute stroke with major intracranial vessel occlusion: Characteristics of cardioembolism and atherosclerosis-related in situ stenosis/occlusion[J]. J Clin Neurosci, 2016, 32(8):24-29.
doi: 10.1016/j.jocn.2015.12.043 |
| [7] |
Kang DW, Jeong HG, Kim DY, et al. Prediction of stroke subtype and recanalization using susceptibility vessel sign on susceptibility-weighted magnetic resonance imaging[J]. Stroke, 2017, 48(6):1554-1559.
doi: 10.1161/STROKEAHA.116.016217 |
| [8] |
Bourcier R, Derraz I, Delasalle B, et al. Susceptibility vessel sign and cardioembolic etiology in the THRACE trial[J]. Clin Neuroradiol, 2019, 29(4):685-692.
doi: 10.1007/s00062-018-0699-8 pmid: 29947813 |
| [9] |
Adams HP, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of org 10172 in acute stroke treatment[J]. Stroke, 1993, 24(1):35-41.
pmid: 7678184 |
| [10] |
Mori E, Yoneda Y, Tabuchi M, et al. Intravenous recombinant tissue plasminogen activator in acute carotid artery territory stroke[J]. Neurology, 1992, 42(5):976-982.
pmid: 1579252 |
| [11] |
Molina CA, Montaner J, Abilleira S, et al. Timing of spontaneous recanalization and risk of hemorrhagic transformation in acute cardioembolic stroke[J]. Stroke, 2001, 32(5):1079-1084.
pmid: 11340213 |
| [12] |
Fitzgerald S, Dai D, Wang S, et al. Platelet-rich emboli in cerebral large vessel occlusion are associated with a large artery atherosclerosis source[J]. Stroke, 2019, 50(7):1907-1910.
doi: 10.1161/STROKEAHA.118.024543 pmid: 31138084 |
| [13] |
Sato Y, Ishibashi-Ueda H, Iwakiri T, et al. Thrombus components in cardioembolic and atherothrombotic strokes[J]. Thromb Res, 2012, 130(2):278-280.
doi: 10.1016/j.thromres.2012.04.008 |
| [14] | 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国缺血性脑卒中和短暂性脑缺血发作二级预防指南2014[J]. 中华神经科杂志, 2015, 48(4):258-273. |
| [15] | Patel AR, Patel AR, Desai S. The underlying stroke etiology: A comparison of two classifications in a rural setup[J]. Cureus, 2019, 11(7):51-57. |
| [16] | Radbruch A, Mucke J, Schweser F, et al. Comparison of susceptibility weighted imaging and TOF-angiography for the detection of thrombi in acute stroke[J]. PLoS One, 2013, 8(5):634-639. |
| [1] | Huan YU,Ruo-tong YANG,Si-yue WANG,Jun-hui WU,Meng-ying WANG,Xue-ying QIN,Tao WU,Da-fang CHEN,Yi-qun WU,Yong-hua HU. Metformin use and risk of ischemic stroke in patients with type 2 diabetes: A cohort study [J]. Journal of Peking University (Health Sciences), 2023, 55(3): 456-464. |
| [2] | Yu-han DENG,Yong JIANG,Zi-yao WANG,Shuang LIU,Yu-xin WANG,Bao-hua LIU. Long short-term memory and Logistic regression for mortality risk prediction of intensive care unit patients with stroke [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 458-467. |
| [3] | Ruo-tong YANG,Meng-ying WANG,Chun-nan LI,Huan YU,Xiao-wen WANG,Jun-hui WU,Si-yue WANG,Jia-ting WANG,Da-fang CHEN,Tao WU,Yong-hua HU. Interaction between ischemic stroke risk loci identified by genome-wide association studies and sleep habits [J]. Journal of Peking University (Health Sciences), 2022, 54(3): 412-420. |
| [4] | WU Jun-hui,WU Yi-qun,WU Yao,WANG Zi-jing,WU Tao,QIN Xue-ying,WANG Meng-ying,WANG Xiao-wen,WANG Jia-ting,HU Yong-hua. Incidence and risk factors of ischemic stroke in patients with type 2 diabetes among urban workers in Beijing, China [J]. Journal of Peking University (Health Sciences), 2022, 54(2): 249-254. |
| [5] | Ya-fei LIU,Lin-lin SONG,Mao-wei XING,Li-xin CAI,Dong-xin WANG. Comparison of pulse pressure variation, stroke volume variation, and plethysmographic variability index in pediatric patients undergoing craniotomy [J]. Journal of Peking University (Health Sciences), 2021, 53(5): 946-951. |
| [6] | Yue HOU,Xu-tong ZHAO,Zhi-ying XIE,Yun YUAN,Zhao-xia WANG. Mitochondrial encephalopathy, lactic acidosis and stroke-like episodes / myoclonus epilepsy with ragged-red fibers /Leigh overlap syndrome caused by mitochondrial DNA 8344A>G mutation [J]. Journal of Peking University (Health Sciences), 2020, 52(5): 851-855. |
| [7] | Xun TANG,Du-dan ZHANG,Xiao-fei LIU,Qiu-ping LIU,Yang CAO,Na LI,Shao-ping HUANG,Hui-dong DOU,Pei GAO,Yong-hua HU. Application of the China-PAR stroke risk equations in a rural northern Chinese population [J]. Journal of Peking University (Health Sciences), 2020, 52(3): 444-450. |
| [8] | Zi-chang JIA,Huan-ju BIAN,Xuan LI,Jing-yuan LUAN,Chang-ming WANG,Qi-jia LIU,Jin-tao HAN. Application of Neuroform EZ stent in the treatment of severe intracranial arterial stenosis with complex symptomatic [J]. Journal of Peking University(Health Sciences), 2019, 51(5): 835-839. |
| [9] | Zi-chang JIA,Xuan LI,Xiao-gang LI,Xiang-zhu ZENG,Jing-yuan LUAN,Chang-ming WANG,Jin-tao HAN. Mechanical thrombectomy treatment in patients with acute ischemic stroke: a single center study [J]. Journal of Peking University(Health Sciences), 2019, 51(2): 256-259. |
| [10] | SUN Zhuo-nan, MENG Xiu-li, WANG Jun, GUO Xiang-yang, HAN Jin-tao, QI Qiang. Perioperative stroke effectively treated by an acute stroke team including anesthesia department: a case report [J]. Journal of Peking University(Health Sciences), 2017, 49(6): 1090-1094. |
| [11] | XIAO Tian-yi, LIU Yan, LI Ji-lai, WANG Rui-tong, DU Ji-chen. Diagnostic value of carotid atherosclerosis score for ischemic stroke [J]. Journal of Peking University(Health Sciences), 2016, 48(6): 1000-1005. |
| [12] | YU Can-qing, CHEN Yi-ping, LV Jun, GUO Yu, Paul SHERLIKER, BIAN Zheng, ZHOU Hui-yan, TAN Yun-long, CHEN Jun-shi, CHEN Zheng-ming, LI Li-ming1. Major depressive disorder in relation with coronary heart disease and stroke in Chinese adults aged 30-79 years [J]. Journal of Peking University(Health Sciences), 2016, 48(3): 465-471. |
| [13] | SHAN Jiao, LI Hong-yu, LIU Guo-feng, YANG Xuan, DONG Wei, JIAN Wei-yan, DENG Fu-rong, GUO Xin-biao. Effect of air pollution on health service demand of the elderly and middle-age patients with hypertension, cardiovascular and cerebrovascular diseases: based on analysis of data from CHARLS [J]. Journal of Peking University(Health Sciences), 2016, 48(3): 460-464. |
| [14] | YANG Cheng, ZHANG Yu-qi, TANG Xun, GAO Pei, WEI Chen-lu, HU Yong-hua. Retrospective cohort study for the impact on readmission of patients with ischemic stroke after treatment of aspirin plus clopidogrel or aspirin mono-therapy [J]. Journal of Peking University(Health Sciences), 2016, 48(3): 442-447. |
|
||